Pseudobulbar Palsy
What is Pseudo-bulbar palsy?
A disease known as pseudo bulbar palsy is caused on by an upper motor lesion resulting from a bilateral disruption of the corticobulbar pathways. Dysarthria, dysphagia, facial and tongue paralysis, and emotional instability are signs of pseudobulbar palsy.
It manifests as the incapacity to regulate facial motions, such as speaking and eating, and is associated with a number of neurological conditions. Patients have trouble swallowing and chewing, develop stiffness in the tongue and bulbar region, faster reflexes, and slurred speech, which is frequently the disorder’s first symptom. Occasionally, they also have uncontrollable emotional outbursts.
The corticobulbar pathways, which are upper motor neuron routes that connect the brain stem’s cranial nerve nuclei to the cerebral cortex, are often damaged bilaterally in pseudo-bulbar palsy.
Signs and symptoms of the Pseudobulbar palsy
- Slow and indistinct speech
- Dysphagia is the inability to swallow.
- The tongue is small, rigid, and spastic.
- Brisk jaw jerk
- Speaking difficulties due to dysarthria
- The labile effect
- The gag reaction might be absent, increased, or delayed.
- Lesions on the limbs’ higher motor neurons may be discovered during the examination.
Causes of Pseudo-bulbar palsy
- Damage to motor fibers from the cerebral cortex to the lower brain stem results in pseudobulbar palsy. A number of neurological disorders, including bilateral corticobulbar lesions and demyelination, may cause the injury. Examples may of:
- Vascular causes include cerebral autosomal dominant arteriopathy with subcortical infarcts and bilateral hemisphere infarction. Percheron infarct and leukoencephalopathy syndrome.
- Supranuclear palsy that progresses
- Amyotrophic lateral sclerosis
- Parkinson’s disease, multiple system atrophy, and a variety of motor neuron disorders, particularly those involving demyelination
- Inflammatory diseases, including multiple sclerosis
- elevated brain stem tumors
- Osmotic demyelination syndrome is a metabolic cause.
- Behçet’s illness and its neurological component
- Brain Trauma
Rare causes of pseudobulbar palsy
- Pseudobulbar palsy: Common signs of central pontine myelinolysis.
- Rarely,a bilateral thalamic infarction of certain nuclei presents as pseudobulbar palsy.
- Acute or subacute neurological clinical signs and symptoms, persistent pseudobulbar palsy, and methotrexate-induced neurotoxicity are rare.
- Multifocal leukoencephalopathy that progresses: Pseudobulbar symptoms are rarely ever caused by it.
- Cerebral malaria: Demyelination may be the cause of pseudobulbar palsy in cases of cerebral malaria.
- Bacterial endocarditis: This condition can cause cerebral disturbances, such as pseudobulbar palsy.
- Examining the cerebrospinal fluid is necessary for syphilis.
- Large petroclival meningioma: It exhibits emotional instability and bulbar motor impairment, which are indicative of pseudobulbar palsy.
- It is rare to have neurocysticercosis.
- The significance of early detection of anti-thyroperoxidase antibodies in a patient with pseudobulbar palsy is highlighted by autoimmune encephalitis and Hashimoto encephalopathy.
Pathophysiology
Pseudobulbar palsy is thought to be caused by the disinhibition of the motor neurons that control laughing and tears. This suggests that there is a reciprocal connection between the brain stem and the cerebellum that modifies laughter and crying responses to make them suitable for the situation. Stimulation in the brain’s subthalamic nucleus may also cause pseudobulbar tears.
Prevalence of the Pseudo-bulbar palsy
The etiology of corticobulbar pathway injury determines the development of pseudobulbar palsy. Bulk rises, especially after age 50, according to the development of motor neuron illness, including pseudobulbar palsy. In every age group, the incidence is greater in men than in women.
One in five people who have an acute stroke and one in eight who have a chronic stroke are affected by pseudobulbar apathy.
How is pseudobulbar palsy diagnosed?
Pseudobulbar palsy is mostly diagnosed by medical professionals based on your symptoms. If the underlying reason is unknown, determining it is the main issue.
