Teres Major Muscle
The teres major muscle, despite its relatively small size, plays a significant role in the movement and stability of the shoulder joint. Situated in the upper back region, it forms part of the rotator cuff group, which comprises muscles crucial for shoulder function.
What Is The Teres Major Muscle?
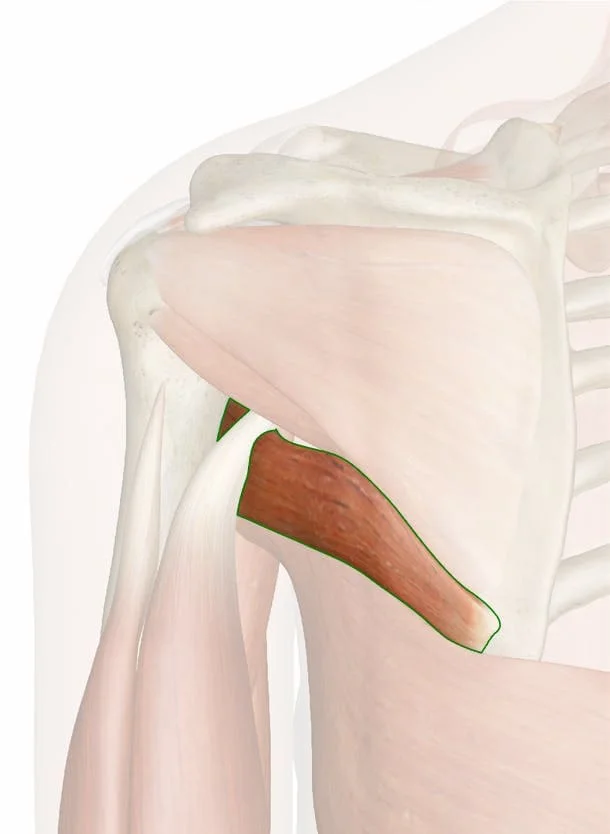
Stretching from the inferior posterior scapula to the medial lip of the humeral intertubercular groove, the teres major is a thick, rectangular muscle that has been flattened. It works in concert with the latissimus dorsi to twist the humerus internally and addictively.
Even though the latissimus dorsi and teres major muscles frequently work together, injury to one muscle alone can also happen. Although they are uncommon, teres major injuries can result from impact or strain trauma.
The lateral edge of the scapula is accompanied by a little muscle known as the teres major (TM). Its synergistic effects have earned it the nickname “Lat’s little helper” at times.
The rotator cuff’s teres minor is an elongated, thin muscle. The word “teres” comes from the Latin word “rounded.” The muscle inserts at the larger tubercle of the humerus as well as the posterior side of the joint capsule. It starts at the lateral border and adjacent posterior surface of the corresponding right or left scapula.
The teres minor’s main job is to control the deltoid’s motion, which keeps the humeral head from sliding upward while the arm is abducted. It also has the role of laterally rotating the humerus.
Structure of the Teres Major Muscle
The medial lip of the humerus’s intertubercular groove is where the teres major inserts after starting on the posterior aspect of the inferior angle of the scapula. Before attaching to the humerus, it passes anterior to the triceps long head and inferior to the teres minor.
Together with the latissimus dorsi and subscapularis muscles, the teres major forms the posterior wall of the axilla and is situated deep within the deltoid muscle.
The latissimus dorsi runs along the inferior border of the teres major after starting inferior to it. The latissimus dorsi then moves superiorly to implant at the lip of the humerus’s intertubercular groove, which is the same location on the humeral head as the teres major.
Studies have shown that the latissimus dorsi and teres major tendons united before they were inserted into the humerus. These tendons often connect close to the insertion point.
The pectoralis major inserts at the same location as the teres major and latissimus dorsi, albeit more laterally, on the lip of the humerus’ intertubercular groove.
For the top two-thirds of its length, it originates from the dorsal surface of the axillary border of the scapula. It also derives from two aponeurotic laminae, one of which divides it from the teres major muscle and the other from the infraspinatus muscle.
Its strands extend laterally and obliquely upward; the top strands terminate in a tendon that is inserted into the lowermost of the three impressions on the humerus’s larger tubercle, while the lower strands are inserted straight into the bone just below the impression.
Function of the Teres Major Muscle
The teres major is responsible for extending, rotating medially, and adducting the humerus. It also contributes to the humeral head’s stability. These are not the only tasks performed by this muscle. The adduction of the humerus and medial rotation are further assisted by the latissimus dorsi. Electromyographic investigations demonstrate that these two muscles work in concert to produce these results, activating as a single muscular unit.
