Deltoid Muscle
What is the Deltoid muscle?
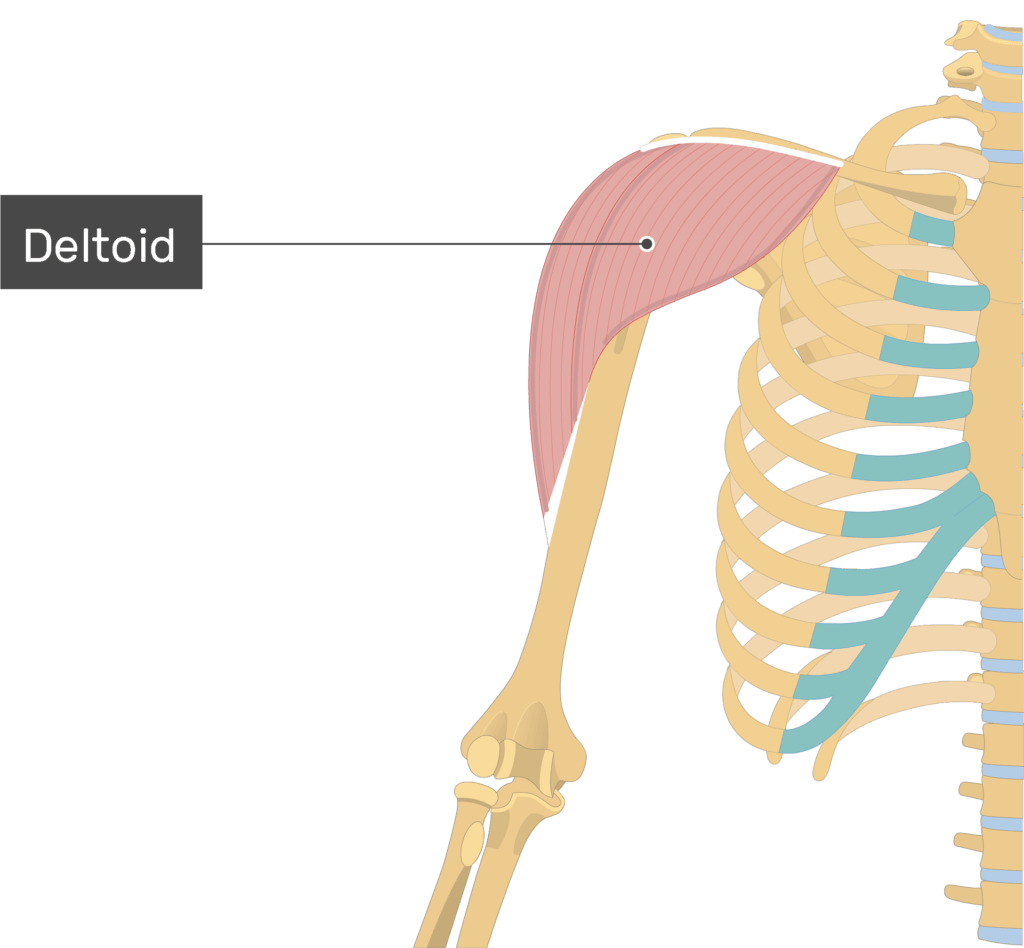
The deltoid muscle is a key player in the complex system of muscles that comprise the human shoulder. Named after the Greek letter delta (Δ) due to its triangular shape, the deltoid is one of the major muscles responsible for the mobility and stability of the shoulder joint.
The name “deltoid” describes the shape of this huge, triangular, intrinsic shoulder muscle, which is shaped like the Greek letter delta reversed. This muscle, which is thick and dispersed anteroposteriorly, shapes the rounded shape of the shoulder.
Surface Anatomy of the Posterior Aspect of the Right Upper Extremity is the location where Immunizations and other intramuscular injections are frequently given into the deltoid.
A vital part of shoulder motion and stability is the deltoid muscle. Injuries to the rotator cuff may need the deltoid to compensate for the weakened shoulder. Trauma and ongoing wear and tear are common causes of conditions affecting this muscle.
Deltoid patches can be utilized in surgery to fix shoulder deformities caused by breast cancer treatment. To diagnose and treat a variety of arm and glenohumeral joint disorders, it is essential to comprehend this muscle’s anatomy and clinical value.