A healthcare professional will ask about when your symptoms started. Additionally, they will want to know about your medical history, including any strokes you may have had. They will do a neurological and physical examination.
Pseudobulbar palsy can be caused by a wide range of illnesses; therefore, your doctor may suggest a number of tests to rule out or confirm potential causes. These might consist of:
- blood testing.
- Cerebrospinal fluid (CSF) examination by spinal tap.
- Imaging studies, such as an MRI of the brain.
- Electroencephalogram, or EEG.
- Evoked potential tests
- Evaluations of speech and cognition.
Treatment of Pseudo-bulbar Palsy
Dysphagia ( difficulty in swallowing )
Effortful Swallow
- Collect the saliva in the middle of the tongue.
- Continue to squeeze your lips together.
- Swallow all over the salivary secretions at the same moment as you’re eating grapes/or a medication.
Dynamic Shaker
- Lie on your back supine reclining on a flat surface or treatment table. Avoid using a cushion or headrest and make sure the shoulders are pressed up against the surface.
- To regulate the shoulders on the level surface, raise up the chin as if you’re attempting to look at your feet.
- Return the head to the level surface.
- Repeat 30 times. Then relax for 2 minutes. As directed by a therapist, repeat more times.
Jaw Thrust
- Place your bottom teeth in front of your upper teeth by thrusting your lower jaw as far forward as you can.
- Hold the position of jaw thrust for the period of time recommended by the doctor or/and physical therapist.
- Repeat the jaw push additional times as advised by the doctor or physical therapist.
Masako Maneuver
- Rod your tongue out of your mouth.
- Bite down lightly on the tongue to hold it in place.
- Hold your tongue between your middle teeth while you swallow.
- Release your tongue. Then, repeat as often as a physician or therapist advises.
Mendelsohn Maneuver
- Press the index, middle, and ring finger of one hand, either right or left, on the neck to identify your apple—the little bump and/or just the skin on the front side of the neck behind the chin.
- Take a single swallow and observe how the apple rises and falls.
- Squeeze your throat muscles to hold the apple at its highest position as you swallow once again.
- Hold it for as long as the therapist suggests, or for as long as you can if you are still unable to do so.
Supraglottic Maneuver
- Arrange a bit of saliva in the mouth.
- Take an in-depth breath/inhalation and maintain that deep breath/inhalation.
- Hold your breath while you swallow.
- Cough as soon as you’ve swallowed.
- Once you have swallowed downward with saliva, you may sample the food or drink at the site of a therapist.
Hyoid Lift Maneuver
- Assemble objects like a drinking straw, bits of paper towel, and a cup. You should start with 3 to 5 sheets of paper and work up to 10 times as your strength develops.
- Put the straw in the mouth.
- Use the straw to absorb, then use the hammering suction to pick up a piece of paper.
- Maintain a strong enough suction to collect every single piece of paper that is larger than a cup.
- Let the paper drop into the cup after stopping the absorption.
- Repeat till all bits of paper fall down in the cup.
Straw drink: Place a straw in a cup with its flat end facing away from your upper teeth. Place the tongue tip on the adjusted place. Seal lips firmly. When the drinking process begins, you have to keep your teeth together. The objective is to suck up a ¼ cup of water in less than 30 seconds.
The balloon pops: Squeeze out the air with a quick blast of sound using a flat palm after filling your cheeks with air and tightly closing your lips.
Using the nose to blow up a balloon
Dysarthria
Oro motor exercises
Tips for Oral Motor Exercises
- Depending on the child’s particular needs, these oral motor activities might be selected. Each exercise may not work for all people. And, the oromotor exercises should be improved as needed to grade up or down and make them easier or harder dependent on the demand of the individual. The number of days or motor exercises that should be performed each week should be added.
- Whenever possible, integrate the function. Add interesting actual meals. When you can, use cups or utensils. included the concept of play to make the workouts enjoyable and inspiring.
- See a pediatric occupational therapist for advice.
- Raise their fingers and hands up to their lips and mouth.
- Use a mirror to play tongue. different oral motor instructions that may be used to target particular motor abilities involving the lips, jaw, cheeks, and tongue.
- Use your tongue and cheeks to play the game “hokey pokey.”
- Play messily with food.
