Radial Tunnel Syndrome
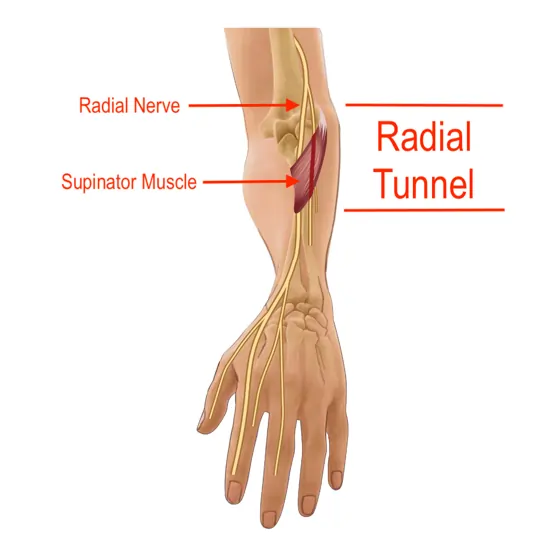
Radial tunnel syndrome is a compressive neuropathy affecting the posterior interosseus nerve (PIN) within the radial tunnel. Many of the motor activities in your arm, such as forearm rotation and wrist and finger straightening, are governed by the radial nerve.
These comparatively easy actions can become unpleasant and challenging due to radial tunnel syndrome, which is caused by compression of the nerve as it passes through the radial tunnel in your forearm. Pain without motor or sensory pathology is one of the symptoms.
Occupational therapy, rest, and in certain situations, surgery, can all be used as treatments. Radial tunnel syndrome, however, is rapidly treatable. Your arm could be pain-free again in around a month with the correct care.
What Is Radial Tunnel Syndrome?
- Radial tunnel syndrome may occur from a pinched or squeezed nerve as it enters the radial tunnel. This causes excessive pressure on your radial nerve, which often leads to chronic discomfort.
- Your radial nerve travels down your arm from its origin in your neck. It regulates the triceps, a muscle located in the upper arm. The space beneath your elbow is called the radial tunnel. After passing through this tunnel made of bone and muscle, your radial nerve descends to your wrist.
- Anywhere in your arm where the radial nerve is pinched, might result in discomfort and paralysis. The pinching is the outcome of a few routine everyday tasks.
Anytime you use your arm muscles to move anything, you run the risk of irritating your radial nerve by:
- Pulling
- Pressing,
- Grabbing.
Your radial nerve may also become irritated by using your hands and wrists. For example, overuse and radial tunnel syndrome may result from doing specific motions frequently for your job or a regular hobby.
Anatomy of the Radial Nerve
- The radial nerve innervates the triceps muscle, wrist extensors, and extensors of the fingers and thumb. It starts through the posterior cord of the brachial plexus. Just proximal to the superior boundary of the superficial layer of the supinator muscle, the nerve splits into superficial and deep branches (the arcade of Frohse).
- Along its distribution, PIN also contains tiny myelinated (group IIA) afferent fibers from muscle and unmyelinated (group IV) afferent fibers from the wrist capsule. Since nociception and pain have been linked to group IV unmyelinated muscle fibers, this could account for the patient’s sensory complaints in cases of pure PIN engagement.
- From the radial head to the inferior border of the supinator muscle, there is an anatomic radial tunnel. The supinator, brachioradialis, extensor carpi radialis longus, and extensor carpi radialis brevis muscles define the boundaries. When the radiohumeral (RH) joint is crossed by the deep branch of the radial nerve (DBRN), the radial tunnel starts. The tunnel closes at the distal margin of the superficial supinator when the DBRN changes into the PIN. Proximally located structures in the radial tunnel have the potential to compress the DBRN.
- Superficially extending fibrous fascial bands to the radial head.
- The leash of Henry is the radial recurrent artery and its vena comitans.
- The extensor carpi radialis brevis’s fibrous border (ECRB).
- The distal, usually fibrous, edge of the supinator muscle; and the proximal edge of the supinator.
- The arcade of Frohse, a fibrous arch near the proximal margin of the supinator, is the most often occurring point of compression. The radial nerve bifurcation and the supinator muscle are used as landmarks in previous DBRN studies. Some estimate the distance between the radial nerve bifurcation and the proximal and distal edges of the supinator muscle using the radiohumeral joint line as a reference point. Regarding a surgical technique, none has established the supinator’s DBRN’s entry and exit sites in connection to visible bone landmarks.
