Levator Scapulae Muscle
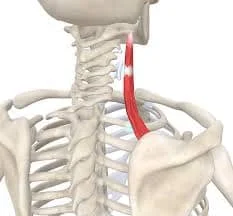
The levator scapulae muscle is a key anatomical structure located in the posterior region of the neck. As its name suggests, this muscle is responsible for elevating the scapula, or shoulder blade, hence playing a crucial role in shoulder movement and stabilization.
What Are Levator Scapulae Muscles?
The levator scapulae can extend and laterally flex the neck and additionally inferiorly rotate the glenoid cavity when used together with other posterior axial-appendicular muscles. Additionally, the levator scapulae facilitate the connection between the superior appendicular skeleton and the axial skeleton. Many illnesses, such as levator scapulae syndrome, flexion-extension syndrome, Sprengel deformity, cervical myofascial pain, and fibromyalgia, might involve the levator scapulae.
Structure of Levator Scapulae Muscles
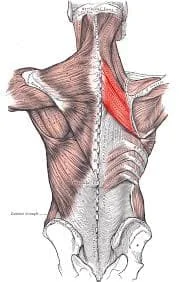
The posterior tubercles of the transverse processes of the C1 (atlas), C2 (axis), C3, and C4 vertebrae are the source of the levator scapulae muscle. Usually located between the superior angle and the root of the scapular spine, the muscle inserts on the posterior lip of the medial scapular border. The levator scapulae comprise a portion of the floor of the posterior triangle of the neck, and the sternocleidomastoid and trapezius muscles cover the superior and inferior portions of the scapulae, respectively.
Function Of Levator Scapulae Muscles
Elevating the scapula is the main function of the levator scapulae. The rhomboid and trapezius muscles work in line with the levator scapula during this exercise. The levator scapulae inferiorly rotate the scapula, depressing the glenoid cavity, as do the descending fibers of the trapezius, latissimus dorsi, rhomboids, pectoralis major, and minor, and gravity. Moreover, the levator scapulae muscle facilitates lateral flexion, ipsilateral rotation, and neck extension.
When the spine is locked, the levator scapulae elevate the scapula and move the inferior position directly. It frequently cooperates with other muscles, such as the pectoralis minor and rhomboids, to cause the scapula to rotate downward.
It would take muscles to anchor the cervical spine and keep it static so it does not bend or rotate to elevate or rotate one shoulder at a time. These forces would be offset by simultaneously elevating both with equal pulls on either side of the cervical spinal roots. Co-contraction of other muscles that raise the spine, such as the top fibers of the trapezius, an upward rotator, would inhibit downward rotation.
The cervical spine is flexed laterally and the levator scapulae rotate to the same side when the shoulder is stabilized. When both shoulders are stationary, straight cervical flexion or extension may result from the simultaneous, equal co-contraction of both levator scapulae muscles. However, neither lateral flexion nor rotation would be produced.
Origin
The posterior tubercle of the transverse process of cervical vertebrae 1 through 4 is where the levator scapulae starts.
Insertion
The muscle fibers descend laterally and insert between the superior angle and the base of the scapular spine, at the superior angle and medial border of the scapula.
Position
There are two deep spots in the levator scapulae, the inferior third is deep into the trapezius, and the superior third is deep into the sternocleidomastoid. The levator of the scapula fibers runs inferiorly from the upper cervical vertebrae’s transverse processes to the scapula’s superomedial border.
Nerve Supply
The levator scapulae are innervated by the dorsal scapular nerve (DSN), which derives from the C4 and C5 nerve roots. This nerve also supplies motor innervation to the rhomboids. The DSN arises from the anterior rami of the C5 root and the upper brachial plexus. It is often the first nerve branch to emerge from the root. Innervation from the cervical nerves (C3, C4) can also occur through the cervical plexus.