Anatomy of Deltoid Muscle
Origin
The majority of the anterior border and upper surface of the lateral part of the clavicle is where the anterior, or clavicular, fibers originate. Both the anterior origin and the end tendons of the two muscles are situated next to the lateral fibers of the pectoralis major muscle.
The cephalic vein runs across a little chiasmatic space, which separates the two muscles from creating a single, continuous muscle mass, indicating how closely connected these muscle fibers are.
The superior surface of the acromion process of the scapula is where the middle, or acromial, fibers originate.
The lower lip of the posterior border of the scapular spine is where posterior or spinal fibers originate.
Insertion
The fibers converge from this broad origin towards their insertion on the deltoid tuberosity in the middle of the lateral aspect of the humerus shaft; the anterior and posterior fibers pass laterally and obliquely, respectively, while the middle fibers pass vertically.
The deltoid insertion is separated into two or three distinct locations that correspond to the three areas of origin of the muscle while being conventionally classified as a single insertion. The insertion is a structure that forms an arch, bordered by an intervening tissue bridge with strong anterior and posterior fascial connections.
It also radiates outward to the deep brachial fascia. In addition, the deltoid fascia is linked to the lateral and medial intermuscular septa and forms a portion of the brachial fascia.
Blood supply
Because of its size, the deltoid muscle has a large circulatory supply from a variety of sources.
The axillary artery branches into the thoracoacromial artery (acromial and deltoid branches).
An outgrowth of the axillary artery is the subscapular artery.
Anterior circumflex artery of the humerus
Hulzer’s posterior circumflex artery
Brachial artery deepening
Except for the profunda brachii, a branch of the brachial artery that is the axillary artery’s continuation inside the arm, all of the arteries supplying the deltoid are branches of the axillary artery.
Lymphatics
The lymphatic drainage from the muscle flows into the deltopectoral lymph nodes, which are located in the deltopectoral groove next to the cephalic vein.
Nerve supply
The axillary nerve innervates the deltoid. The posterior division of the superior trunk, the posterior cord of the brachial plexus, the superior trunk, and the anterior rami of the cervical nerves C5 and C6 are the origins of the axillary nerve.
The deltoid muscle is composed of seven neuromuscular segments, according to studies. Of these, three are located in the deltoid’s anatomical anterior head, one in the anatomical middle head, and three in the anatomical posterior head.
These neuromuscular segments work in tandem with the supraspinatus and pectoralis major muscles of the shoulder girdle. They are supplied by smaller branches of the axillary nerve.
Sometimes axillary surgeries, such as those for breast cancer, result in injury to the axillary nerve. The anterior dislocation of the humeral head can potentially cause damage to it.
Related Muscles
To move the upper limb and stabilize the shoulder, the deltoid muscle collaborates with the supraspinatus, infraspinatus, teres minor, and subscapularis, the four rotator cuff muscles.
When the deltoid abducts the arm past 15°, these muscles support the glenohumeral joint and start abduction from 0° to 15°. The only rotator cuff muscle that does not rotate the humerus is the supraspinatus.
Abduction is initiated by the supraspinatus, which also supports the deltoid in abduction to greater angles.
Structure of Deltoid Muscle
The medullary parts that make up the shoulder girdle are the clavicle, scapula, and proximal humerus. Conversely, the following muscles are found in this area:
Deltoid
muscles of the rotator cuff, such as the teres minor, subscapularis, supraspinatus, and infraspinatus
The muscles of the posterior axioappendicular region comprise the serratus posterior, rhomboids, levator scapulae, latissimus dorsi, and trapezius.
Triceps Brachii
Both major and minor pectoralis
The deltoid has three sections:
- Anterior (clavicular)
- Lateral (acromial)
- Posterior (spinal)
The lateral section is multipennate, whilst the anterior and posterior regions are unipennate. These three pieces work together to produce a triangle muscle.
The scapular spine, superior acromial surface, and lateral third of the clavicle are the origins of the deltoid muscle.
As a result, the proximal attachment of this muscle is U-shaped, similar to the distal insertion of the trapezius muscle. The deltoid connects itself distally to the humerus’s deltoid tuberosity.
Function of Deltoid Muscle
The deltoid is the primary muscle responsible for arm abduction in the frontal plane when all of its fibers contract at the same time. To get the most out of the deltoid, the arm has to be turned medially.
Because of this, during arm adduction, the deltoid is an antagonist muscle of the latissimus dorsi and pectoralis major. The pectoralis major uses the anterior fibers to help flex the shoulder. The subscapularis, pecs, and lats collaborate with the anterior deltoid to internally (medially) rotate the humerus.