Causes of the Radial Tunnel Syndrome
Your radial nerve passes beneath facial bands, which are tissue fibers that encircle, divide, or tie together muscles, organs, and other soft structures in your body, as it passes through the radial tunnel beneath your elbow. This disorder is caused by excessive pressure on the nerve resulting from inflammation of the radial tunnel and all its components.
Several factors can lead to this compression, such as:
- Repetitive actions: The radial nerve and surrounding tissues can get stressed by repetitive gripping, twisting, or strong pronation and supination of the forearm. This can cause discomfort and compression. Examples include playing certain sports like tennis or basketball, using tools like paintbrushes or screwdrivers, and doing manual labor.
- Direct trauma: The radial nerve can be compressed by a direct hit to the outside of the elbow or forearm, such as one received in a fall or when playing contact sports. This can result in swelling and inflammation.
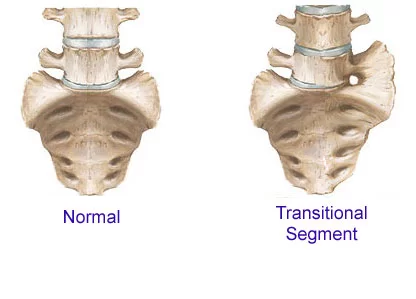
- Anatomical variations: Even in the absence of damage or repetitive activity, some people may naturally have tighter muscle bands or fibrous structures in the forearm, which can compress the nerve.
- Swelling and inflammation: Rheumatoid arthritis, fluid retention, and overuse traumas are a few conditions that can result in swelling or inflammation in the forearm. These conditions can also compress the radial nerve.
- Cysts or tumors: Noncancerous growths in the forearm, such as ganglion cysts or lipomas, can push on the nerve and cause problems.
Symptoms of the Radial Tunnel Syndrome
The hallmark signs of radial tunnel syndrome are forearm pain and weakness. The back of your hand hurts is one of the additional symptoms.
- A tender area directly below your elbow.
- Soreness that worsens with wrist rotation.
- Soreness that worsens when you reach out with your fingers.
- The outer edge of your elbow hurts.
- A hard time holding stuff.
- Difficulty moving or lifting objects.
- Having trouble extending your wrist.
The symptoms of radial tunnel syndrome vary from person to person. There will be those who have moderate symptoms and those who have more severe ones. It is advisable to speak with a medical practitioner about any symptoms you may have experienced.
Risk Factors of the Radial Tunnel Syndrome
- The age group of 30 to 50 is the most common for radial tunnel syndrome cases. Additionally, women are far more prone than men to have this illness.
- You may be more susceptible to radial tunnel syndrome if you have certain conditions, such as weak and flexed arms and wrists.
- They are not properly warming up before engaging in physical activity.
- Diabetes.
- The thyroid gland is underactive.
- Tumors or lumps in your arm that are ganglion cysts.
- Fluid or swelling in your arm.
- Inflammation of the radial nerve.
Diagnosis of the Radial Tunnel Syndrome
Radial tunnel syndrome diagnosis includes a thorough medical history, a physical examination, and possibly some more testing to rule out other illnesses.
Medical history:
Your physician will inquire about:
- Your symptoms, where they hurt, how bad they are, and how long they last.
- Any recent physical exertion or injuries that could have contributed to the pain.
- Your profession and interests.
- Any further health issues you may have.
Physical assessment:
- During the physical examination, your hand, forearm, and elbow will be examined. Your physician will:
- Check for any discomfort, redness, or swelling.
- Check the range of motion in your fingers and wrists.
- Assess the strength of your hand and wrist muscles.
- Use particular tests, including the reverse Finkelstein test and the Frosi sign, to evaluate the PIN nerve.
- Finkelstein test: In this test, you bend your wrist down towards your palm and use the other hand to press your thumb against your forearm. The thumb and base of the index finger may hurt, which could be a sign of radial tunnel syndrome.
- Resisted Wrist and Finger Extension: Extending your wrists and fingers against your doctor’s mild resistance is known as “resisted wrist and finger extension.” During this movement, weakness or pain may be an indication of nerve compression.
Further testing: Although there isn’t a single, conclusive test for radial tunnel syndrome, your doctor may in some circumstances advise further testing to rule out other disorders that present with comparable symptoms. These examinations could consist of:
- X-rays: To rule out anomalies in the bone, such as fractures.
- MRI scans: To view the forearm’s soft tissues and spot any anomalies that might be squeezing the nerve.