The humeral head is also adducted by the pectoralis major. The teres major helps the supraspinatus, infraspinatus, subscapularis, and teres minor muscles of the rotator cuff to stabilize the humeral head.[8] These muscles work together to keep the humeral head from subluxing.
As components of the rotator cuff, the infraspinatus and teres minor adhere to the head of the humerus and aid in maintaining the humeral head in the glenoid cavity of the scapula. They cooperate with the posterior deltoid for adduction and external (lateral) rotation of the humerus.
According to Hughes RE and An KN (1996), during maximal contraction, Teres Minor can only cause very little scapular plane adduction, with an adductor moment arm of roughly 0.2 cm at 45° of shoulder internal rotation and approximately 0.1 cm at 45° of shoulder external rotation.
Origin
The lower portion of the lateral border of the scapula and the posterior side of the inferior angle are the sources of the teres major muscle. The muscle can be easily palpated at the inferior scapular angle, where it feels like a soft tissue structure.
Insertion
Teres Major Muscle inserted on the medial lip of the intertubercular groove on the humerus.
It is related to the latissimus dorsi muscle, which surrounds the bottom border of the teres major. The tendon of the latissimus dorsi and the tendon of the teres major are separated by a bursa.
Nerves Supply
The lower subscapular nerve, which derives from the C5, C6, and C7 nerve roots, innervates the teres major. This nerve arises from the brachial plexus; more precisely, it is the third branch of the posterior cord. It ends in the lower subscapular nerve after giving origin to the thoracodorsal nerve (C6, C7, C8 to the latissimus dorsi).
Along with innervating the teres major, the lower subscapular nerve also innervates the subscapularis as it flows inferiorly from the brachial plexus. The posterior cord splits into the axillary and radial nerves after producing the thoracodorsal nerve and lower subscapular nerve.
Blood Supply
The posterior circumflex humeral artery and the thoracodorsal branch of the subscapular artery supply the teres major.
The third distal segment of the axillary artery gives rise to the posterior humeral circumflex artery, which passes posteriorly via the quadrangular space and around the humeral neck. Through the quadrangular gap, the axillary nerve follows the posterior humeral circumflex artery. The teres major (superior), teres minor (inferior), long head of triceps brachii (medial), and surgical neck of the humerus (lateral) comprise the quadrangular space. The teres major, teres minor, deltoid, and long head of the triceps are supplied by the posterior humeral circumflex artery as it travels.
Lymphatics
The axillary artery nourishes the latissimus dorsi, intercostal muscles, and serratus anterior. It also gives rise to the subscapular artery, the biggest branch of its distal section. The circumflex scapular artery and the thoracodorsal artery are the two branches of the subscapular artery. This thoracodorsal artery crosses the lateral angle of the scapula as it flows anteromedially. This artery supplies the latissimus dorsi, serratus anterior, subscapularis, and teres major along its journey.
Embryology
It normally starts to develop in the upper limb between weeks four and five. In particular, the limb bud first emerges in week four, and migration—which results in the formation of the anterior and posterior condensations—occurs in week five. The latter results in the teres minor and teres major shoulder muscles. By eight weeks, all of the muscular groups in the upper extremities are established.
The paraxial mesoderm gives rise to the teres major, a muscle in the upper limb. The myotome is the result of this. There are further subpopulations within the myotome, and the primaxial myotome eventually gives rise to the teres major.
Actions
There are multiple shoulder actions carried out by the teres major. To put it another way, its main functions are to drag the arm towards the midline of the body, rotate it inward, and extend, medially rotate, and adduct the humerus.
Additionally, the teres major is crucial in maintaining the stability of the humeral head and preventing subluxation or partial dislocation. The latissimus dorsi muscle and the teres major frequently cooperate to perform these tasks.
Related Muscles
The teres minor, subscapularis, supraspinatus, and infraspinatus are the four muscles that make up the rotator cuff. One of the most important functions of the rotator cuff muscles is to stabilize the glenohumeral joint. Not regarded as a rotator cuff muscle, teres major nevertheless contributes to supporting the glenohumeral joint.
Anatomical Variations
Although they are uncommon, physiological variations of teres major have been documented, particularly at the insertion point. The tendon that joins the latissimus dorsi tendon at the medial lip of the humerus’s intertubercular groove is where the teres major enters. Variations in the proximal and distal locations of tendon fusion have been documented in the literature.
