Manual Techniques for the Cervicothoracic Spine
Introduction
Manual Techniques for the Cervicothoracic Spine are specialized hands-on treatment methods used by physiotherapists to improve mobility, reduce pain, and restore normal function in the neck and upper back region.
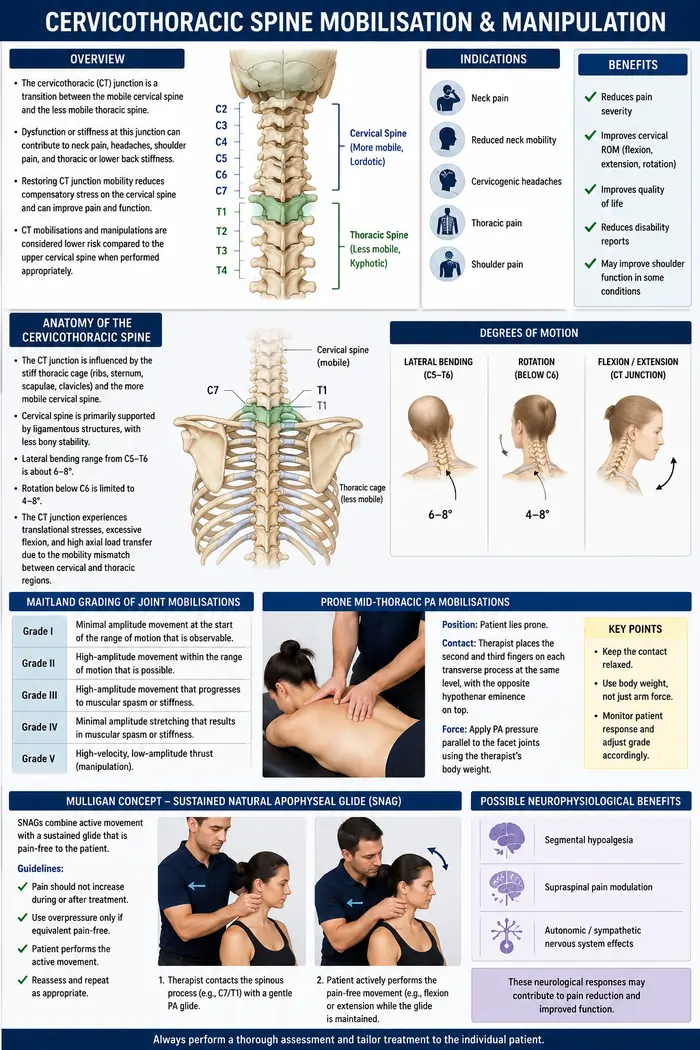
A possible site of stiffness is the cervicothoracic (CT) junction, which serves as a transition between the less mobile, kyphotic thoracic spine and the more mobile, lordotic cervical spine. Headaches, shoulder discomfort, neck pain, and general lower back stiffness can result from a reduction in cervicothoracic joint motion.
Although the evidence for this relationship mostly comes from older cross-sectional studies in occupational populations, a modified mobility pattern known as the “Inverse C7-T1 relationship” has been connected to neck pain, highlighting the significance of restoring proper CT junction mobility in people experiencing neck discomfort.
Enhancing CT junction mobility lessens the mid and lower cervical segments’ need for movement, which lessens the load on the cervical spine. Although careful assessment is still necessary, the cervicothoracic section is usually thought to represent a lower risk profile for modification than the upper cervical spine.
Therefore, cervicothoracic mobilization and manipulation are used as therapies for shoulder, neck, and thoracic discomfort and dysfunction. Because of the neurophysiological advantages of manual treatments and the concepts of regional interdependence, neck discomfort is often treated with manual therapy for the thoracic spine.
To reduce discomfort and improve range of motion, cervicothoracic mobilization and manipulation include a variety of skilled passive motions used at different speeds and amplitudes, from small-amplitude, high-velocity thrust methods to gentle oscillations.
Anatomy of the Cervicothoracic Spine
The safe implementation of manual treatment methods in the cervicothoracic area requires a grasp of its anatomy. When treating disease at this junction, it is important to take into account the markedly different degrees of mobility between the cervical and thoracic spines, which are separated by the cervicothoracic spine.
Because of its attachment to the chest, which includes the scapulae, clavicles, ribs, and sternum, the thoracic spine adds stiffness and reduced movement to this area. On the other hand, the cervical spine’s ligament-like components provide the majority of its structural support, with very little bone stability throughout.