When the shoulder is rotated internally, the intermediate fibers execute basic shoulder abduction; when the shoulder is rotated externally, they complete shoulder transverse abduction.
When the shoulder is internally rotated during tight transverse extension, as in rowing activities, they are not used as much because the posterior fibers are used instead.
To extend the shoulder, the latissimus dorsi is helped by the posterior fibers.
Together with the posterior deltoid, other transverse extensors, the infraspinatus and teres minor, function as external (lateral) rotators that oppose powerful internal rotators like the pecs and lats.
Preventing the humeral head from dislocating while a person is carrying large loads is one of the deltoid’s major functions in humans. Because of the way abduction works, it would also assist in carrying items farther away from the thighs so they wouldn’t strike them, as on a farmer’s stroll.
It also guarantees the glenohumeral joint’s accurate and quick mobility, which is necessary for manipulating the hands and arms. Although the anterior and posterior fibers simultaneously co-contract to aid with this function, as with fundamental abduction motions, the intermediate fibers are most suited for it.
When the deltoid muscle contracts, the arm is raised in the scapular plane, which also raises the humeral head.
There is a simultaneous contraction of several rotator cuff muscles, mainly the infraspinatus and subscapularis, to prevent this from compressing on the undersurface of the acromion of the humeral head and harming the supraspinatus tendon.
Despite this, the head of the humerus may still migrate 1-3 mm upward during the first 30–60 degrees of arm elevation.
Embryology
The deltoid and other striated muscles of the trunk and limbs originate from the segmented paraxial mesoderm. Stomata are the bilaterally paired blocks into which the paraxial mesoderm separates.
During the fifth week of development, myogenic precursors, or myoblasts, in the somites travel toward growing limb buds.
The dorsal and ventral muscle masses are the two main groups of these myoblasts that condense in the dorsal and ventral limb buds. From the dorsal muscle mass, the deltoid muscle develops.
Anatomical Variations
There have been reports of uncommon anatomical deltoid variations in the literature. There are multiple case reports describing distinct fascial sheaths on the posterior aspect of the deltoid.
In a different one, the posterior deltoid may resemble the teres minor and is entirely isolated from the other muscles.
These variations could be confusing for surgeons and surgical personnel while doing posterior deltoid flap surgeries, thus they need to be known.
Significant surgical ramifications could potentially result from an abnormal placement into the humerus’s medial epicondyle. This variation increases the risk of caused by neurovascular injury because the deltoid fibers run superficially to the brachial artery, ulnar nerve, and median nerve.
There have also been reports of abnormal deltoid straps. It was discovered that the abnormal straps ran perpendicular to the posterior deltoid fibers, which could be confusing for flap surgery patients.
Variants of the thoracoacromial artery are also reported in the research. The artery in the type I version burrows into the deltoid muscle after bridging the deltopectoral gap.
In the type II form, the artery passes via the cephalic vein, crosses the deltopectoral gap, and then returns to the pectoralis major.
Clinical Importance
A clinical test for deltoid function involves elevating the patient’s arm to a 15° angle. An alternate is abduction against resistance.
Patients without injury to the deltoid or axillary nerves will not exhibit lateral deltoid contraction, while those with normal muscle function will.
Overuse of crutches, surgery, and posterior shoulder dislocation following severe trauma are common causes of axillary nerve palsy.
The deltoid is most frequently abnormally affected by tears, fatty atrophy, and enthesopathy. Uncommon deltoid muscle injuries are often associated with large rotator cuff tears or traumatic shoulder dislocations.
Several factors, such as aging, inactivity, denervation, cachexia, muscular dystrophy, and causal injury, can lead to muscle atrophy. An extremely rare disorder associated with mechanical stress is called deltoid humeral enthesopathy.
On the other hand, deltoid acromial enthesopathy is presumably a sign of seronegative spondyloarthropathies, and any relevant clinical and serological investigations should likely be conducted after its diagnosis.
Diagnosed
It’s not necessarily a sign of a deltoid muscle injury if you are unable to raise your arm. Weakness in the arm muscles can also occur from:
Cachexia is the severe loss of muscle brought on by illness or a bad diet.
Myopathies, or neuromuscular disorders, are types of muscle disorders.
adverse reactions to a vaccination.
Imaging tests may also be suggested by your provider. If they think your shoulder has any bone fractures, dislocations, or tears in the tissue, they might order an MRI, CT, X-ray, or ultrasound. An electromyogram (EMG) examines the function of your nerves and muscles.
