Elbow Joint Mobilization
Elbow Joint Mobilization is a physiotherapy technique used to improve elbow joint movement, reduce pain, and restore normal function. It involves gentle, controlled manual movements performed by a qualified physiotherapist to address joint stiffness caused by injury, arthritis, surgery, or prolonged immobilization.
Elbow joint mobilization can improve range of motion, improve flexibility, and facilitate a quicker return to daily activities and sports when paired with stretching and strengthening exercises.
Elbow Joint Complex
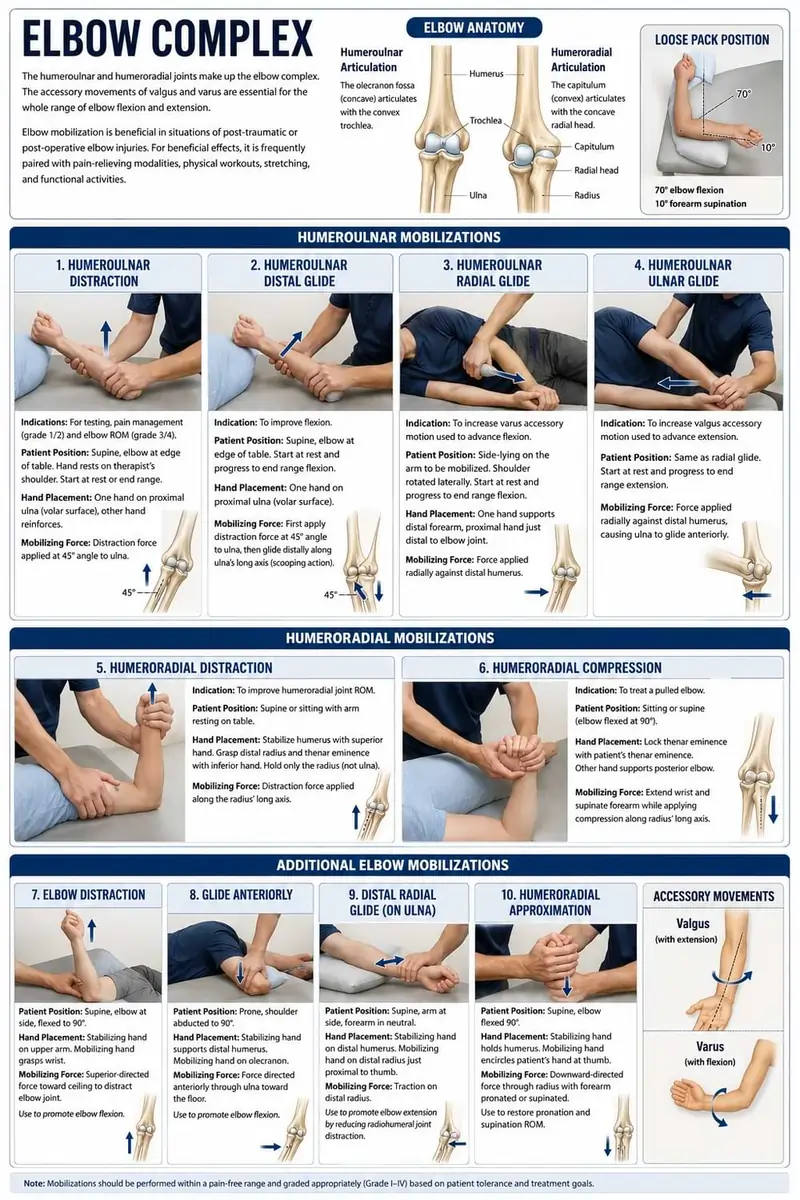
The humeroulnar and humeroradial joints make up the elbow complex. The accessory movements of valgus and varus are essential for the whole range of elbow flexion and extension. Each joint’s method is explained.
Elbow mobilization is beneficial in situations of post-traumatic or post-operative elbow injuries. For beneficial effects, it is frequently paired with pain-relieving modalities, physical workouts, stretching, and functional activities.
Humeroulnar Articulation
The olecranon fossa, which is concave, articulates with the convex trochlea.
Loose pack position
- 70 degrees of elbow flexion
- 10 degrees of forearm supination.
Humeroulnar Distraction and Progression
- Indications: For testing purposes, pain management (grade 1/2) and elbow range of motion (grade 3/4).
- Patient Position: Lying supine, place your elbow at the edge of the treatment table. The joint will be held in a resting position during the initial treatment, and the patient’s hand will rest on the therapist’s shoulder.
To stretch into flexion or extension, the therapist has to position the elbow at the limit of the possible range. - Hand Placement: The patient’s elbow is maintained either at rest or at the maximum range of flexion. The therapist covers the proximal portion of the ulna on the volar surface with one hand and uses the other to strengthen it.
- Mobilizing Force: At a 45-degree angle to the bone’s shaft, force is delivered at the proximal ulna.
Humeroulnar Distal Glide
- Indication: To improve flexion.
- Patient position: Lying supine with the elbow resting on the treatment table’s edge. At first, the elbow is at rest. The elbow is positioned at the end range of flexion to make progress. The therapist applies pressure with one hand to the proximal ulna over the volar area.