Since teres major is commonly employed in tendon transfer procedures for rotator cuff surgery, surgeons need to be aware of these variations.
Diagnosis of pronator teres muscle
A complete physical examination is necessary for the diagnosis of a pronator teres muscle ailment. Imaging tests and nerve conduction studies may also be performed. The following are typical steps for identifying a problem with the pronator teres muscle:
Physical examination
In addition to examining the afflicted area, a medical professional may inquire about the patient’s symptoms, including any tingling, discomfort, weakness, or numbness in the fingers, hand, or forearm.
In addition, they might evaluate the patient’s strength, feeling, and range of motion in the afflicted arm.
Imaging tests
A pronator teres muscle ailment may be diagnosed with the aid of an MRI, ultrasound, or X-ray.
These examinations can be used to detect any damage or irregularities in the surrounding structures, such as fractured bones or dislocated joints, or in the muscle itself.
Nerve conduction studies
If pronator teres syndrome is suspected, a nerve conduction study may be requested to evaluate the median nerve’s function.
To monitor the electrical activity of the nerves, tiny electrodes are applied to the skin during this test.
Surgical Considerations
The inferior border of the quadrangular space is made up of the teres major. The posterior humeral circumflex artery and the axillary nerve are located in this area. The teres minor forms this space’s superior border. Surgery is frequently necessary to repair tears to the teres minor. To prevent iatrogenic neurological or vascular damage, it is crucial for surgeons practicing in this field to be knowledgeable about anatomical structures.
Teres major is frequently employed in musculotendinous transfer for rotator cuff deficiencies, despite not being one of the four rotator cuff muscles. The axillary nerve, the radial nerve, and its branches may be in danger during this procedure. When transferring the latissimus dorsi and teres major tendons during rotator cuff repair, surgeons need to be on the lookout for these structures.
Rarely, isolated teres major tears happen when playing sports like baseball, tennis, swimming, and water skiing that require overhead motion. Regretfully, the literature outlining the handling of these cases is scant. Surgical surgery may be necessary in certain circumstances, however conservative care is typically the norm for teres major injuries.
Clinical significance
Isolated Teres Major Tears
Rarely, major tears can occur either acutely or over time. Patients frequently arrive with acute, sudden-onset pain in the axilla, shoulder, and proximal upper extremity. Physical exercise and any other activity that involves placing the hand posterior to the back aggravate the pain. In the inferior posterior axilla, ecchymosis and edema are common. During a physical examination, the teres major region may palpate with point pain. As a result of their injury, the patient may also exhibit weakness in the humerus’s internal rotation, adduction, and extension.
Combined Tears
It is possible to have separate or combination teres major injuries. In addition to the latissimus dorsi, the teres major is also impacted by combined tears. Because the tendons of these muscles converge near the lip of the humeral intertubercular groove, they are frequently damaged simultaneously. These combined tears happen similarly to single tears and are most common in young athletes, particularly pitchers of baseball.
Acute discomfort in the upper arm and posterior axilla, accompanied by soreness when palpated along the teres major and latissimus dorsi, are common presentations of the combined tear. Visual inspection often reveals mild asymmetry and ecchymosis. Magnetic resonance imaging (MRI) is the most effective imaging modality for evaluating the injury. To treat these combined tears nonoperatively, oral anti-inflammatories, physical therapy, and rest are frequently used. Most people can get back into their sport in a few months.
Teres Major Muscle Strain
Although they are uncommon, teres major strains can happen as a result of trauma or physical activity. One of the risk factors for a teres major strain is not warming up before exercise. This pathology has also been linked to motor vehicle accidents and falls onto the lateral border of the scapula.
A physical examination may reveal the jump sign, which is defined as an involuntary muscular withdrawal accompanied by passive internal rotation of the shoulder. Using a particular procedure to observe both shoulder girdles, broad field view magnetic resonance imaging can be used to further assess the amount of the strain and differentiate it from a tear. Since most of these injuries result in only modest consequences, the incidence of major injuries may be underreported.
Injury
Acute tears and chronic tears are two different kinds of rotator cuff injuries. A quick movement can result in acute tears. This may include hurling a strong pitch, grasping a swiftly moving rope while participating in water sports, tumbling into an extended hand quickly, or suddenly pushing with the paddle when kayaking. A persistent rip gradually becomes larger. They commonly happen when the tendon rubs against the underlying bone, which is at or close to the tendon. The teres minor usually returns to normal after a tear to the rotator cuff.