Surgical Considerations
When performing treatments with an anterior approach, deltoid manipulation is important to take into account because it provides superior access to the shoulder joint. The following procedures need deltoid manipulation:
Recurrent anterior shoulder instability is an indication that an open Bankart capsular repair is necessary.
Shoulder arthroplasty: suggested for advanced degenerative arthritis, avascular necrosis, and post-traumatic deformity. comprises reverse complete shoulder arthroplasty, hemiarthroplasty, and total shoulder arthroplasty.
Tenotomy, tenodesis, and repair of the biceps long-head tendon are indicated in cases of end-stage tendinopathy of the long head and instability of the biceps long-head tendon or bicipital groove.
Even though the majority of rotator cuff repair surgeries are now done arthroscopically, the current indications for these treatments are still somewhat debatable.
The mini-open approach (lateral deltoid-splitting approach) is a well-liked substitute for the deltopectoral approach.
Ruptures of the cephalic vein and injury to the axillary nerve are possible side effects of deltoid manipulation.
Deltopectoral Approach
Using this approach, the route of the surgical incision is first marked on the skin by the coracoid process. subsequently, the deltopectoral groove is incised.
The center of the deltoid and pectoralis major fibers is where you should notice the “fat stripe,” which contains the cephalic vein.
Next, the pectoralis major retracts medially, and the deltoid retracts laterally. The direction of the cephalic vein’s retraction depends on the surgeon’s preference.
Alternatives to the Deltopectoral Approach
If the deltopectoral approach to shoulder surgery is not possible, then the anterolateral and direct lateral techniques may be used.
For instance, in some circumstances, a modified anterolateral approach may provide better access than an anterior approach to particular fracture parts.
Repairing the rotator cuff and advancing anterior shoulder joint decompression are the main goals of the anterolateral approach to the acromioclavicular joint and subacromial area.
The anterolateral surgical technique is very helpful in exposing the posterior side of the shoulder, as per a 2018 study.
The coracoid process and the acromion serve as the incision landmarks in this approach.
The acromioclavicular joint is shown, and the deltoid is then retracted. While repairing a rotator cuff, the muscle is split.
Complications of Deltoid Manipulation
When this muscle needs to be manipulated during shoulder surgery, a deltoid injury may result. One such is the separation of the deltoid muscle from the clavicle.
Complete healing takes four to six weeks, along with full-thickness and transosseous sutures for reunion.
Damage to the axillary nerve is yet another possible side effect of these operations. The nerve runs posteroanteriorly, passing beneath the deltoid muscle.
The nerve could be unintentionally injured by an anterior deltoid retraction or incision. Damage to the axillary nerve might impair feeling across the deltoid and arm abduction beyond 15°.
Inadequate surgical technique can also result in cephalic vein rupture and upper limb edema.
Other Issues
The incapacity to abduct the arm is not a distinctive sign of a localized deltoid pathology because it can also be a symptom of proximal neuromuscular disorders and systemic processes.
The following are included in the differential diagnosis of deltoid disorders:
- symptoms of Lambert-Eaton myasthenic
- Inflammatory processes of the muscles, such as polymyositis and dermatomyositis
- The typical presentation of polymyalgia rheumatica is stiffness as compared to weakness.
- Adverse reaction to vaccinations using the metal hydroxide
- Nutritional deficiencies or chronic illness-related the condition
The incapacity to abduct the arm or proximal muscular weakness are common presentations of these disorders. Correct diagnosis and differences of various deltoid problems are helped by a comprehensive clinical test.
Palpation
When the patient’s elbow reaches 90 degrees, have them abduct their shoulder against the opposition.
Anterior Fibers: Palpated Deltoid with elbow extended, shoulder abducted 90 degrees, and resistance to horizontal adduction.
Maintain the same posture as before and fight horizontal abduction with the posterior fibers.
Length Tension Testing
Anterior Deltoid
The patient will be seated in a high position.
With the testing shoulder in hand, the therapist will be behind the patient.
To stretch this muscle, reverse the movement by performing extension, external rotation, and horizontal abduction shoulder without allowing the body to spin.
The anterior deltoid muscle’s principal functions are flexion, internal rotation, and horizontal adduction.
Place one hand on the patient’s forearm and use the other to press the shoulder anteriorly from the posterior while completing extension and external rotation to extend the muscle.
