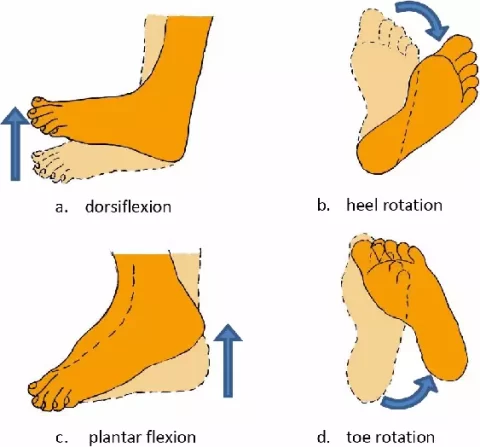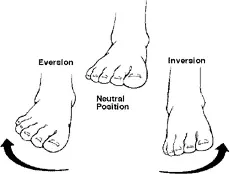
Ankle Inversion
Ankle Inversion Ankle inversion refers to the movement where the sole of the foot turns inward, typically towards the midline of the body. It involves the contraction of muscles like the tibialis posterior and anterior, and is essential for activities like walking, running, and maintaining balance. Ankle Eversion and Inversion: What Are They? Movements of…