- Encourage tolerance of a spoon or other eating utensils in different sections of the mouth.
- Keep your mouth open and shut.
- Make distinct side-to-side movements with your tongue.
- Plump your lips after pressing them together.
- evaluate various types of utensil textures, plastic, metal, plastic-coated, etc
- Brush the patient’s mouth and face while holding and playing with a toothbrush.
- Describe the mouth’s components and encourage mirror play.
- Add rhythmical, whole-body play with therapeutic balls, and uneven surfaces such as trampolines or crash pads to boost proprioceptive input. fantastic for strengthening and stabilizing the core, which is necessary for eating, cleaning teeth, etc.
- Examine mouth play with teething instruments and toys.
- Examine how teething toys and equipment are used in various positions, including as prone, supine, side-lying, etc.
- Use rhythmical music, inclusive of touching the cheeks or lips.
- Offer frozen fruit on a tongue depressor. Try making frozen fruit skewers with this recipe.
- Chew a straw.
- Pucker your lips in an assumed kiss.
- Use a party noise maker.
- Use a straw to pick up squares of paper and drop the paper into a basin.
- Prepare fish lips
- Try to use a stick with an attractive scent and push your lips together while you move your lips from side to side.
- Puff up your cheeks.
- Make your lips square.
- Buzz the sounds of the alphabet make from A-Z. Take note of your mouth’s movements. Alternatively, use the buzzing sounds of the letters to spell out your name or other things.
- Blow bubbles
- A cotton ball or tiny craft pom may be moved down a line by blowing through a straw.
- Suck the ice till it melts after freezing water on a stick.
- Try using sticks to create a Shirley Temple. Popsicles are a delicious way to practice your oral motor skills.
- Pour water into an ice cube tray. Add popsicle sticks to produce a cube pop. Lick and absorb until the ice melts.
- Scoop peanut butter onto a spoon. Use the tip of your tongue to lick the peanut butter off.
- Mark the tip of your nose with your tongue. As many times as you can, maintain the posture.
- touch your tongue to your chin.
- Hold the posture.
- In your right cheek, press your tongue. Press the tip of your tongue into your left cheek while holding it.
- Use your tongue to count your teeth. Touch individual teeth with the tip of your tongue.
- Chew some bubble gum.
- Deep breathing mouth exercises. Use these printable deep breathing cards.
Puffy cheek breathe
- Press your lips together, blow up your cheeks, take a big breath through your nose, hold it in, and then exhale through your nose.
- Repeat three to five times.
Submerged cheek breathe
- Inhale deeply through your nose while keeping your cheeks drawn in. Then, exhale through your nose after sucking your cheeks and pressing your lips together.
- Do this three to five times.
Pressed lip breathe
- Press the lips together in a straight line.
- Take prolonged breathing through the nose.
- Breathe out slowly through your nose.
- Repeat three to five times.
Reverse tongue breathe
- Pull your tongue back into the back of your mouth, open your mouth wide, take a big breath, hold it in for a few seconds, then release it while keeping your mouth open. Repeat 3 to 5 times.
Tongue touch breathe
- Put the tip of your tongue on the root of your mouth, inhale deeply through the side of your mouth, keep it there for a few seconds, then exhale through the side of your mouth 3 to five times.
Breath Control Exercises
- Breathe in gently for 3 seconds.
- Hold your breath for 3 seconds.
- Exhale the air slowly for 3 seconds.
- Continue breathing in this regulated way.
Hyperadduction Exercises
- Patients with hyperadduction of the articulatory folds can look like with incorrect articulation quality and too much loudness. Use simple phonation and gentle articulatory touches to treat.
- Practice speaking in a low voice.
Diaphragmatic Breathing
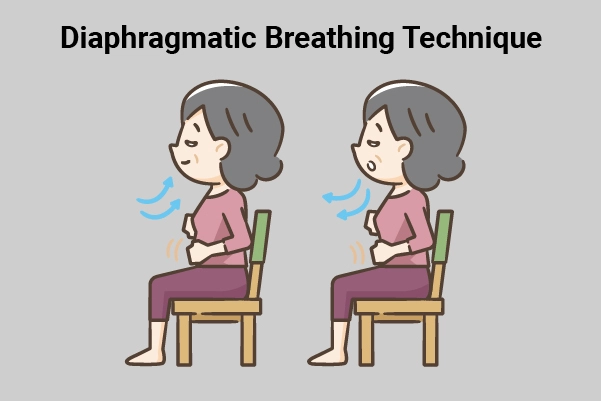
- Position: Put one hand on your stomach and the other on your chest.
