Plantar Fasciitis
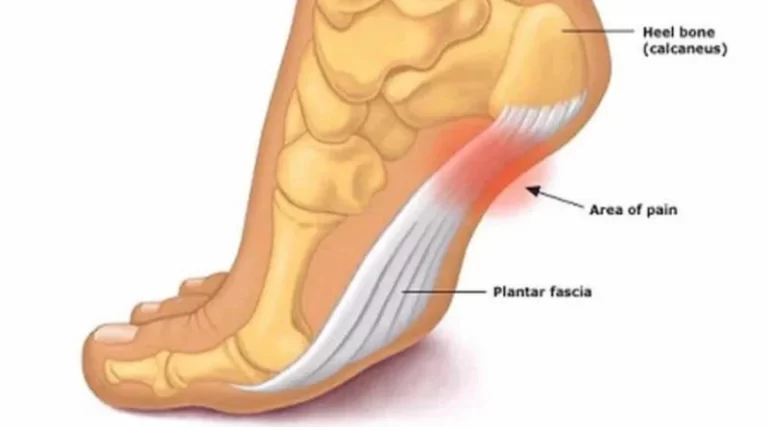
What is Planter Fasciitis? Plantar fasciitis is a common foot condition that causes heel pain at the bottom of the foot. It occurs when the plantar fascia—a thick band of tissue that runs along the sole—becomes inflamed or irritated. This tissue supports the arch of the foot and absorbs shock during movement. Repeated strain or…