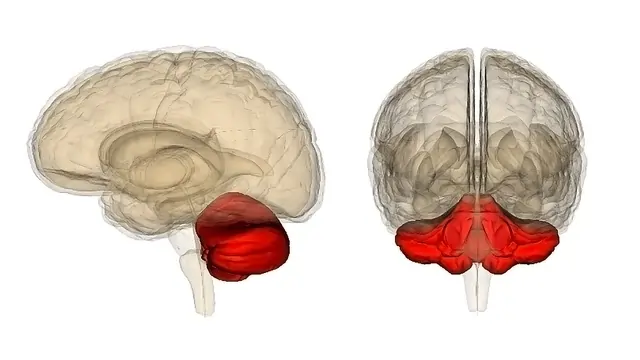
Autosomal Recessive Cerebellar Ataxia
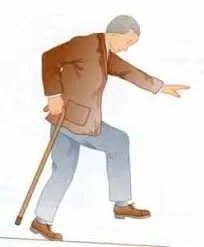
Introduction: The disorder known as autosomal recessive cerebellar ataxia type 1 (ARCA1) is characterised by developing mobility issues. Early to mid-adulthood is when the disorder’s signs and symptoms initially manifest. Dysarthria, a speech disability, ataxia, a balance and coordination problem, or both are among the disorder’s early signs. Additionally, they could struggle with movements that…