Wrist Muscles
Introduction
The muscles that originate and are primarily found in the forearm are referred to as wrist muscles. The muscle belly is usually found in the forearm, and wrist movements are made possible via a lengthy tendon that crosses the wrist joint and connects to a hand bone. The wrist can move in four different ways: flexion, extension, radial deviation, and ulnar deviation.
- Many everyday tasks involve the wrist, which is prone to various degenerative conditions and serious injuries.
- The hand can move in multiple directions relative to the forearm due to the complex structure of the wrist joint. Understanding how the wrist functions biomechanically is essential from both a scientific and clinical angle. It is important to understand the mechanics of the carpal bones, especially the role of soft tissues, to diagnose and treat diseases affecting the wrist.
- For instance, ligaments are a key component in this process.
- It is important to understand the biomechanics of wrist movement, which refers to the movements necessary for performing everyday tasks. Studying the causes and effects of injuries and surgical treatments also requires an understanding of how the wrist behaves under normal and abnormal conditions. This knowledge is vital for how wrist conditions are currently managed.
- Biomechanical models can be used as tools in clinical settings to evaluate the wrist joint both before and after surgery.
- Currently, clinical decision-making for surgery typically relies on the current state of the wrist and its appearance on imaging tests. Moreover, arthroscopic procedures used for a definitive diagnosis are usually secondary to other imaging methods. Information obtained from in vivo biomechanical research is necessary to support the development of surgical simulation and planning tools for wrist procedures or the implantation of artificial joints.
- These tools help in optimising treatment by reducing the stress on the joint, preventing the development of harmful changes such as osteoarthritis, and increasing the lifespan of implants. It has been suggested that using customised models, biomechanical simulations, load analysis, and appropriate boundary conditions for implants is beneficial. However, due to the complexity of simulating such a joint system, this area has not received widespread attention.
- The wrist joint consists of eight distinct carpal bones positioned between the five metacarpal bones and the forearm bones, the ulna and radius.
- These carpal bones are arranged in two rows: the proximal carpal row (PCR), which includes the scaphoid, lunate, triquetrum, and pisiform, from the radial to the ulnar side; and the distal carpal row (DCR), which includes the trapezium, trapezoid, capitate, and hamate, also from radial to ulnar.
- Strong ligaments connect the bones of the DCR, effectively making them function as a single unit.
- This functional unit moves in response to the muscle activity of the forearm due to its tightly bound connection to the base of the metacarpal bones. There is very little movement between the bones of the wrist, as they are held together tightly by several ligaments.
- In contrast, the PCR shows different movement patterns.
- The entire row moves in the same direction, but there is noticeable movement between individual bones. During wrist flexion and extension, the PCR moves along with the DCR. However, during radial and ulnar deviation, the movement continues. The PCR acts as an intercalated segment between the radius and the DCR.
- None of the muscles that control the wrist are attached directly to the PCR.
- Instead, all tendons involved in wrist movement attach distally. The movement of the PCR depends entirely on the mechanical forces from the surrounding joints. Therefore, any movement of the wrist in any direction must originate from the DCR. Movement in the PCR begins only when the extrinsic ligaments that cross the midcarpal joint become taut, and the force applied to the PCR overcomes the frictional forces between the articular segments and the resistance of opposing muscle forces. The wrist relies on its unique bone shape, its interactions with adjacent bones, and its extrinsic and intrinsic ligaments.
- The triangular fibrocartilage complex (TFCC) is a critical load-bearing structure.
- It is located on the medial side of the wrist, between the lunate, triquetrum, and the ulnar head. The TFCC is made up of a triangular fibrocartilage disc, the ulnomeniscal homologue, the ulnar collateral ligament, the dorsal and palmar radio-ulnar ligaments, the base of the extensor carpi ulnaris tendon sheath, and the ulnolunate and ulnotriquetral parts of the palmar ulnocarpal ligament. Its primary function is to stabilise the ulnar side of the wrist. It also prevents ulnocarpal impaction by transmitting and distributing the axial load from the carpus to the ulna. It plays a key role in enabling movement at the wrist.
- The wrist joint is surrounded by an extensive and complex network of ligaments, with a total of 33 intra-articular and intra-capsular ligaments.
- Descriptions of the wrist ligaments vary significantly in the literature, which can make the anatomy difficult to understand. This is further complicated by the use of different classifications, names, and descriptions in various sources. The structure and function of the carpal ligaments have been the subject of many published studies, with more recent comprehensive research helping to clarify the wrist’s ligamentous anatomy.