- Electromyography (EMG) and nerve conduction studies (NCS): To evaluate nerve function, two tests are used to monitor the electrical activity of the muscles and nerves: electromyography (EMG) and nerve conduction studies (NCS). These tests, however, are not always helpful in identifying radial tunnel syndrome since they can provide normal results even in cases when the nerve is pinched.
Differential Diagnosis of the Radial Tunnel Syndrome
Radial tunnel syndrome can present with symptoms of multiple different disorders, a precise diagnosis is essential for appropriate therapy. A medical practitioner may take into account the following primary disorders when making a differential diagnosis of radial tunnel syndrome:
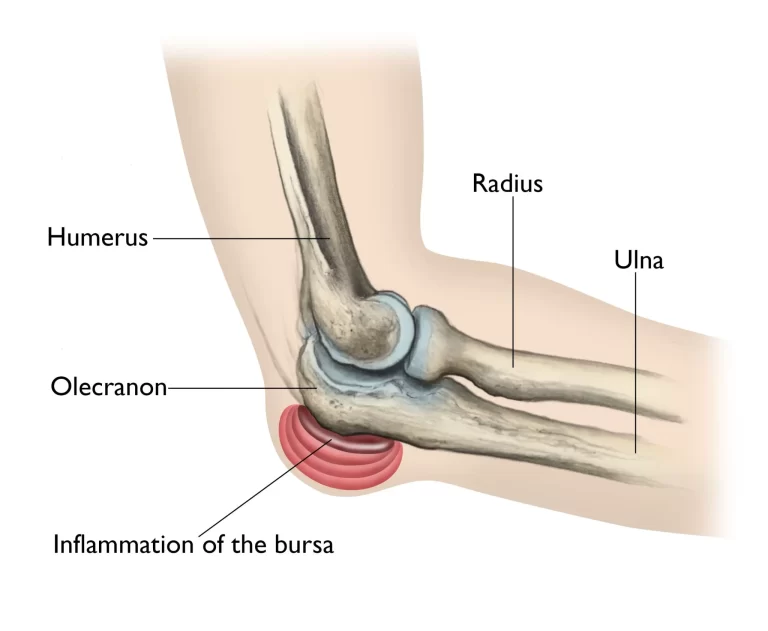
- Lateral epicondylitis, often known as tennis elbow, is characterized by pain and soreness on the elbow’s exterior, which can occasionally spread to the forearm. In contrast to radial tunnel syndrome, lateral epicondylitis pain usually affects the elbow joint rather than the wrist or hand.
Differentiating between the two conditions can be aided by specific tests, such as resisted wrist extension with the elbow straight. - Compression syndrome of the posterior interosseous nerve (PIN): This condition is comparable to radial tunnel syndrome, except it affects the PIN closer to the wrist. The thumb, index, and middle fingers can all experience pain, weakness, and numbness as common symptoms. Yet to identify the exact location of the compression, certain physical examination techniques like EMG/NCS studies could be used.
- Cervical Stenosis: A narrowing of the spinal canal in the neck, known as cervical stenosis, can compress the spinal cord and nerve roots. Like radial tunnel syndrome, cervical stenosis can produce discomfort, weakness, numbness, and tingling in the arm and hand. On the other hand, cervical stenosis frequently causes symptoms in the arm and leg on the same side, along with headaches, neck pain, and trouble balancing. Cervical stenosis diagnosis requires imaging examinations of the cervical spine, such as MRIs or X-rays.
- Cervical Foraminal Stenosis: A particular kind of cervical stenosis known as cervical foraminal stenosis is characterized by narrowing in the foramina—the apertures through which nerve roots leave the spinal canal. Symptoms in the arm and hand may resemble radial tunnel syndrome, such as discomfort, weakness, numbness, and tingling, similar to cervical stenosis. However, the distribution of symptoms varies depending on the precise location of the damaged nerve root and may not be the same as radial tunnel syndrome. Accurate diagnosis depends on imaging studies and maybe EMG/NCS testing.
Treatment And Management for the Radial Tunnel Syndrome
Radial tunnel syndrome is treated conservatively at first, with the goals of reducing inflammation, relieving pain, and halting additional nerve injury. Surgery could be considered if these methods don’t work. Below is a summary of the available alternatives for treatment and management:
Conservative Treatment
- Rest: It’s important to avoid activities that increase the symptoms. This could involve switching to other tools, altering work methods, or temporarily cutting back on sporting activities.
- Immobilization: For a brief time, putting on an elbow or wrist splint might assist limit movement and encourage recovery.
- Applying warm compresses or ice packs to the injured area can help reduce pain and inflammation. This is known as ice or heat therapy.