Posterior Deltoid
The patient will be seated in a high position.
The therapist will stand in front of the patient, and then go back to them for a more thorough examination of their length.
Reverse the motion by flexion, internal rotation, and horizontal adduction of the shoulder joint to stretch this muscle.
Extension, external rotation, and horizontal abduction are the three main actions of the posterior deltoid muscle.
Place one hand on the patient’s shoulder and the other on the forearm as you do flexion, internal rotation, and horizontal adduction.
As an alternative, place the patient’s shoulder against your chest and have the therapist move to the back of the patient while holding their forearm and shoulder to extend the muscle.
This will result in flexion, internal rotation, and horizontal adduction of the shoulder.
Exercises of Deltoid Muscle
Stretching Exercise of Deltoid muscle
Standing chest and shoulder stretch
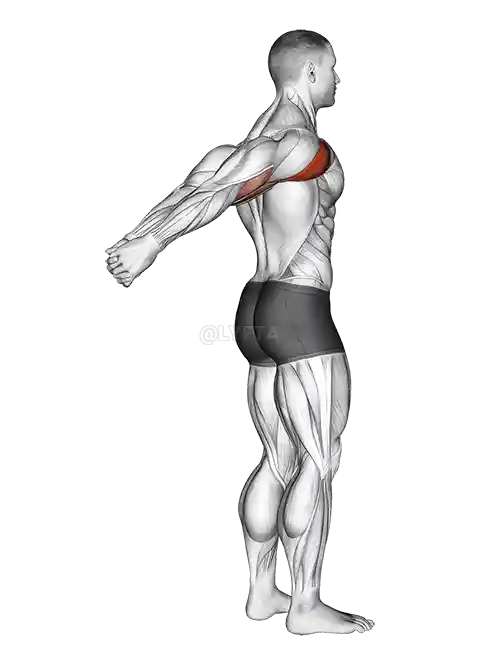
Maintain a standing position with your shoulders back, your core tight, and your feet about hip distance apart. Focus on maintaining good posture.
Place your hands together by stretching both arms behind your back.
Breathe in, and then as you release, raise your hands behind your head as high as is comfortable, until your chest and shoulders feel well stretched.
Hold the position, breathing deeply for 30 seconds. Release, then repeat two more times.
Cross-body shoulder stretch
Using your feet hip-distance apart and your core tight, take a high stand.
Place your ears on top of your hips, knees, ankles, and shoulders.
Reach past your right shoulder and extend your left arm shoulder height across your body. Grip your left forearm with your right hand.
When you feel a stretch in the area of your left shoulder that goes toward the midsection, slowly bring your left arm closer to your body.
For 30 seconds, hold this posture while taking deep breaths.
After taking a break, continue two more times, then switch sides.
Dynamic bear hug stretch

With your feet about shoulder-width apart, your posture straight and tall, and your core tight, stand tall.
As if you were going to hug someone, extend your arms wide.
Hugging yourself with your right arm on top of your left, bring your arms across your chest until you feel a slight stretch across the middle of your shoulders. This will happen when you feel a stretch across the front of your shoulders and chest.
Swing your arms wide again in a controlled motion.
This time, before you swing your arms, reach the end of your range of motion and return to the hugging position, placing your left arm over your right.
Continue for 30 seconds. Rest, then repeat two more rounds.
Strengthening exercise of Deltoid muscle
Dumbbell front raise
Hold dumbbells in front of you while standing, with your hands facing your legs.
Stretch your arms straight up to shoulder height while bending your knees and elbows just a little bit.
Slowly return to the starting position.
Initially 2 sets of 10 reps. Rest about 40 seconds between sets.
Move up and down at an even pace. Two seconds up, two seconds down. Maintain your elbows from locking out or slouching during performance.
Try combining front, lateral, and reverse fly shoulder raises into one sequence, reducing the rest time between sets to 30 seconds.
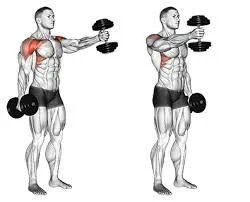
Dumbbell lateral raise
Standing with your palms facing each other, hold dumbbells.
Maintaining a small bend in your elbows and knees, raise your arms in wide arcs from your sides to around shoulder level.
Slowly return to the starting position.
Four sets of 12 reps. Rest about 60 seconds between sets.
Move up and down at an even pace. Two seconds up, two seconds down. keep from leaning back or locking your elbows during execution.