- Ligaments are essential in guiding and limiting the movement of the carpal bones during hand movement.
- They include volar and dorsal ligaments, as well as extrinsic ligaments that connect the carpal bones to the radius or metacarpals. Intrinsic ligaments originate and are attached to the carpal bones themselves.
- Extrinsic Carpal Ligaments
- The extrinsic ligamentous system provides support to the carpus and prevents it from moving in a single direction.
- These ligaments connect the carpal bones to the radius or metacarpals. The functional role of extrinsic wrist ligaments in carpal movement is not yet fully understood. Some of the extrinsic wrist ligaments include the dorsal intercarpal (DIC), dorsal radiocarpal (DRC), radioscaphocapitate (RSC), long radiolunate (LRL), short radiolunate (SRL), ulnocapitate, and ulnocapitate ligaments. The extrinsic ligaments are part of a complex network, and the direction of movement affects how these different parts of the ligaments are stretched.
- Intrinsic Carpal Ligaments
- The intrinsic ligaments start and end within the carpus.
- Most carpal bones are directly connected to their adjacent bones through interosseous ligaments. The lunate and capitate bones do not have direct ligamentous connections. Most attention is given to the ligaments that connect the bones of the PCR, due to their movement. These include the scapholunate interosseous ligament (SLIL) and the lunotriquetral interosseous ligament.
Wrist Muscles
Six Primary Wrist Flexing Muscles
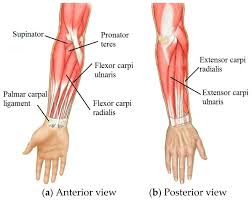
- The wrist is flexed by six major muscles. These muscles are the palmaris longus, flexor carpus radialis, and flexor carpi ulnaris. These three muscles start on the humerus, go across the forearm, pass through the wrist via tendons, and end in the hand’s bones. The tendons of the other three muscles—the flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus—attach to the phalanges, or finger bones, and begin in the forearm. These muscles can assist with both wrist flexion and the flexion of the finger or thumb to which they attach because of where they insert.
- Overall Motion
The wrist is typically thought of as a universal joint with two degrees of freedom (DOF). The FE-axis and RUD-axis are two orthogonal anatomical axes that have historically been used to determine motion. Instead of the typical six DOF provided for the standard kinematic analysis, two DOF can be used to represent the motion of the hand to the forearm. - When off-centre forces are applied, the DCR bones move as a single unit. This is comparable to a scale’s beam passing through the capitate’s head on an instantaneous axis. The radiocarpal and midcarpal joints equally share FE motions (sagittal plane).
- Wrist motion during everyday tasks mimics the dart thrower’s motion, from ulnar deviation and flexion to radial deviation and extension, to complete the motion behaviour. One common wrist motion utilised in daily activities is the dart-thrower’s arc.
- The presence of the wrist’s “centre of rotation” is still up for debate. For both FE and RUD, if one exists, it will be located in the head of the capitate.
The forearm contains the muscles that act on the wrist joint. Just the muscular tendon that inserts into the hand or fingers after passing through the wrist joint. The carpus and PCR are not directly connected by tendons. The wrist is flexed by the muscles on the palmar side and extended by the muscles on the dorsal side of the forearm. The motion of the wrist bones is solely dependent on the mechanical forces generated by the surrounding articulations. The relationships between the ligaments and the shape of the carpal bones are essential to physiological carpal biomechanics. The mobility of the wrist bones is intricate and happens in three dimensions. A change in intercarpal mobility is the cause of many wrist issues. Intercarpal motion is still not fully understood - Six of the forearm’s many muscles are implanted at the base of the metacarpal bones or the carpal bones (at the DCR). Moments about the FE and RU axes are influenced by these six muscles. They are exclusively focused on the wrist and consist of the palmaris longus (PL), flexor carpi radialis (FCR), and flexor carpi ulnaris (FCU) on the anterior side.
- The extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), and extensor carpi ulnaris (ECU) are the three main wrist extensor muscles on the posterior side. Their moment arms around the wrist axes are bigger. The PL, FCU, and FCR are primarily responsible for flexion. The flexor digitorum superficialis muscle provides support for the move. The ECRL, ECRB, and ECU are the primary producers of extension. The extensor digitorum muscle will help them. The ECU and FCU generate adduction. The FCR, ECRL, and ECRB are responsible for abduction. The abductor pollicis longus muscle provides assistance for it.