Blood Supply
The levator scapulae muscle’s main blood supply is the dorsal scapular artery. There is currently disagreement over the genesis in the literature. The subclavian artery is the most commonly mentioned origin, followed by a branch of the thyrocervical trunk. At the level of the levator scapulae, the transverse cervical artery, a branch of the thyrocervical trunk, splits into the superior and deep branches. The dorsal scapular artery is another name for the deep branch of the transverse cervical artery.
Lymphatic Drainage
The axillary and supraclavicular lymph nodes are typically connected to the shoulder blade. The right lymphatic duct receives the lymph nodes that drain from the right scapula. The thoracic duct receives direct drainage from the left scapula.
Embryology
The paraxial mesoderm is the source of the levator scapulae and the rhomboid major and minor muscles. Their development is stimulated by Wnt signaling and fibroblast growth factor (FGF) in tailbud neuroectodermal progenitors. originating from the dorsal scapular nerve, or the anterior (motor) nerves of C5.The spinal cord’s basal plate is where the anterior root develops.
Failed supraclavicular brachial plexus blocks may be related to the anatomic variance of the subclavian artery. Clinicians perform supraclavicular brachial plexus blocks to provide upper limb anesthesia and analgesia. The dorsal scapular artery, which is thought to be a variant branch of the subclavian artery that passes through the brachial plexus nerve bundle, is theorized in a case report by Kohli et al.
Anatomic Variation
The subclavian artery’s anatomic variance affects supraclavicular brachial plexus blocks that don’t work. Supraclavicular brachial plexus blocks are useful for analgesia and upper limb anesthesia. An ultrasound image of a different branch of the subclavian artery is presented by Kohli et al. They suggested that it could be the dorsal scapular artery crossing the brachial plexus nerve branch.
Surgical Considerations
Eden-Lange Procedure
The levator scapulae is not primarily used in many surgical operations. The goal of the 1924-described Eden-Lange operation is to restore the functionality lost in trapezius muscle palsy, also referred to as “winged scapula.” The rhomboids are linked to the infraspinatus fossa, and the tendon of the levator scapulae is moved to the acromion.
Modified Eden-Lange Procedure
The Redesigned Another method used to replicate native scapular placement is the Eden-Lange process. The surgeon attaches the rhomboid major to the infraspinatus fossa and the rhomboid minor to the supraspinatus fossa, rather than moving the rhomboid to the center of the scapula. The scapula’s spine is then joined to the levator scapulae muscle.
Thoracotomy
There have been reports that the levator scapulae are involved in thoracotomy procedures for lung excision. To prevent the functional effects of dynamic shoulder instability, it is necessary to identify and release a single deep aponeurosis that covers the levator scapulae and serratus anterior.
Clinical Significance
Scapulothoracic Articulation
The complex sliding junction known as the scapulothoracic articulation, combined with the glenohumeral, acromioclavicular, and coracoclavicular joints, makes up a portion of the shoulder. With its 17 muscle attachments, the scapula has a complex anatomical relationship.
These attachments work together to maintain the scapula dynamically and regulate the glenoid’s position, allowing the upper extremity to move freely across the glenohumeral joint. There are no ligamentous ties connecting the scapula to the thorax.
Because of the intricate nature of the scapulothoracic articulation, morphological changes in normal architecture can cause scapulothoracic diseases to be present and go undiagnosed or underappreciated.
Levator Scapulae Syndrome
Tenderness across the upper medial angle of the scapula, or levator scapulae syndrome, is the most prevalent clinical symptom of levator scapulae pathology. Despite having a long history, this illness is frequently ignored. Muscle-stretching motions frequently worsen symptoms.
It is hypothesized that a confluence of a bursa between the insertion of the levator scapulae, origin serratus anterior, and the scapula causes continual trigger points, crepitation, and enhanced heat emission. Local corticosteroid injections and physical therapy are effective forms of treatment.
Snapping Scapula Syndrome
Profound dysfunction of the shoulder may manifest as excruciating crepitus or scapulothoracic bursitis, sometimes known as “washboard syndrome” or snapping scapula syndrome. This disorder usually appears as a result of a long-term injury, excessive strain, or imbalance in the muscles that affect the scapulothoracic articulation.
