Maitland Mobilization Technique
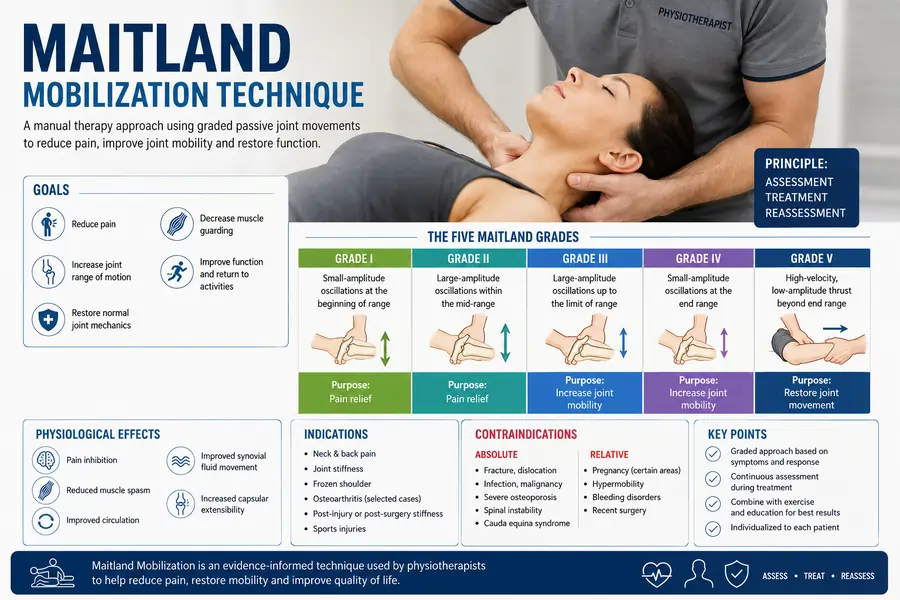
Maitland Mobilization Technique is a widely used manual therapy approach developed by Australian physiotherapist Geoffrey Maitland. It involves gentle, graded passive joint movements to reduce pain, improve joint mobility, and restore normal function.
The method is a safe and efficient treatment for a variety of musculoskeletal problems since it is based on a thorough patient assessment and uses several mobilization grades that are customized to the individual’s symptoms and condition.
What is Manual Therapy?
In general, manual therapy can be characterised as a hands-on approach with a therapeutic aim or as the use of hands in a healing and restorative manner.
Manual therapy techniques are used in many different fields to treat and manage disease and dysfunction, either as a stand-alone treatment or in combination with other therapies. Physical therapists are sometimes regarded as manual therapy specialists; manual therapy is also used in treatment by osteopaths, chiropractors, and nurses. Understanding the physiological, neurological, and psychophysiological mechanisms is essential to using manual therapy therapeutically competently and safely. Manual therapy operates through a variety of distinct methods.
From the standpoint of physical therapy, manual therapy is a crucial and often used therapeutic approach for the treatment of tissue, joint, and movement dysfunction.
Mobilisations from the Maitland school of thinking are undoubtedly the most popular, straightforward type of manual therapy utilised by physical therapists. There are various mainstream methods of manual therapy.
Maitland Concept
The Maitland Concept of Manual Physical Therapy, as it came to be known, places a strong emphasis on a particular way of thinking, ongoing evaluation and assessment, and the art of manipulative physical therapy—knowing when, how, and which techniques to use—as well as a complete dedication to the patient.
The Maitland idea may be applied to either the spinal joints or the peripheral joints; both require technical explanation and have different technical terminology and effects, but the basic theoretical approach is the same for both.
The idea bears the name of its creator, Geoffrey Maitland, who, together with a number of his associates, was regarded as a pioneer of musculoskeletal physical therapy.
Key Terms
Joint play movements, also known as accessory movements, are joint motions that an individual is unable to perform. These motions, which go hand in hand with a joint’s physiological movements, include roll, spin, and slide. To evaluate range and symptom response in the open pack position of a joint, the accessory motions are passively observed. Applying the Maitland approach therapeutically requires an understanding of accessory motions and their dysfunction.is essential to apply the Maitland concept clinically
Physiological movement is defined as any movement that an individual may actively do and assess for quality and symptom response.
Injuring Movement: During the clinical assessment, moving the joint in a certain way might cause the pain or symptoms to come on.
Overpressure: Every joint has a passive range of motion that is greater than its active range. The end of a typical passive movement is stretched to reach this range. There is almost always some discomfort in this region, and the subjective evaluation should determine whether there is a dislocation or subluxation.
Initial Assessment
A logically supported and derived hypothesis regarding the nature of the causes of the movement problem or discomfort may be formed using the Maitland concept, which is an excellent tool for making a first examination. You should study the part on Initial evaluation in Maitland’s book, Peripheral Manipulation, and think about incorporating mobilisations into your evaluation procedure.
A thorough and efficient evaluation is essential to each patient’s participation, just like in any treatment choice. By checking for warning signs, including malignancy, a recent fracture, an open wound or current bleeding, infectious arthritis, joint fusion, and more, the Subjective Assessment is required to determine whether mobilisations are appropriate for this patient or contraindicated.