Lateral bending shows a range of 6–8° between C5 and T6, but spinal rotation below C6 is restricted to a range of 4–8°. The cervicothoracic junction experiences translational stresses, excessive flexion, and a large transfer of axial load because of the great disparity in mobility between these adjacent areas.
Indications
Multiple research studies have been conducted, such as the Clinical Practice Guideline, which lists numerous indications for the use of cervicothoracic mobilizations and manipulations to reduce pain.
The following diagnoses indicate that adding this therapy to pain management may be beneficial.
- Pain in the neck
- Reduced neck mobility
- Cervicogenic headaches
- Pain in the thoracic region
- Pain in the shoulders
Benefits of Cervicothoracic Manual Therapy
Mid-thoracic manipulation improved the following in some examinations, including the meta-analysis on the impact of thoracic manipulation for neck pain:
- Pain severity
- Cervical flexion, extension, and rotation range of motion (ROM)
- Life Quality
- Reduced disability reports
It should be mentioned that further high-quality research is required because the overall trust in the data supporting these advantages is now assessed as low to extremely poor. According to some research, individuals with subacromial pain syndrome may benefit from cervical and thoracic joint mobilizations in terms of pain, disability, range of motion, and patient satisfaction. For further information, see CPR for Shoulder Pain and Cervicothoracic Manipulation.
Patients with forward head posture may benefit from grade IV cervical spine mobilizations (unilateral and central PA), according to some research.
It has also been demonstrated that thoracic mobilizations combined with deep flexor strengthening exercises might lessen chronic neck discomfort.
Neurological advantages of thoracic manual treatment have also been demonstrated. Positive clinical results are caused by a series of neurological reactions from the peripheral and central nervous systems that are triggered by the mechanical force generated by manual treatment. Segmental hypoalgesia, supraspinal pain modulation, and sympathetic nervous system effects are a few of them.
Cervicothoracic Spine Mobilisation
The Maitland Concept technique follows the grading of the joint mobilisations as follows:
- Grade I -A minimal amplitude movement at the start of the range of motion that is observable.
- Grade II-A high-amplitude movement within the range of motion that is possible.
- Grade III –A high-amplitude movement that progresses to muscular spasm or stiffness.
- Grade IV –A minimal amplitude stretching that results in muscular spasms or stiffness.
- Grade V –A manipulation of high-velocity, low-amplitude thrust (HVLAT).
Prone Mid-Thoracic PA Mobilisations
Technique:
Position: On a treatment table, the patient rests prone.
Contact: To perform the PA mobilisation, the therapist inserts the second and third fingers into each transverse process of the same level while resting the opposing hypothenar eminence on top.
Force: Apply pressure in a PA motion parallel to the facet joints using the therapist’s weight over the
Mulligan concept:
Sustained Natural Apophyseal Glide (SNAG)
Patients with neck discomfort have shown relief when using the Mulligan Concept approach for a Sustained Natural Apophyseal Glide (SNAG) applied to the cervicothoracic spine. SNAGs are painless spinal manual therapy methods that use active movement and sustained force application.
As with allMulligan approaches, overpressure should be used if the equivalent indication is painless. To guarantee that the therapies are suitable, these methods adhere to certain guidelines. Among the guidelines is the therapist’s search for the PILL response: P stands for painless, I for instantaneous, and LL for long-lasting.
- The approach shouldn’t be used if it doesn’t show the PILL response. CROCKS is the second principle:
- C-Contraindications
- (The absence of a PILL response is a contraindication in and of itself.)
- R-Repeated steps (day one consisted of just three repeats).
- O-Excessive pressure.
- C-Communication (between the patient and the doctor at all times).
- K-Understanding (of diseases and treatment plans).
- S-Maintain the mobilization throughout the whole movement.