- The primary wrist muscles that regulate wrist flexion, extension, and deviation are the flexor muscles on the anterior (palm) side of the forearm and the extensor muscles on the posterior (back) side. The flexor carpi radialis and ulnaris for flexion and the extensor carpi radialis longus, brevis, and ulnaris for extension are important examples. Many of these muscles start in the forearm and attach to the bones of the hand through tendons that go through the wrist.
Wrist flexor muscles
- The front (front) side of the forearm contains these muscles, which are in charge of bending the wrist down towards the palm.
Wrist flexion and radial deviation (bending towards the thumb) are facilitated by the flexor carpi radialis.
Flexor carpi ulnaris: Facilitates ulnar deviation (bending towards the pinky finger) and wrist flexion. - Palmaris longus: Tightens the palm’s skin and aids in wrist flexion.
Flexor digitorum superficialis: Helps with wrist flexion but mostly flexes the fingers.
Flexor digitorum profundus: A deep muscle that helps in wrist flexion and finger flexion.
Flexor pollicis longus: Promotes wrist flexion and thumb flexion.
Wrist extensor muscles
- The wrist is bent upward by these muscles, which are found on the posterior (back) side of the forearm.
Extensor carpi radialis longus: This muscle extends and aids in wrist abduction.
The wrist is extended and aided in abduction by the extensor carpi radialis brevis. - Extensor carpi ulnaris: Assists in adducting (bending in) the wrist.
Extensor digitorum: Promotes wrist extension and finger extension.
Extensor digiti minimi: Helps extend the wrist and extends the little finger.
Extensor indicis: Helps extend the wrist and extends the index finger.
The abductor pollicis longus aids in wrist extension and thumb abduction.
The thumb is extended by the extensor pollicis brevis.
The thumb is extended by the extensor pollicis longus.
Biomechanics of the Wrist
Between the hand and forearm, the wrist transmits force. Together, the flexors and extensors stabilise the wrist during a variety of motions. For instance:
Wrist extensors contract isometrically to fix the wrist in a slightly extended position when gripping firmly.
Radial and ulnar deviation occur in a coordinated way during throwing or racquet sports.
Coupled movements
There is typically a small ulnar deviation in conjunction with wrist flexion.
There is a small radial deviation when the wrist is extended.
Smooth wrist motion requires coordinated muscle recruitment.
Wrist Motion
- Except for the pisiform, a sesamoid bone, and the forearm, seven carpal bones interact intricately to provide wrist mobility. Although each of them has a distinct motion axis, they are all dependent on the carpal alignment with the distal radius and the location of neighbouring carpal components. Generally speaking, there is no motion between the DCR and the metacarpals, minimal motion between the PCR and the DCR, and noticeable motion between the radius and the PCR
- Carpal motion varies within each row, especially within the PCR, from a functional perspective. The DCR bones work as a single unit. The triquetrum tends to extend, the scaphoid to flex, and the DCR to spin towards pronation under an axial force. Due to the interlocking of the articular surfaces and the dense ligamentous connections between the bases of the metacarpals and the DCR bones, this unit also comprises the metacarpals. The DRC moves in the same manner as the third metacarpal flexes or expands.
- The mobility pattern of the PCR bones is distinct. Compared to the DCR, the PCR moves more frequently between the individual bones. The triquetrum, scaphoid, and lunate exhibit the least range of motion (ROM). Global wrist flexion causes the PCR bones to flex, while global wrist extension causes them to extend. When the wrist is extended globally, the lunate tends to pronate and the scaphoid to supinate. During global wrist flexion, the opposite event takes place. The PCR bones exhibit a distinct motion characteristic in the case of global wrist RUD that is best characterised as reciprocal. Palmar flexion and secondary, variable counter-rotation of the PCR bones towards the ulnar edge of the wrist are caused by radial deviation.
- A primary extension and a secondary, erratic counter-rotation towards the wrist’s radial margin result from ulnar deviation. During RUD, the PCR bones exhibit the same longitudinal motion behaviour that they do during wrist FE. As a result, the PCR bones palmarflex and dorsiflex, respectively, to accommodate wrist RUD.
- Using an optical tracking system, Patterson et al. reported that when the wrist was moved passively with a constant force applied to the tendons, or actively via the extensor and flexor tendons, there were no appreciable variations in carpal bone motion (FE and RUD). They came to the conclusion that active and passive wrist movements have identical carpal bone kinematics in a healthy joint. Preventing pathological alterations in the wrist requires a thorough grasp of normal carpal anatomy and functioning.