Reverse fly

In the Standing position.
While your palms facing each other, hold dumbbells.
Your torso should be at a 45-degree angle with the ground as you bend forward.
Hold the dumbbells up and out to the sides until they are parallel to the floor while maintaining a slight bend in your elbows. Concentrate on pressing your shoulder blades together as you raise the weights.
Four sets of 12 reps. Rest about 60 seconds between sets.
Throughout the activity, maintain a solid, neutral posture for your spine. Use an incline bench to support yourself if you are not strong enough to perform this today.
Try combining front, lateral, and reverse fly shoulder raises into one sequence and reducing the rest time between sets to 30 seconds
Summary
The primary shoulder muscle is the deltoid. The anterior, lateral, and posterior deltoids are its three heads. The three heads work together to support the shoulder joint and move the arm.
Additionally, every head has a unique set of attachment points and may perform a variety of motions, including abduction, flexion, extension, and rotation.
Surgery may result in direct or indirect damage to the deltoid muscle. Rehabilitation could be required in certain situations to regain strength, range of motion, and flexibility.
FAQ
What is the definition of a deltoid?
The muscle that gives the human shoulder its rounded shape is the deltoid muscle. It is sometimes referred to as the “common shoulder muscle,” especially when referring to domestic cats and other similar animals.
Where is the landmark for the deltoid muscle?
The form of the deltoid muscle is a rounded triangle. The patient should be seated comfortably and have visibility of their arm from the shoulder to the tip of the elbow to define this location. Trace an imaginary inverted triangle beneath the shoulder by palpating the acromion, or outer edge of the scapula.
What is the antagonist of the deltoid muscle?
The primary mover for arm abduction is the midsection of the deltoid muscle. The latissimus dorsi is the antagonist posteriorly, and the pectoralis major is the antagonist anteriorly against the middle deltoid.
What is the deltoid muscle in a female?
There are three heads to the shoulder deltoid muscle: the anterior, or front, medial, or side, and posterior, or rear deltoids. By engaging in deltoid workouts, women can increase the strength of these muscles and enhance the function and range of motion of their shoulders.
What shape is a deltoid?
The deltoid is a thick, triangular shoulder muscle. Its name comes from its shape resembling the Greek letter “delta” (Δ). The origin of the muscle is broad, extending to the clavicle, acromion, and scapular spine. It passes inferiorly around the glenohumeral joint on all sides before entering the humerus.
What is the origin of deltoid muscle?
The acromion process of the scapula (shoulder blade), the spine, and the lateral portion of the clavicle (collarbone) are the origins of the deltoid muscle. The muscle then extends down the arm from these locations of origin to implant on the deltoid tuberosity of the humerus, which is the long bone in the upper arm.
What is the main cause of deltoid pain?
Deltoid tendonitis, an inflammation of the rotator cuff and the surrounding muscles and tendons, is a common cause of pain in the deltoid muscle. Deltoid tendonitis is a repetitive stress injury that is frequent in athletes and those with physically demanding employment. The intensity of it might vary from moderate to severe.
What is deltoid weakness?
Muscle degeneration in the deltoid region is known as deltoid atrophy. The muscle shrinks and loses strength. There may be a discernible variation in the size of one deltoid from the other if it just affects one side. The muscle is weaker because it is smaller.
Do deltoids make you look bigger?
The large, complex shoulder muscles known as the “delts” are made up of the front, middle, and rear deltoids. They complement the back, arm, and chest muscles well to create the impression of a powerful upper body. Use shoulder exercises like incline presses, front raises, upright rows, and overhead presses to bulk them up.
What is the action and nerve supply of the deltoid?
When the posterior deltoid contracts, the arm travels forward and backward. The acromial artery, deltoid artery, posterior circumflex humeral artery, and anterior circumflex humeral artery all give blood to the deltoid muscle. It has axillary nerve innervation.
What is the insertion of the deltoid?
All of the head’s fibers come together to insert into the humerus’ deltoid tuberosity. The medial and lateral intermuscular septa are connected to the deltoid fascia, which is continuous with the brachial fascia.
What type of muscle is the deltoid?
The ball-and-socket joint in your shoulder that joins your arm to your body’s trunk houses your deltoid muscles. Your deltoid muscles enable you to move your arms in various planes. Additionally, they stabilize and safeguard your shoulder joint. The deltoids are skeletal muscles, just like the majority of other muscles in your body.


13 Comments