Imaging
Although rotator cuff tears frequently result in minor muscle atrophy, isolated teres minor atrophies have also been seen. Excessive and/or persistent compression of the structures passing through this anatomical tunnel is the result of quadrangular space syndrome. The gap is traversed by the posterior humeral circumflex artery and the axillary nerve. In abduction, extension, external rotation, and overhead exercise, the most common complaints from those afflicted are shoulder pain and paresthesia down the arm.
Compression of the appropriate axillary nerve branch or posterior humeral circumflex artery has been directly linked to selective atrophy of the teres minor muscle. Pathologically, dilated veins, lipomas, fibrous bands, and glenoid labrum cysts can all occupy the quadrilateral space. Thoracic outlet and inlet syndrome, anterior shoulder dislocation, humeral neck fracture, and brachial plexus damage are all associated with similar symptoms. To get the most comprehensive differential diagnosis feasible, those disorders must be included.
Ultrasonography is a useful diagnostic technique for teres minor fatty degenerative atrophy. Affected muscles exhibit increased echogenicity and perhaps a modest decrease in mass. Consolidating the diagnosis of neurogenic muscle atrophy is aided by MR imaging. Increased signal intensity on T2-weighted MRI sequences and normal signal intensity on T1-weighted sequences are indicative of extracellular edema following traumatic events leading to brain injury. A Doppler ultrasonography can be used to diagnose posterior humeral circumflex artery compression and decreased blood flow during stressed arm positions and/or maneuvers.
It is important to find the nerve next to the vessel. The posterior path of the axillary neurovascular bundle is evident in the neutral position, but in an elevated arm posture, it may be seen at the posterior axillary fold, right before it perforates the deltoideus. An MR angiography is necessary to evaluate the artery in great detail. The primary objective of an ultrasonography examination is to exclude any bulk that occupies space. To detect any decreased nerve conduction velocity and, thus, denervation of the affected muscle, further electromyography is useful.
Other Issues
Quadrangular Space Syndrome
The axillary nerve and posterior humeral circumflex artery are compressed as they pass through the quadrangular area in this uncommon ailment. Compression may result from either teres major fibrous bands or hypertrophy. It is linked to athletes who play sports like baseball pitchers, swimmers, and volleyball players that call for a lot of arm abduction and external rotation. Individuals frequently arrive with gradual onset shoulder pain, weakness, and loss of feeling in the axillary nerve innervated region. Furthermore, patients may have localized point soreness.
The upper quadrant of the body exhibits an imbalance in muscular strength, tension, and movement patterns, which is indicative of this illness. Many muscles of the front and posterior thorax are involved. Patients exhibit hunched over in their thoracic spine, lifted and extended shoulders, reduced spine mobility in the thoracic vertebrae, and forward head position.
There is a connection between these postural deviations and neck and back discomfort and inflammation. This is frequently brought on by those who read, watch television, or use computers for extended periods and maintain bad posture. Furthermore, upper-crossed syndrome may eventually result in dysfunction of the glenohumeral and cervicothoracic joints.
Physical Therapy
Injuries
Sports-related injuries fall onto the lateral scapula, and impact or strain injuries to the muscle sustained in motor accidents are associated with the development of teres major injuries.
Moreover, repetitive microtrauma from reaching up and behind (such as when taking a briefcase out of the back of a car, tossing something overhead, and other sports-related injuries) can result in myofascial pain in the teres major muscle.
Teres Severe injuries cause discomfort and make it difficult to perform tasks requiring the arm to move sideways or backward.
Although isolated teres’ major tears are rare, they can happen to pitchers and bowlers in baseball or cricket.
The main symptom of a teres major tear is acute pain that flares up in the shoulder, upper arm, and armpit. This usually happens when there is no treatment or rest for the muscle.
Usually, it hurts dull and gets worse when you move your hands behind your back, as in reaching into your pockets, playing tennis, pitching in a baseball game, or doing a downward freestyle stroke.
The affected muscle area may become inflamed, which could lead to swelling. The enlargement is perceptible when touched, even though it is not visible from the outside (at the bottom of the scapula).
The range of motion in the arm is limited in those who experience discomfort and pain in the upper arm.
A jump sign, or the involuntary withdrawal of the stimulated muscle, is another common indicator.
When exercises are performed without a suitable warm-up, Teres Major Strain frequently results.