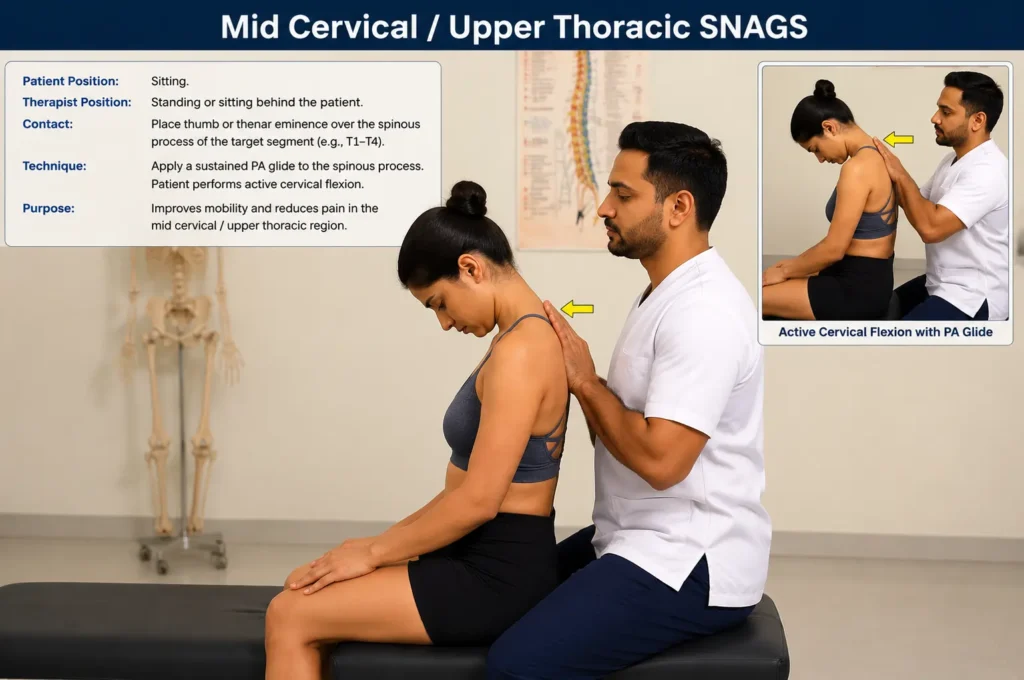
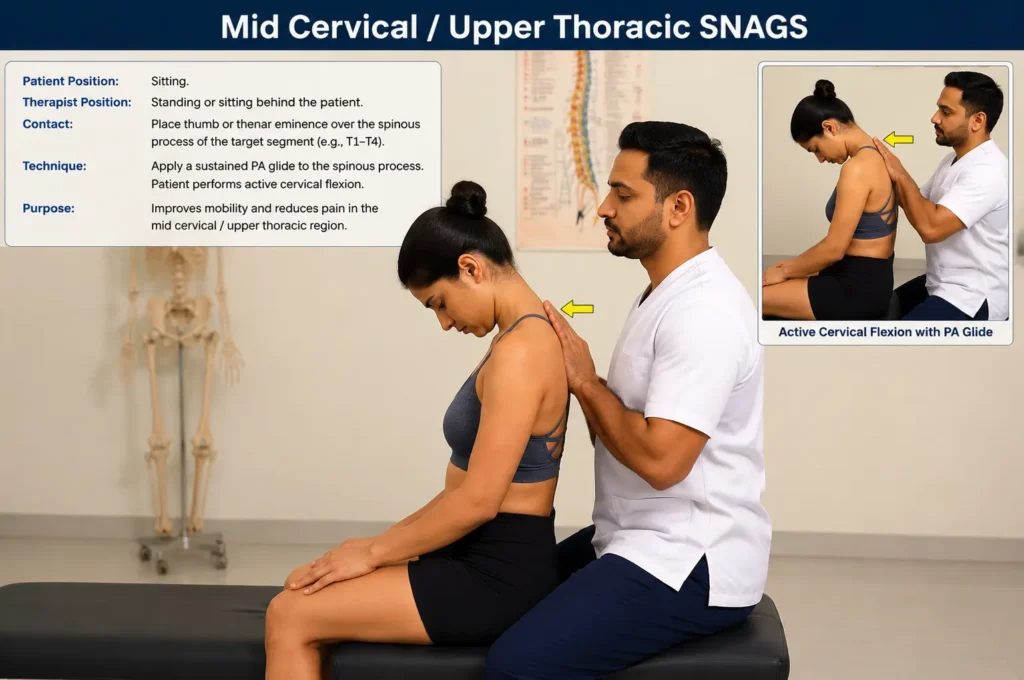
Mid Cervical/Upper Thoracic SNAGS Technique:
Mid-CervicalUpper-Thoracic-SNAGS-Technique
Position: The patient is sitting up straight.