- Feel your stomach elevate and go down with each individual breath. Continue for 1 minute.
- The stomach pulls in as you inhale. The hand on the chest should remain motionless and maintain its posture.
- Feel the muscles in your stomach tighten and draw in as you exhale. The hand on the chest should remain motionless and maintain its posture.
- Feel your tummy push out as you inhale. As you breathe out or exhale, say the following noises and words, staying mindful of the stomach softly drawing in.
- Use simple breathing noises like “sss” and “shh” to begin.
- Typically progress to vowel sounds like “ahh” and “ooh.”
- Work your way up to lengthier words, phrases, and sentences by starting with simple words like “hello” and your first name.
Pursed lip breathing
- Increases ventilation
- releases retained air in the lungs, keeps the airways open, and slows down the pace of breathing by continuously exhaling.
- restore breathing patterns by allowing fresh air to enter the lungs and removing old air.
- Relieves shortness of breath. Create general relaxation
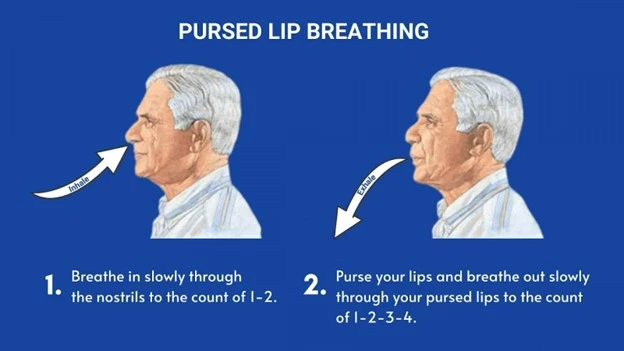
Pursed lip breathing technique
- Your shoulder and neck muscles should be relaxed.
- Inhale gently past the patient’s nose for 2 counts, keeping your mouth closed. Do not take a longer breath inhalation; a typical breath pattern will do. Inhaling could help you count to one or two.
- Pucker your lips as if you will use a whistle or carefully flicker the light of a candle.
- While counting to four, gently and softly release your breath through pursed lips. Breathing out may assist you to count to yourself for exhale, and count.
lateral costal expansion

- Lateral costal expansion. Often referred to as lateral basal expansion, it can be performed unilaterally or bilaterally while the patient is seated or in a comfortable hook-lying posture. Place your hands on the lateral side of the lower ribs to focus the patient’s attention on the area where movement is to occur.
- ask the patient to exhale and feel the motion of the rib cage downward and inward as the patient start exhales put rigid toward the ground pressure into the ribs with the palm of the patient’s hands just before to inspiration, administer a rapid downward and inward stretch to the chest region, this placement is rapidly stretch on the external intercostal muscle to encourage the promoted contraction external intercostal muscles turn the ribs outward and upward during inhalation
- As the patient inhales, instruct them to extend their lower ribs instead of your hands.
- Help the patient by compressing the rib cage in a downward and outward path. Once the patient is taught to perform maneuvers independently, the patient may cover their ribs with their hand or apply resistance with a belt. Apply mild but firm manual resistance to the lower rib part to accelerate sensory comprehension as the patient inhales in and the chest expands, and the ribs flare again as the patient exhales.
To improve chest mobility
To mobilize one side of the chest
- When seated, the patient moves away from the tight side to stretch the tight organization and expand the side of the chest during inhalation, then the patient presses the fisted palm into the lateral aspect of the chest as he/she bend toward their tight side and exhale.
- progression by requiring the patient to bend away from the tight side and raise the arm on the right side of the chest past the head.
- This will cause the tight tissue to stretch even more.