In patients with upper crossed syndrome (UCS), the teres major is short and hyperactive; see the link.
One of the four rotator cuff muscles, the teres major, is implicated in several shoulder disorders, including quadrangular space syndrome
Assessment of Teres Major Muscle
Palpation
When the patient is in the prone position and their arm is not lying on the table, grasp the latissimus dorsi with your fingers and thumb.
Lay your fingers and thumb medially on the lateral edge of the scapula.
The teres major muscle fibers are situated medial to the latissimus and attach to the lateral margin of the scapula.
Track these fibers up to where they merge with the latissimus dorsi in the axilla.
Length Tension Testing / Stretching
When the patient is in the prone position and their arm is not lying on the table, grasp the latissimus dorsi with your fingers and thumb.
Lay your fingers and thumb medially on the lateral edge of the scapula.
The teres major muscle fibers are situated medial to the latissimus and attach to the lateral margin of the scapula.
Track these fibers up to where they merge with the latissimus dorsi in the axilla.
Treatment of pronator teres muscle
Rest
It’s critical to give the injured armrest so that the muscle can repair.
It is advised to stay away from activities that make the injury worse, such as hard lifting or repetitive motions.
Ice
Reducing pain and inflammation in the wounded area may be achieved by applying an ice pack.
Applying ice for 20 to 30 minutes every few hours is possible if necessary.
Compression
Compression sleeves or bandages can support the affected muscle and help with edema reduction.
Medications
It can be suggested to use over-the-counter painkillers, including ibuprofen or acetaminophen, to assist control of discomfort and inflammation.
Exercise of Teres Major Muscle
Stretching exercise of Teres Major Muscle
Teres major stretch
You can perform this stretch in a seated or standing position. Raise your right arm high above you.
Next, bend your right elbow so that your right hand’s palm reaches down your back, aiming between your scapulae.
Put the left hand on the elbow of the right.
You can now gently help the right elbow to go toward the left.
Try not to let your head droop forward and keep your chest raised. To maintain firmness on the back, also point the scapulae in the direction of the tail.
With this gentle movement, you might feel a stretch if your teres muscles are extremely tight.
You might begin to incline your upper body to the left to intensify the stretch.
Retain the scapulae firmly in place and the pelvis level. Refrain from collapsing to the left.
After five to eight seconds, go to the left.
External Rotation Stretch
Place yourself on a level bench and stretch your right upper arm at your side, away from your shoulder.
Your forearm points away from your feet as your elbow bends to a ninety-degree angle.
With help, firmly grasp your elbow with one hand while using the other to press your wrist downward.
Hold this pose for 15 to 30 seconds, or until you feel a slight stretch. Then, switch to your left arm.
Overhead Shoulder Flexion
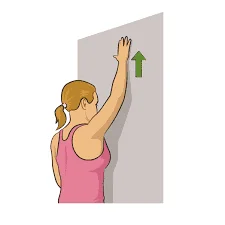
Step inside a door frame and take a position.
Raise both arms over your head and place your palms on the wall, slightly above the frame, shoulder-width apart.
Move your head and upper torso in front of your hands while you slant slightly forward.
Ten seconds after you feel a slight stretch, hold it. Do it two or three times.
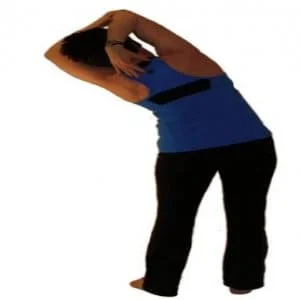
Side Bends

Spread your feet wider than your shoulders and take a tall stance.
Point the toes of your right foot sideways and rotate it outward by ninety degrees.
Lean to the right and rest your right hand on your knee while extending your left arm above your head.
When you feel strain in your upper body’s left side, stop and hold the position for 20 to 30 seconds.
Stretch again in the opposite way.
Keep your thighs and chest pointed forward while performing the exercise.
Standing Hands Clasped Over Head

Maintain a straight posture and place your feet hip-width apart. With your hands toward the roof, clench them together and place them over your head. Lower your pelvis and your tailbone straight down to the floor.
Your shoulders and chest are bare.
Similar to a tripod, feel the tips of your feet. Touch the ground with the balls of your heels, big toes, and small toes.
Inhale, raise your elbows straight up and extend your hands toward the ceiling.
Bending the side will increase the stretch’s intensity.
Crossing your hands at the waist will help you feel more extended.