Conditions
- Cyclists’ Palsy and Carpal Tunnel Syndrome
- De Quatrain’s Carpal Instability and Wrist Sprain
- Colles Fracture
- Smith’s Fracture
- Scaphoid Fracture
- Hand and Wrist Osteoarthritis
- Complex Rheumatoid Arthritis Syndrome of Regional Pain
- Injuries to the Triangular Fibrocartilage Complex
- The Thumb of the Gamekeeper
- Skier’s Thumb Instability of the Moon
- Hamate Fracture
- Claw Hand, Benediction Hand, and Ape Hand
- Dupuytren’s Agreement
- Fractures of the Metacarpal
- Damage to the Extensor Mechanism
- Flexor Tendon Injuries
- Impaction syndrome of the ulnocarpal joint
- Dissociation and tearing of the lunotriquetral ligament
Sprains of the Wrist
Damage to a ligament is known as a sprain-type injury. The wrist and palm are an intricate structure made up of tiny bones joined by ligaments. People naturally try to reach forward to catch themselves when they fall forward, whether jogging, playing sports, or just tripping. Upon contact, this extended-wrist, outstretched-arm position may result in wrist ligament tears.
Fractured wrist
The most common wrist fracture occurs in the same way as a wrist sprain (an outstretched arm with the wrist extended). Automobile accidents also frequently result in this fracture. There are eight tiny bones in the wrist, but the scaphoid bone is usually the most likely to be fractured. Until an X-ray is taken, this injury may appear to be a simple sprain, depending on the extent of the damage.
Rehabilitation of Wrist Muscles
- strengthening activities
- Curl your wrists (flexors)
- Wrist curls in reverse (extensors)
- Exercises for radial and ulnar deviation
- Strengthening the grip
- Resistance exercises using a TheraBand
- Extending
- Stretching the wrist flexors
- Stretching the wrist extensor
- Gliding of the thumb tendon (for APL/EPB)
- Practical Instruction
- Sports-specific exercises
- Plyometric wrist exercises
- Exercises for hand-eye coordination
- Hand therapy
- Release of soft tissues
- Radius, ulna, and carpal bone mobilisation
- Neural glides for radial, ulnar, and median nerves
Importance of Wrist Muscle Balance
- It’s crucial to have balanced flexor and extensor strength to prevent:
- Overuse injuries
- Tendinitis
- Weakness in grip
- Insufficient stability of the wrist
- Shoulder or elbow muscles frequently compensate for an imbalance, resulting in a cascade of dysfunction.
FAQs:
What are common wrist injuries?
Common wrist injuries include sprains, strains, fractures (like the distal radius and scaphoid), and conditions from repetitive stress such as tendonitis and carpal tunnel syndrome. Acute injuries often result from a fall on an outstretched hand, while overuse injuries are linked to repetitive motions
What is the difference between muscle pain and tendon pain?
Muscle pain is a dull ache from muscle contraction, while tendon pain is a sharp ache from the tissue connecting muscle to bone, often caused by overuse or a tear. Muscles are more flexible and have a blood supply, which can lead to faster healing, whereas tendons are rope-like and less elastic, making them prone to inflammation (tendinitis) and longer healing times, sometimes requiring surgery.
Conclusion
Functional activities, fine motor tasks, and sports performance all depend on the wrist muscles. Injury prevention, diagnosis, and rehabilitation depend on an understanding of their anatomy, nerve supply, and biomechanical function.
For stability and accurate movement, flexors, extensors, and deviation muscles must cooperate. Clinicians and physiotherapists who have a thorough understanding of wrist muscles are better able to create treatment plans and exercise regimens for patients with wrist pain, instability, or sports-related injuries.
References
- Vaquero-Picado A, Barco R, Antuña SA. Lateral epicondylitis of the elbow. EFORT Open Rev. 2016 Nov;1(11):391-397.
- Neumann DA. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 3rd ed. St. Louis: Elsevier; 2017.
- Palastanga N, Soames R. Anatomy and Human Movement. 6th ed. Edinburgh: Elsevier; 2012.
- Levangie PK, Norkin CC. Joint Structure and Function: A Comprehensive Analysis. 6th ed. Philadelphia: F.A. Davis; 2020.
- Floyd RT. Manual of Structural Kinesiology. 20th ed. New York: McGraw-Hill; 2018.
- Michlovitz S, LaStayo P. Wrist rehabilitation after injury. J Hand Ther. 2015;28(2):137-45.
- Brigham C, Leffert R. Wrist splinting and therapeutic exercise. Phys Ther. 1995;75(10):881-9.
One Comment