The clinical presentation has also been linked to osseous lesions at the superomedial angle of the scapula as a result of recurrent injury or avulsion of the levator scapulae. Military soldiers may be particularly susceptible to this illness because of ongoing stress and repeated injuries brought on by upper extremity load-bearing exercises. With an 80% success rate, cautious treatment is usually used.
The most successful treatment option for patients who do not respond to conservative measures is arthroscopic bursectomy, either with or without partial scapulectomy.
Myofascial Pain
Cervical myofascial pain is a musculoskeletal disorder characterized by discomfort noticed in the surrounding fascia and muscles. One of the muscles in the cervical spine that is most frequently affected is the levator scapulae. Myofascial pain’s precise etiology is unknown, however, it is commonly brought on by trauma, poor posture, overuse of the muscles, or as a side effect of another medical disease like fibromyalgia or zygapophyseal joint arthropathies.
There are three types of cervical myofascial pain: trigger point-associated, localized, and regional. Hypersensitive regions in muscle tissue known as trigger points can cause pain when mechanically stimulated and can also transmit pain to nearby tissue. There are often trigger points in the levator scapulae, and a painful point in this area is often linked to the diagnosis of fibromyalgia
Other Clinical Considerations
Many examples of active levator scapula trigger points have also been reported; these include cases resulting from acute whiplash injuries. Dysfunction of the upper and middle cervical spine is correlated with pain at the place of insertion. The levator scapulae atrophy in patients with Sprengel deformity varies in severity.
Other Issues
Association with Posterior Triangle of the Neck
For anesthesiologists and surgeons, the posterior triangle of the neck, which is situated in the lateral cervical area, is a crucial anatomical position. This anatomic region contains the primary arterial structures of the neck and upper extremities, the deep cervical lymph nodes, the whole brachial plexus, and cervical sympathetic ganglions.
The area is traversed by other nerves, including the cutaneous cervical, vagus, phrenic, and spinal auxiliary nerves. The posterior triangle of the neck is formed by the trapezius behind and the sternocleidomastoid anterior, with the clavicle completing the base. The levator scapulae are a part of the floor close to the splenius, scalenus, and anterior scalene muscles.
The location of the levator scapulae in the posterior triangle of the neck is important for performing a cervical paravertebral block of the brachial or cervical plexuses utilizing a posterior method. A muscle-sparing needle trajectory is ideal in the posterior approach to the brachial or cervical plexuses to minimize pain and soft tissue damage during the treatment. The levator scapula and trapezius muscles may be the location of the needle implantation.
Medial Angle
The levator scapulae insert at the spinal vertebral angle, which is the angle at the medial border. Studies have shown that the right spine vertebral angle is larger than the left and that a change in angle can cause pathology in the levator scapulae due to a change in the insertion site’s orientation, which could lead to neck stiffness.
Assessment
When putting the patient in a supine position, supporting the ipsilateral scapula, and bending and rotating the head to the other side, one can measure the length and tension of the levator scapulae.
Additionally, this muscle has a lot of trigger points, which can be felt in the superior and inferior attachments.
Exercise
Levator Scapulae Muscles stretching exercise
STANDING ASSISTED LEVATOR SCAP STRETCH

- Place your feet shoulder-width apart and hold yourself up tall.
- With the top of your hand at the lower part of your back, place your left arm behind your back.
- Press your chin to your chest.
- Turn your chin in the direction of your right armpit.
- To help with the stretch, raise your right arm above your head and rest it on your head.
- Change sides and reset to the center.
SEATED ASSISTED LEVATOR SCAP STRETCH

- With your feet flat on the floor, take a tall seat on a chair’s edge.
- To stabilize your left shoulder, reach under the chair and grip onto your left arm.
- Turn your chin in the direction of your right armpit.
- To help with the stretch, raise your right arm above your head and rest it on your head.
- Change sides and reset to the center.