- Mobilizing Force: The therapist first applies the distraction force to the joint at a 45-degree angle to the ulna. Then, while keeping the distraction force in place, the force is applied distally along the ulna’s long axis. We refer to this as a scooping action.
Humeroulnar Radial Glide
- Indication: To increase the varus accessory motion, which occurs concurrently with elbow flexion and is therefore utilized to advance flexion.
- Patient Position: Rotate the shoulder laterally while sidelying on the arm that has to be mobilized. The table provides support for the humerus. Start at rest and work your way out to end-range elbow flexion.
- Hand Placement: The physical therapist supports the distal forearm with one hand while keeping the base of their proximal hand just distal to the elbow joint.
Humeroulnar Ulnar Glide
- Indication: To enhance the range of motion (ROM) of the elbow joint by increasing valgus, an accessory motion that is accompanied by elbow extension.
- Patient position: The wedge is retained beneath the proximal portion of the forearm for stability, much like in the radial glide. The elbow is maintained in the resting position throughout the first therapy sessions, then gradually extended to the end range.
- Mobilizing Force: The ulna glides anteriorly as a result of the force acting radially against the distal humerus.
Humeroradial Articulation
The capitulum is convex, and it articulates with the concave radial head.
- Resting Position: Forearm supination and elbow extension to the maximum extent possible.
- Treatment Plane: It has a concave radial head that is perpendicular to the radius’s long axis.
Humero-radial Distraction
- Indications: To improve the humeroradial joint’s range of motion.
- Patient Position: With the arm resting on the treatment table, one can lie supine or sit.
- Therapist Position and Hand Placement: The therapist is positioned between the client’s hip and upper extremity on the ulnar side of the forearm. Use your superior hand to stabilize the client’s humerus. Using your fingers, grasp the inferior distal radius and thenar eminence of your hand. Only the radius should be grasped or held, not the ulna.
- Hand placement: The therapist stabilizes the patient’s humerus on the medial side of their arm. The palmar surface of the lateral hand grips the radial head.
- Mobilizing force: The therapist’s palm moves the radial head in a volar or dorsal direction.
Humeroradial compression
- Indication: To treat a pulled elbow
- Position of the patient: Sitting or supine (elbow flexion at 90 degrees)
- Hand placement: The therapist’s right hand is used to approach the patient’s right hand, and vice versa. Another hand is used to support the posterior portion of the elbow. The client’s thenar eminence is locked with the therapist’s thenar eminence.
- Mobilizing force: The therapist extends the wrist and supinates the forearm while applying compression stress along the radius’s long axis.
Elbow Distraction
The patient is placed supine on a mat for this procedure, with their elbow at their side and bent to a 90-degree angle. The non-mobilizing hand stabilizes the upper arm. By grabbing the patient’s wrist and applying a superior-directed effort toward the ceiling, the mobilizing hand distracts the elbow joint and encourages the joint play required for elbow flexion.
As a mobilization to encourage elbow extension or an anterior capsular stretch, this method can also be used with the elbow further extended.
Glide Anteriorly
The operator uses the stabilizing hand to support the distal humerus while the patient is in a prone posture with the shoulder abducted to a 90-degree angle. The olecranon process is covered by the mobilizing hand.
The ulna is moved anteriorly during mobilization by applying a force straight through its line and toward the floor. This method is frequently applied to increase elbow flexion.
Distal Radial Glide (on Ulna bone)
The patient was in a supine posture with their forearm neutral and their arm at their side. One hand stabilizes the distal humerus. Just proximal to the thumb, the mobilizing hand is positioned along the distal radius.
The therapist tugs on the distal radius, causing mobilization. By diverting attention from the radiohumeral joint, this method is frequently utilized to encourage elbow extension.
Humeroradial Approximation
The therapist uses the stabilizing hand to hold the patient’s humerus as they lie supine on a mat with their elbow flexed perpendicular to the mat. The patient’s hand is encircled by the mobilizing hand at the thumb.
A downward-directed force that passes through the radius and is either pronated or supinated is the mobilization. Regaining pronation and supination range of motion can be accomplished using this approach.
FAQs
What is the mobilization of the elbow fracture?
Mobilisation comprises graded passive or active motions of the elbow joint with the purpose of avoiding joint stiffness, soft tissue contracture, and eventual restoration of normal mobility.
What are the different types of joint mobilization?
Physical therapists use expert, hands-on passive joint mobilizations to increase range of motion, reduce joint discomfort, and enhance flexibility. The three main categories of joint mobilizations are oscillatory, sustained, and manipulative
What are the three types of mobilization?
1. The mobility of oscillatory joints is gradual and mild. With greater mobility and less pressure, it exercises your joints passively.
2. Long, deep stretches are similar to sustained joint mobilization.
3. Joint manipulation requires greater power.
What are mobilization techniques?
Physical therapists employ joint mobilization, a hands-on manual treatment approach, to increase joint mobility, reduce discomfort, and restore normal movement.
What mobilization improves wrist extension?
Use a volar glide, which involves moving the carpal bones in the direction of your palm, to promote wrist extension. To lessen pinching and increase range of motion, this motion mimics natural joint mechanics.
References
- https://www.physio-pedia.com/Elbow_Mobilizations
- Carolyn Kisner. Therapeutic Exercise. Foundations and techniques. Sixth edition