One area where the adaptability of mobilisations is seen is the Objective Assessment. In addition to being a therapeutic approach, the therapist can evaluate a patient’s joints and tissues by examining their extensibility, pain reproduction, bony blockages, or abnormal end feels.
Principles of Techniques
Decisions Which Need to be Made:
- The direction– The physical therapist must use clinical reasoning to determine the mobilization’s direction and make sure it fits the diagnosis. Not every path will work for every disorder.
- The desired effects: What is the therapist hoping to achieve with mobilisation? Reduce discomfort or stiffness?
- The patient’s and the therapist’s starting position– to ensure a pleasant and successful course of therapy. To achieve a localised impact, it is also necessary to consider how the therapist’s hands will apply force.
- The Method of Application –
- The position
- range, amplitude, and rhythm
- duration of the technique.
- The Expected Response –
- Should the patient be pain-free
- have an increased range
- have reduced soreness.
How Might the Technique be Progressed?
Duration, frequency, or rhythm:
How to Choose the Direction?
Appropriate mobilisations, it is important to get the type of glide, the direction, and speed correct.
Different Types of Mobilisation: How Many Glides?
Each joint has a different movement are in a different direction from other joints, and therefore, care needs to be taken when choosing which direction to manipulate. Although it is not part of the concept used by Maitland, this is where the Concave Convex Rule could be used, but for now, consider it as the number of possible glides a clinician may use:
- A-P (Anteroposterior)
- P-A (Posteroanterior)
- Longitudinal Caudad
- Longitudinal Cephalad
- Joint Distraction
- Medial Glide
- Lateral Glide
Due to anatomical position and other physical limitations, not all peripheral or spinal joints can be subjected to all of the types of glide. Here are examples of mobilisations of joints of the body:
- Elbow Mobilizations
- Wrist/Hand Mobilizations
- Hip Mobilizations
- Knee Mobilizations
- Ankle and Foot Mobilisations
- Spinal_Manipulation
- Shoulder Mobilizations and Manipulation
- Cervicothoracic Manipulation
Concave Convex Rule: Up, down, Left or Right?
Choosing the direction of the mobilisation is to ensure you are having the desired clinical outcome. In summary:
There are two important things to remember
When a convex surface (i.e., head of the humerus) moves on a stable concave surface (i.e., Glenoid Fossa), the sliding of the convex articulating surface occurs in the opposite direction to the movement of the bony lever (i.e., the Humerus).
The opposite can be said, for example
When a concave surface (i.e., tibia, talocrural joint) is moving on a stable convex surface (i.e., talus), sliding occurs in the same direction as the bony lever.
Examples:
To improve shoulder flexion, perform an A-P mobilisation due to the way the convex humerus articulates with the concave glenoid fossa.
An easier way to visualise this is to try to show this rule with your hands.
How to Choose the Grade: How Far into the Range and Quickly or Slowly?
- Grade I – small amplitude movement at the beginning of the available range of movement
- Grade II – large amplitude movement within the available ROM (range of movement)
- Grade III – high amplitude movement that progresses to muscular spasm or stiffness
- Grade IV – small amplitude movement stretching into stiffness or muscle spasm
- Grade V – 5th grade is possible, but further training will be required to perform safely.
The grading scale has been separated due to its clinical indications:
Lower grades (I + II) are used to reduce pain and irritability (use VAS + SIN scores).
Higher grades (III + IV) are used to stretch the joint capsule and passive tissues that support and stabilise the joint, thereby increasing the range of movement.
The number of mobilizations should be thought of as an oscillation in a rhythmical way:
2Hz – 120 movements per minute
For 30 seconds – 1 minute
Therapeutic Effect
How and Why Does This Work, Mechanisms of Action?
Several complex systems interact to produce the pain-relieving effects of mobilisations; subsequently, there is not a single theory of its mechanism.
Pain Gate Theory
Thinking of pain theory in this way is very simplified and may not be suitable in some contexts, when discussing pain with patients, this description can be very useful.
An explanation of the sensory nerves is necessary to comprehend the PGT. At its simplest explanation.
There are 3 types of fibers:
- a-Beta fibres – Large diameter and myelinated – touch and pressure – Fast (50m/s)
- a-Delta fibres – Small diameter and myelinated – temperature and pain (well localised, sharp/prickly) – Medium (15m/s)
- C fibres – Small diameter and unmyelinated – pain (dull, poorly localised, persistent) – Slow (1m/s)
- The size of the fibres is an important consideration, as the bigger a nerve is, the quicker the conduction.
This means that, additionally, conduction speed is also increased by the presence of a myelin sheath; subsequently, large myelinated nerves are very efficient at conduction. A-Beta fibres are the quickest of the 3 types, followed by A-Delta fibres and finally C fibres
The interaction of these nerves is important, but it does not tell the whole story. It’s crucial to remember that just a portion of these neurons function as pain receptors. a-Delta fibers have a unique function in the sensory system and are frequently linked to the transmission of rapid, sharp pain sensations. These nerves all form synapses with projection cells, which then proceed to the brain via the spinothalamic tract.