- Nonsteroidal anti-inflammatory medicines (NSAIDs), such as ibuprofen or naproxen, are available over the counter and can be used to treat pain and inflammation.
- Physical therapy: To promote improved nerve function and avoid further compression, a physical therapist might create a program to increase muscular strength, flexibility, and nerve gliding.
Other options:
- Corticosteroid injections: Because of the possible adverse effects, corticosteroid injections should not be used frequently. However, they can offer more focused pain relief and reduce inflammation when administered directly into the area around the nerve.
- Ultrasound therapy: Although more research is needed to see how helpful this treatment is for radial tunnel syndrome, it employs sound waves to encourage healing and reduce inflammation.
Non-Conservative Treatment
After a fair trial period (usually three to six months), if conservative methods are not able to provide a noticeable improvement, surgery may be considered. By releasing any structures that are compressing the PIN, surgery aims to decompress the nerve. This may entail:
- Endoscopic surgery: A minimally invasive technique to access and release a nerve that uses a camera and tiny equipment.
- Open surgery: A more conventional method of accessing and releasing the nerve that involves a bigger incision.
Physical therapy for the Radial Tunnel Syndrome
For both conservative treatment and post-surgical rehabilitation, physical therapy is essential in controlling radial tunnel syndrome. In this way, physical therapists can assist:
conservative handling
- Reducing pain and inflammation: Physical therapists can manage pain and inflammation using a variety of approaches, including manual therapy, therapeutic ultrasonography (though more study is needed to determine its long-term usefulness), and modalities like ice or heat therapy.
- Increasing range of motion and flexibility: Improving flexibility and range of motion: Compression may result from taut radial nerve-surrounded muscles and tissues. The forearm and wrist can be made more flexible using gentle stretches and mobilization procedures, which will relieve pressure on the nerve.
- Exercises for Strengthening: By building up the hand and forearm muscles, you can support the surrounding tissues and enhance joint stability, which will stop more nerve compression. Depending on the demands of the individual, exercises may focus on particular muscle groups.
- Exercises for nerve gliding: These enhance the nerve’s ability to move easily through surrounding tissues. This may lessen irritability and encourage recovery. As an illustration, consider slowly stretching and mobilizing the nerve by moving the wrist and arm in particular directions.
- Education and activity modification: To stop additional nerve strain and encourage healing, physical therapists can teach you about good posture, body mechanics, and activity modification strategies.
Your healthcare provider will choose a customized treatment plan based on your preferences, general health, and the severity and origin of your disease. Proper diagnosis and therapy are essential to minimize irreversible nerve damage and enhance the possibility of a complete recovery. Not everyone needs surgery, and most people recover well from conservative care.
Post-surgical rehabilitation:
Physical therapy is essential for restoring full function and avoiding the creation of scar tissue after surgery to decompress the radial nerve. Typically, the rehabilitation program entails:
- Pain management: Post-surgical pain and inflammation can be controlled with the use of modalities and manual therapy.
- Restoring range of motion: Mild workouts help to prevent stiffness by progressively increasing the wrist and elbow’s range of motion.
- Activities for strengthening: As pain decreases, some activities help the hand and forearm muscles become more stable and strong, which supports optimal function. To help stretch and release the tight muscle and tissue surrounding the radial nerve, you can also perform a variety of exercises. These include:
- Wrist Extension Stretch: Raise your afflicted arm straight in front of you, palm upward, fingers pointing skyward. Pull back on your fingers with your other hand until your forearm stretches.
- Wrist Flexion Stretch: Extend the afflicted arm straight in front of you, palm down, fingers pointing downward. Pull back on the back of your palm with your other hand until your forearm stretches.
- Wrist supination: With your forearm and hand facing up, place your afflicted arm by your side at a 90-degree angle. With the other hand resting on your wrist, turn your forearm inward towards your body without causing any movement in the other limbs.
- Radial nerve glides: Standing upright, lowering your shoulders a little, and rotating your arms into your body are the steps for radial nerve glides. Tilt your head in the other direction, flex your wrist to one side, and raise your arm to waist level. Hold the pose for three to five seconds when you start to feel the stretch.
- Scar tissue management: By reducing the production of new scar tissue and enhancing tissue gliding, techniques like massage and scar mobilization can assist stop further compression.
- Functional retraining: Your therapist can help you restore your skill, coordination, and confidence in using your affected arm and hand by guiding you through exercises and tasks that mimic daily tasks.