Contact: The opposing thumb makes contact with the other side of the first thumb to supply the mobilization force, while the medial border of the distal phalanx of one thumb is on the articular pillar. When doing mid-cervical/upper thoracic SNAG, the therapist may make contact either ipsilaterally over the articular pillar (for an ipsilateral SNAG) or centrally over the spinous process. Regardless of the issue’s direction, it is advisable to begin by applying pressure to the painful area.
Force: Applied to the patient’s eye on the opposite side, anteriorly and superiorly along the facet’s plane.
Motion: While the clinician maintains a smooth gait during the whole movement, the patient actively flexes, extends, rotates, or side-bends while applying overpressure with their palm on their cheek.
Cervicothoracic Reverse SNAG Technique:
Position: The patient is sitting up straight.
Contact: Using a broad-based key grip with the spinous process between the thumb and index finger while standing to the patient’s side, the contact sites are at the transverse processes of the vertebra. In addition to providing control and a counterforce for the mobilization, the other arm will hold the patient’s head to regulate flexion or extension.
Force: Along the facet’s plane, directed superiorly and anteriorly.
Motion: While the therapist conducts an oscillatory mobilization in the anterosuperior motion for two to five oscillations per second while maintaining the glide, the patient remains passive.
Cervicothoracic Spine Manipulation
The functional and segmental limitations on range of motion are addressed by the HVLAT of the spine. To ensure that the therapy is suitable and to lower the chance of an adverse occurrence, a comprehensive investigation must be carried out utilizing [Reasoning|clinical reasoning]. When deciding whether to utilize an HVLAT, doctors must employ extra methods (such as red flags) due to unknowns surrounding screening tools.
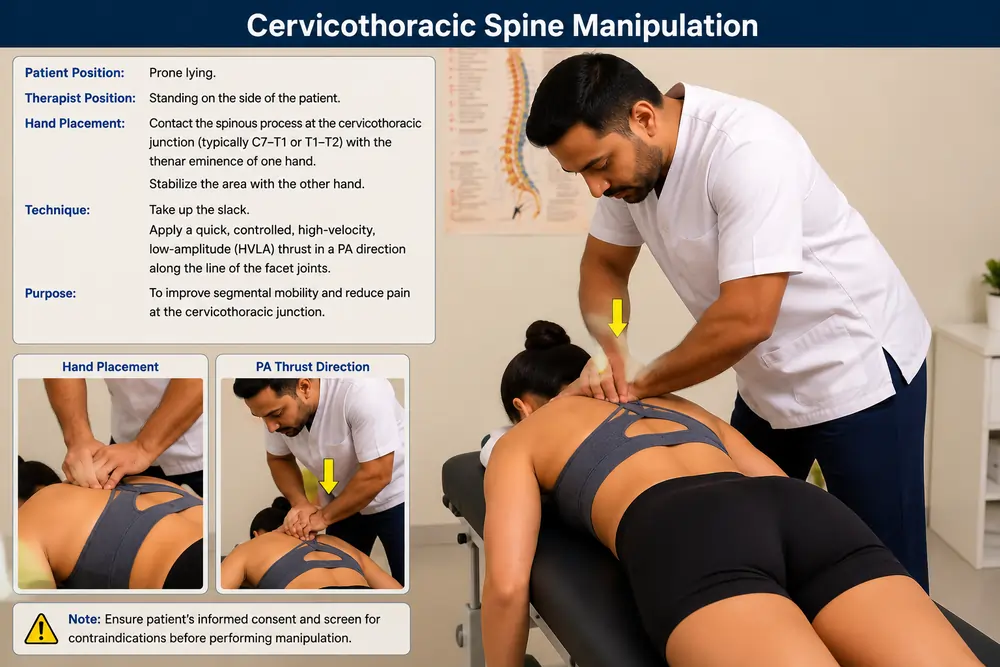
Cervicothoracic Junction Manipulation in Prone Technique:

- Contact: The therapist aligns the elbow at a 90-degree angle in the thrust direction and inserts the radial border of the proximal phalanx on the C7–T1 arch. The posterior/lateral temporal bone is where the cradle hand is located.
- The barrier is created at the C7–T1 articular pillar by the short-leveraged hand. To engage the segment, the long leverage hand then performs contralateral rotation, ipsilateral side bending, and PA extension.
- Thrust: The opposing forearm quickly adds rotation and side-bending to finish the impulse, while the short-leveraged hand delivers a lateral break toward the opposing axilla.