STANDING MODIFIED LEVATOR SCAP STRETCH

- Place your feet shoulder-width apart and hold yourself up tall.
- With your elbow slightly bent, extend your left arm across your body.
- To keep your left shoulder stable, take hold of your left wrist with your right arm and tense up a little bit.
- Press your chin to your chest.
- Turn your chin in the direction of your right armpit.
- Change sides and reset to the center.
STANDING BANDED LEVATOR SCAP STRETCH

- Place your feet shoulder-width apart and hold yourself up tall.
- With the top of your hand at the lower part of your back, place your left arm behind your back.
- Press your chin to your chest.
- Turn your chin in the direction of your right armpit.
- To help with the stretch, raise your right arm above your head and rest it on your head.
- Change sides and reset to the center.
LEVATOR SCAP TRIGGER POINT RELEASE

- Apply pressure with your palm to the area of the levator scapulae that is most tense.
- After locating a trigger point, utilize a trigger point ball to further identify the knot.
- Position the ball on your trigger point and lean against a wall to roll it up, down, and side to side.
- Pause and lean into the trigger point when you detect a tender place.
- Hold for a duration of 15 to 60 seconds.
- Try alternating between a static hold and a vigorous roll until the area starts to feel better.
- For a total of two to five minutes on each side, work on one side at a time.
Levator scapulae stretching in a sitting position on the bench
As you sit on the side edge of the bench, make sure your right arm is away from your body and your shoulder is down. Hold the bottom of the bench with your right hand.
Now bring your head forward and bend it toward your chest.
Next, rotate and bend your neck to the side and tuck your chin under your left armpit.
To aid with the stretch, raise the left hand onto the side of the head.
Go back to the beginning and do it again.
Levator scapulae stretching in sitting or standing
The patient can stretch while sitting or even while standing.
Look down at the floor and to your right hip while maintaining the downward position of your stretched left shoulder.
Stretch the patient when it is comfortable, hold the stretch for 20 seconds, and then release the tension.
To further lower the shoulder, the patient might also sit on the left hand.
To achieve a deeper stretch, pull the head towards the ground with your right arm.
Levator scapulae stretching with a band
On the left side—the side that is being stretched—step on the strong band.
Hold the band firmly in your left hand so that it can support your right arm and shoulder.
Bend the head to the side in the direction of the anchoring side’s right shoulder. Then, watch at the front pocket by tucking the chin in toward the right side.
On the same side as the band, the patient can feel a comfortable stretch above the scapula and on the left side of the neck.
Maintain this stance and carry out the exercise again on the right side by placing your left foot on the band.
Levator Scapulae Muscles strengthening exercise
Dumbbell Shrugs
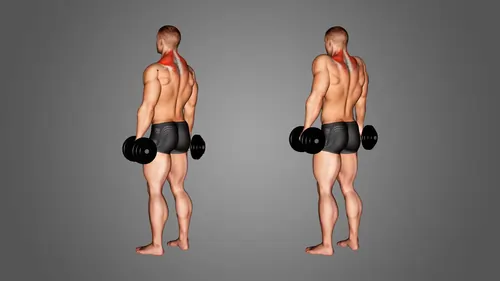
- Make sure your feet are shoulder-width apart before beginning this exercise.
- With each hand, hold a single dumbbell.
- As though shrugging your shoulders, pull your shoulders up near your ears.
- Perform fifteen repetitions in three sets twice a week.
Lateral Raises
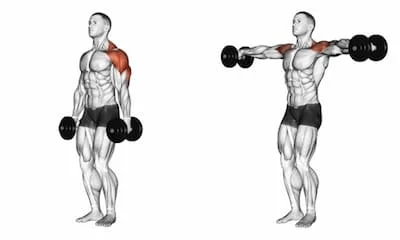
- Place both hands on a dumbbell and place your feet shoulder-width apart.
- Lower dumbbells after raising arms laterally until the elbow and shoulder are level.
- Perform fifteen repetitions in three sets twice a week.