Within the spinal cord, inhibitory interneurons act as gatekeepers. The inhibitory interneurons block the gate when there is no feeling from the nerves, since no crucial information needs to go to the brain. The gate is open, and pain is perceived when the smaller fibers are activated because the inhibitory interneurons do not respond. The gate is closed when the bigger a-Beta fibers are activated because they reach the inhibitory interneurons more quickly and prevent the interneuron from functioning. This explains why touching the region after banging your head or stubbing your toe helps because it activates the a-Beta fibers, which then block the experience of pain.
Descending Inhibition
Pain is dependent upon segmental modulation and descending regulation from higher centers in addition to modification during its ascending transmission from the periphery to the brain.
It must be viewed as a complex interplay of several distinct biological and physical elements that are required to be fully understood in order to properly understand the process, rather than only a linear one.
Should Manual Therapists Take Blood Pressure?
The effect manual therapy has on blood pressure is a contentious and sometimes overlooked factor while practicing manual treatment, especially on the neck. A 2012 publication by Taylor and Kerry emphasized this as a professional issue that should be a major concern for physiotherapists worldwide. Manual treatment may have a central effect on the central nervous system (CNS) or a local effect due to the cervical arteries’ proximity. Patients may be seriously at risk from this, as explained here.
When manipulating the cervical spine, care must be used due to the proximity of the vertebral artery to the lateral cervical articulations (MCS).
Due to poor food, high levels of stress, and sedentary lifestyles, hypertension—also known as “the silent killer”—is prevalent in the industrialized world. Surprisingly, 30% of individuals may not be aware of its grave implications. One of the leading causes of stroke is hypertension, which can also serve as a warning indicator for a patient’s stroke risk. Cervical manual treatment should thus be utilized to make sure there is no harm to the patient.
In a concerning study of 597 physical therapists, Frese et al. (2002) discovered that 47% of participants.
It’s never measured BP, and 4.4% said they regularly checked. The most frequent justification for choosing not to monitor blood pressure was that my patient population does not need it. Given the high rate of obesity, hypertension, and other recognized risk factors for stroke and hypertension, this is a worry and should be crucial for all patient populations.
Who benefits from the Maitland concept?
Your physical therapist will assess your back pain and decide which type of treatment is appropriate. Treatment according to the Maitland principle is often beneficial for those with mechanical back pain, such as joint discomfort and stiffness.
Use of joint mobilization: indications and limitations
- pain, muscle guarding, and spasm
- Reversible joint hypomobility
- positional faults/ subluxation
- progressive limitation
- functional immobility
Contraindication and precaution
- hypermobility
- joint effusion
- inflammation
Condition requiring special precautions for stretching:
Mobilization may be used with extreme care in the following conditions if the signs and the patient’s response are favorable:
- Malingnancy
- Bone disease
- Unhealed fracture
- Excessive pain
- Total joint replacements
Conclusion
One of the most popular manual treatment techniques in physical therapy is the Maitland Mobilization Technique. It aims to reduce pain, restore joint mobility, and enhance functional movement by using graded passive oscillatory motions that are customized to the patient’s symptoms and physical findings. When mobilization is paired with focused stretching, strengthening, and patient education, the highest results are often obtained.
FAQs
What is the Maitland protocol?
Using different mobilizations of the spine, peripheral joints, and other areas of the body to provide greater freedom of movement, the Maitland technique is a manual therapy diagnostic tool. This method helps you understand your limitations and gradually overcome them by using passive and accessory movements in a controlled setting. Using different mobilizations of the spine, peripheral joints, and other body regions to provide greater freedom of movement, the Maitland technique is a manual therapy diagnostic tool. This method helps you understand your limitations and gradually overcome them by using passive and accessory movements in a controlled setting.
Can Maitland help with stiffness?
For those with neck or back discomfort, joint stiffness, restricted range of motion, post-surgical limitations, or pain that varies with different postures or motions, the Maitland Method is particularly beneficial.
What should I expect during Maitland?
Your physical therapist will use their hands to move, manipulate, and apply pressure to the affected region or areas as part of the Maitland technique, which involves manual treatment and mobilization.
Is Maitland mobilization safe?
Motivation for research. Maitland mobilization was suggested in these investigations, and some evaluations have shown that manual therapy may be safe and beneficial in reducing the symptoms of osteoarthritis.
What is Grade 3 Maitland mobilization?
Grade III: This grade is characterized by gradual oscillations and large amplitude mobilizations that occur primarily in the middle to end of the range of motion. Grade IV: At the end of the range of motion, mobilizations in this grade have slow oscillations and a small amplitude. Movements that come into opposition are referred to as grades III and IV.
References:
- Kisner, C., & Colby, L. A. (1996a). Therapeutic Exercise: Foundations and Techniques. F. A. Davis Company.
- Maitland Technique, Physiopedia, https://www.physio-pedia.com/Maitland%27s_Mobilisations