Precautions and Contraindications
Before administering mobilizations, particularly manipulation methods, a comprehensive history and clinical assessment are necessary. Informed permission, which includes a description of the method, its intended advantages, and any potential hazards, must be acquired before using any mobilization or manipulation techniques.
Contraindications for thoracic joint manipulation include:
Structural compromise and bony pathologies
- Tumor (such as metastatic illness)
- Infection (such as osteomyelitis or TB)
- Metabolic conditions (such as osteoporosis and osteomalacia)
- Congenital disorders (such as congenital fusions and dysplasias)
- Iatrogenic factors, including recent surgery, surgical fusion, and long-term corticosteroid usage
- Ankylosing spondylitis, rheumatoid arthritis, connective tissue disease, and synovial cysts are examples of inflammatory conditions.
- Traumatic injury (such as instability, ligamentous rupture, dislocation, or fracture
Neurological Disorders
- Acute myelopathy of the cervical, thoracic, or lumbar regions
- Compression of the spinal cord
- The Cauda Equina Syndrome
- Progressive compression of nerve roots accompanied by neurological impairments
- Sensory loss or bilateral hyperreflexia
Vascular Pathologies
- Cervical artery abnormalities or vertebrobasilar insufficiency
- Aortic aneurysm
- An anticoagulant medication or bleeding problems
- Pectoris angina
- Untreated dysrhythmias or cardiac insufficiency
- Acute stomach discomfort accompanied by guarding
Precautions
- Negative response to earlier manipulation
- Inflammatory joint processes
- Minor osteoporosis
- Disc herniation and disc protrusion
- Spondylolisthesis
- Hypermobility or ligamentous laxity
- Arterial calcification
- Arterial hypertension
- Serious degenerative joint diseases
- Growing children: open growth plates or growing ossification centers
- Serious kyphosis and scoliosis
- Herpes zoster on the thoracic spine
- Systemic infections
- Psychological dependency upon manipulation
- Pain with a psychological overlay
- Despite several modifications, the symptoms have not changed or gotten worse.
Conclusion
Neck discomfort, thoracic pain, and shoulder dysfunction can all be effectively treated by cervicothoracic mobilization and manipulation. To ensure that informed permission is gained and contraindications are ruled out before beginning treatment, clinicians should choose approaches based on comprehensive evaluation, clinical reasoning, and patient presentation.
Manual therapy should be incorporated into a more comprehensive rehabilitation program that includes exercise, even if existing data suggest short-term advantages in pain and range of motion. The overall confidence in the evidence base is still low to critically poor. To bolster the evidence for these methods, more rigorous research is required.
FAQs
What is the best position for cervical traction?
However, disc edema and/or neck discomfort with muscular or soft tissue causes are the most common conditions for which prolonged traction is employed. The patient may be sitting or in a supine position while cervical traction is given. Because it allows for more posterior pressure loading, the supine posture is recommended.
Who should avoid cervical traction?
Physicians should avoid using cervical traction in patients who have any of the following probable or relative contraindications: acute torticollis, aortic aneurysm, active peptic ulcer disease, discitis, osteomyelitis, osteoporosis, ligamentous instability, primary or metastatic.
What is the best cervical traction device for home use?
Your level of discomfort will determine which at-home neck traction device is ideal for you. Foam neck stretchers, such as RestCloud, provide rapid static relief for moderate stress and poor posture. Inflatable neck braces or over-door water bag systems (like Dynamic or Parsons) provide customizable stretching for focused decompression of pinched nerves.
What exercises should be avoided with cervical compression?
High-impact activities: Running, leaping, and contact sports are examples of high-impact activities that should be avoided since they can further damage the spine. Heavy lifting: Excessive lifting might worsen your symptoms and put a lot of strain on your spine.
References
1. Joshi S, Balthillaya G, Neelapala YVR. Immediate effects of cervicothoracic junction mobilization versus thoracic manipulation on the range of motion and pain in mechanical neck pain with cervicothoracic junction dysfunction: a pilot randomized controlled trial. Chiropr Man Therap.
2. Hutting N, Kerry R, Coppieters MW, Scholten-Peeters GGM. Considerations to improve the safety of cervical spine manual therapy.
3. https://www.physio-pedia.com/Manual_Techniques_for_the_Cervicothoracic_Spine