To mobilize the upper chest area and stretch the pectoral muscles
- Instruct the patient to pull both elbows together and bend forward during exhale while they remain seated in a chair with their hands clasped behind their head. During deep inhalation, have the patient horizontally abduct their arms, lengthening their pectorals.
To mobilize the upper chest and shoulders
- When the patient is seated in the chair, have him or her extend both arms 180 degrees past the head while flexing both shoulders and slightly abducting them during inhalation.
- When exhaling, the patient must lean forward at the hips and reach for the ground.
To increase exhalation during deep breathing
- The patient’s hips and knees are gently flexed while they breathe in a hook-lying position.
- Tell the patient to lift both legs to the chest once at a time to protect the lower back during exhalation.
- Knee to the chest moves the stomach contents superiorly into the diaphragm to help with expiration.
Facial muscle exercises
Brower raise
- Place your index and middle fingers in a closed, peaceful stance.
- Rest your fingertips beyond your eyebrows and slightly press the skin down.
- Lift your eyebrows up and down, while producing resistance with the weight of your fingernails.
- Repeat 10 times
- Complete 6 sets
Cheekbone lift
- Place your fingertips on each cheekbone.
- Lift the skin gently until it becomes tight.
- Open your lips to form an extended “O” arrangement; you should feel resistance in your cheek muscles.
- Hold for 5 seconds
- Complete 10-15 sets
The cheeks squeeze
- Extremely chubby cheeks and a justification for making a fish face repeatedly. Sign us up.
- Push your chin forward and tilt your head all the way back.
- Suck your cheeks in as much as possible.
- Hold for 5 seconds
- Complete 10-15 sets of repeats
Jaw flexion
- Turn your head so that you are facing the ceiling.
- Move your lower lip beyond your upper lip as far as you can; you should feel this in the jaw muscles. Shut your ears.
- Hold for ten seconds.
- Complete 10-15 sets of repeats
Puffer fish press
- Puffer fish press facial exercise will help to inhibit the very un-funny look of the laugh lines around your mouth. Here’s how:
- close down your mouth and inflate the cheeks
- passes the air from one cheek to the other side.
- Repeat for 30 seconds.
What are the complications of pseudobulbar palsy?
The following issues could happen from pseudobulbar palsy:
Aspiration pneumonia: When you have trouble controlling your lips and tongue, you may inhale food particles or liquids, which can result in aspiration pneumonia.
Malnutrition and dehydration: It can be very difficult to swallow meals and drinks if you have severe dysphagia. Dehydration and malnutrition may result from this. If your dysphagia is severe, you could require a feeding tube.
Mental health issues: Your life may be greatly impacted by pseudobulbar palsy. Additionally, some of its side effects, such as trouble speaking and excessive emotional outbursts, may make you avoid social situations. This may have an impact on your mental well-being and lead to anxiety and/or depression.
FAQs
What is the most prevalent cause of pseudobulbar palsy?
Traumatic brain injuries.
tumors .
Inflammation and infections that impact your brain.
Chronic (long-term) neurological problems.
Cerebrovascular diseases, include strokes and vascular abnormalities.
Is pseudobulbar palsy a stroke?
Pseudobulbar affect (PBA) is the result of damage to the brain regions that regulate emotions. Other names for this neurological illness include involuntary emotional expression disorder, emotional lability, and reflex weeping. PBA arises as a result of numerous neurological illnesses, such as: Stroke
What are the main symptoms of PBA?
Frequent, uncontrolled, and uncontrollable outbursts of crying or laughing that are exaggerated or unrelated to your emotional state are the main indicator of pseudobulbar affect (PBA). Tears frequently follow laughter. Between incidents, which can happen at any moment, your mood will appear normal.
Is pseudobulbar palsy a type of dementia?
Because of the substantial brain damage frequently underlying it, pseudobulbar palsy is connected with dementia as well as emotional ability. Likewise, when the left cerebral hemisphere is substantially affected, pseudobulbar palsy may be coupled with aphasia, generally of the non-fluent type
References
Pseudobulbar Palsy. (2025, November 10). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/pseudobulbar-palsy
Wikipedia contributors. (2025, April 4). Pseudobulbar palsy. Wikipedia. https://en.wikipedia.org/wiki/Pseudobulbar_palsy