Summary
The flat bones that comprise the shoulders are known as scapulae, or shoulder blades in everyday speech. The levator scapulae muscle, a thin long, superficial neck muscle, elevates each scapula structurally. The levator scapulae muscle extends to the rear sides of the neck where it attaches.
The levator scapulae muscles collaborate with other muscles such as the trapezius and rhomboids to move and support the neck. For example, the levator scapulae muscles prevent the neck from over-flexing when the neck flexes laterally, or bends directly to the left or right, using the scalene muscles.
FAQ
What is the levator scapulae muscle used for?
It turns the scapula downward, and the levator scapulae elevate it and tilt the glenoid cavity inferiorly. When the scapula is locked, the cervical vertebral column flexes laterally to the side, and the levator scapulae contract to stabilize the vertebral column during rotation.
What is the levator scapulae’s primary function?
The levator scapulae is a broad superficial muscle that moves from the cervical vertebrae to the scapula on the other side of the neck. Its main function is to raise the scapula, although it rotates the shoulder and tilts the head.
How do you strengthen the levator scapulae?
Make sure your feet are shoulder-width apart before beginning this exercise. With each hand, hold a single dumbbell. As though shrugging your shoulders, pull your shoulders up near your ears. Perform fifteen repetitions in three sets twice a week.
What causes levator scapulae pain?
The most common cause of levator scapulae syndrome is bad shoulder position. For instance, movement over and rounding your shoulders while using a computer. This position extends the levator scapulae muscle, which may become inflamed and painful if held for a long period.
Can you damage your levator scapulae?
Shoulder bad posture is the usual cause of levator scapulae syndrome. For example, you should roll your shoulders and stoop when using a computer., for instance. Stretching the levator scapulae muscle over a longer period may result in pain and inflammation in the muscle
How do you reduce levator scapulae?
Two potential therapy options include posture guidelines to reduce the strain on the levator scapulae and stretching to relieve tension. The levator scapulae benefit from Active Release Techniques (ART).
Why is my levator scapulae always tight?
The disease is more common in office workers because they often sit for extended periods with their head and shoulders thrusting forward, resulting in a “hunch back” posture at the joints of the lower and upper neck, which in time becomes stiff and inflexible.
What is the best sleeping position for levator scapulae pain?
Techniques for sleeping on your back shoulders, or neck are stiff. Try sleeping on your back or the other side to prevent irritating your painful shoulder. Try placing a pillow next to your aching shoulder if you’re on your back to deter yourself from rolling that way in the middle of the night.
How do you test for levator scapulae pain?
When putting the patient in a supine position, supporting the opposite scapula, and bending and rotating the head to the other side, one can measure the length and tension of the levator scapulae. Additionally, this muscle has a lot of trigger points, which can be felt in the superior and inferior attachments.
What is the synergist of the levator scapulae?
Elevation, adduction, and downward rotation of the scapula can be achieved by performing a concentrated contraction of the levator scapulae muscle while the spine is fixed. Sahrmann4 states that for scapular lift and adduction, this muscle works in concert with the upper trapezius, while in scapula rotation, it opposes the latter.
What are the muscles of the scapulae?
The rear of the shoulder girdle is formed by the scapula. It is a strong, triangular, flat bone. Numerous muscle groups are attached to the scapula. The rotator cuff muscles, teres major, subscapularis, teres minor, and infraspinatus are the muscles that make up the scapula’s intrinsic muscles.
What are the attachments of the levator scapulae muscle?
The back’s extrinsic muscle is the levator scapulae. It connects the upper limb to the spinal column and is located in the posterior triangle of the neck. Attachments: Joins the medial edge of the scapula to the transverse processes of the C1–C4 vertebrae. Movement: Shaping of the shoulder blades.
What nerve controls the levator scapulae?
The levator scapulae, rhomboid major, and rhomboid minor muscles are innervated by the dorsal scapular nerve, a motor nerve. These muscles are referred to as periscapular stabilizing muscles because of their collective and dynamic action. They each can raise and retract the scapula.
3 Comments