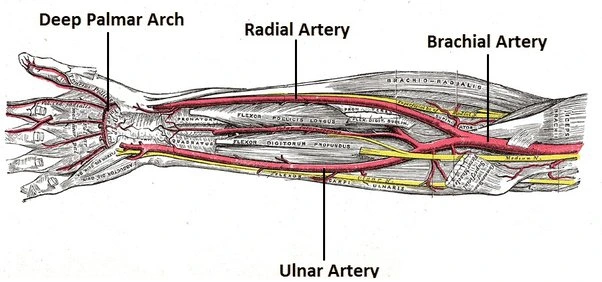
Ulnar Artery Thrombosis
What is an Ulnar Artery Thrombosis? Ulnar artery thrombosis is a condition where a blood clot forms in the ulnar artery, leading to reduced blood flow to the hand. It can result from trauma, repetitive stress (as seen in hypothenar hammer syndrome), or underlying vascular disorders. Symptoms include pain, cold intolerance, discoloration, and weakness in…