Advantages of radial tunnel syndrome physical therapy:
- Enhances range of motion and flexibility while reducing pain and inflammation
- Boosts stability and strength
- Improves the glide of nerves
- Expedites healing and resumption of regular activities
- Aids in avoiding more issues
It’s crucial to remember that:
- A comprehensive evaluation will be performed by a physical therapist to determine your unique condition, restrictions, and objectives.
- After that, they will create a customized treatment plan based on your requirements and development.
- For best outcomes, the physical therapy program must be followed consistently.
- You can greatly increase your chances of recovering from radial tunnel syndrome and regaining full function in your arm and hand by speaking with a qualified physical therapist.
Prevention for the Radial Tunnel Syndrome
The following advice can be used to prevent radial tunnel syndrome:
- Steer clear of repetitive motions: Take regular breaks to stretch and rest your arms if your work or hobbies need you to make repetitive motions with your wrists and forearms.
- Keep proper posture: When seated at a desk, ensure sure your wrists are straight and your elbows are bent 90 degrees.
- Use safe lifting techniques: Don’t use your back when lifting large objects; instead, use your legs and core muscles.
- Develop stronger forearms: Consistently engaging in forearm strengthening activities can aid in providing support to the radial nerve’s surrounding muscles and tissues.
- Wear the appropriate braces or splints: Your doctor may advise wearing a brace or splint to help keep your wrist in a neutral posture if you are at risk of developing radial tunnel syndrome.
See a physician as soon as possible if you feel any pain, weakness, or numbness in your wrist or hand to receive a diagnosis and treatment plan.
Depending on the source and extent of the injury, there are wide variations in the long-term prognosis for radial nerve injuries. A full recovery is usually achievable. Most radial nerve injuries will heal with the initial therapy in around 12 weeks.
See your doctor about managing your symptoms if your nerve damage is caused by an underlying medical disease, such as diabetes or alcoholism. The fastest people to heal are those who are younger at the time of the injury and those who have had previous nerve damage traumas. A full recovery can take anywhere from six to eight months if surgery is required.
FAQs
What signs and symptoms are present in radial tunnel syndrome?
We should take into account that radial tunnel syndrome can manifest as elbow and forearm aches. The dorsal forearm and lateral elbow pain, which can also spread to the wrist and dorsum of fingers, are the diagnosis. The condition is more prevalent in women between the ages of thirty and fifty.
What signs and symptoms indicate a pinched radial nerve?
Pain, numbness, and/or paresthesia are possible signs of radial nerve damage, particularly in the thumb, middle finger, index finger, back of the hand, and/or arm.
How is radial tunnel syndrome treated?
Initially, nonoperative treatment for radial tunnel syndrome involves activity moderation, anti-inflammatory medication, and removable splints. Avoiding activities that require a continuous elbow extension with wrist flexion and forearm pronation is one way to modify one’s activity.
How much time does a radial tunnel last?
Stopping or significantly reducing the activity that is causing your symptoms is the best course of action for treating this disease. Try to rest your arm if you can, and stay away from any painful motions. For most people, symptoms can be successfully relieved in three to six weeks with rest and medication.
How is radial tunnel syndrome managed at home?
putting on an elbow brace. avoiding activities that exacerbate the pain and resting the hand and arm. using over-the-counter (OTC) pain relievers, such ibuprofen.
What kind of radial nerve exercise is the best?
Flex your wrist with the palm facing up and internally rotate your arm (thumb towards your body). Turn your head slightly away from the side you are extending. As you continue to tilt your head and flex your wrist, raise your arm away from your body. Hold each gliding position for three to five seconds.
References
- Shamrock, A. G., & Das, J. M. (2023, August 14). Radial Tunnel Syndrome. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK555937/#:~:text=Radial%20tunnel%20syndrome%20refers%20to,release%20reserved%20for%20recalcitrant%20cases.
- Professional, C. C. M. (n.d.-b). Radial Tunnel Syndrome. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/15658-radial-tunnel-syndrome
- Radial Tunnel Syndrome. (n.d.). Physiopedia. https://www.physio-pedia.com/Radial_Tunnel_Syndrome
- Woon, C., MD. (n.d.). Radial tunnel Syndrome – hand – orthobullets. https://www.orthobullets.com/hand/6024/radial-tunnel-syndrome
- Radial Tunnel Syndrome: What is it? Symptoms, causes, diagnosis, and treatment. (n.d.). https://www.assh.org/handcare/condition/radial-tunnel-syndrome
- Srakocic, S. (2021, March 24). Radial tunnel syndrome: What is it, and how is it treated? Healthline. https://www.healthline.com/health/radial-tunnel-syndrome



2 Comments