Strengthening Exercise of Teres Major Muscle
Single-Arm Dumbell Row

Select a level bench, place your right knee and right hand beneath your shoulder on the bench, and take a dumbbell in your left hand.
Keep the dumbbell positioned just beneath your left shoulder.
Bend at the elbow and start lifting the dumbbell higher. It’s crucial to keep your arm close to your body and raise it until it nearly reaches your hip.
Lower yourself to the starting position.
Once you reach the appropriate number of repetitions, repeat this movement.
Finish the five to ten repetitions.
One set at a time, repeat.
Chin Ups
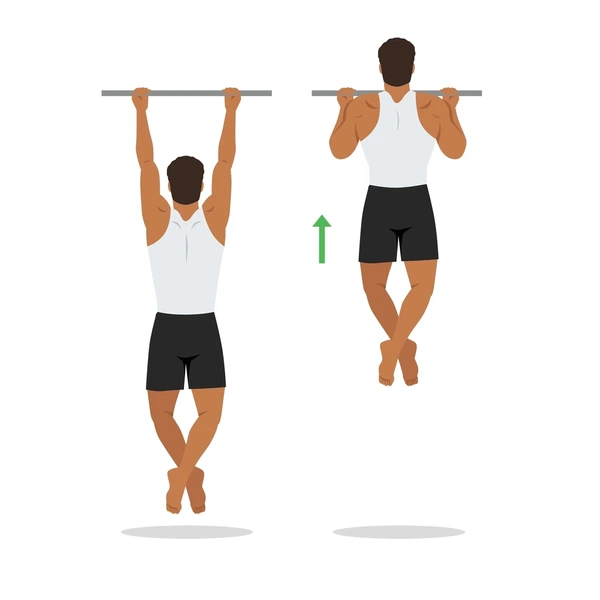
With your hands shoulder-width apart, take an underhand grip on the bar.
Pull yourself up to the bar as high as you can while keeping your arms perfectly straight, preferably bringing your chest as near to the bar as you can.
At the top, pause for a few moments before stepping back down to the beginning.
Finish the five to ten repetitions.
One set at a time, repeat.
High Cable Reverse CrossoverFly
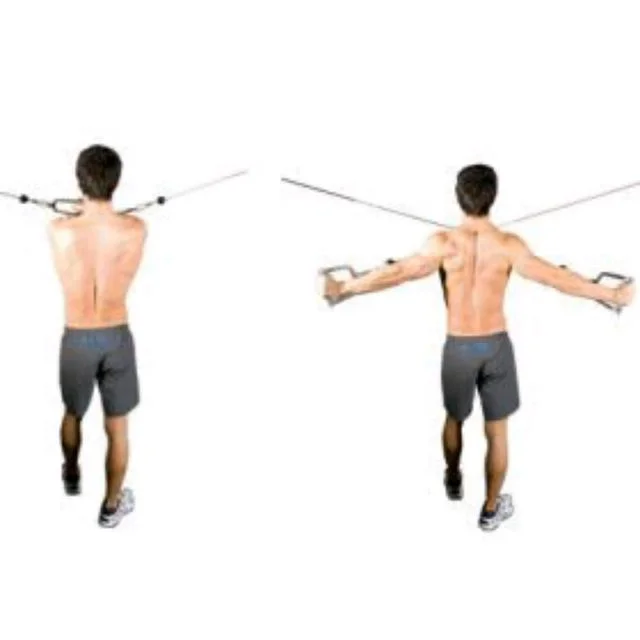
Place yourself in front of the machine with two pulleys at head height.
To align your arms with your back, take hold of the handles with an overhand grip and start lowering your elbows as far back as you can.
With steadiness and control, start to go back to your starting position.
Finish the five to ten repetitions. One set at a time, repeat.
Seated Cable Rows
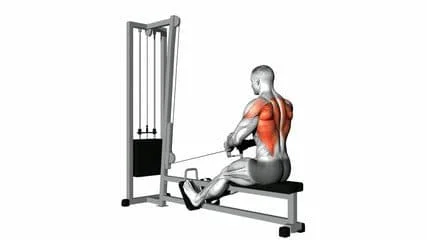
- With your feet flat on the ground, take a straight seat on the bench.
- Keeping your elbows by your sides, extend your arms, grasp the cable’s grip, and pull downward.
- To get back to your starting posture, slowly extend your arms.
- Manage your repetitions of this action until you reach the appropriate quantity.
Dumbbell Pullover
- Just your neck and upper back should rest on a bench.
- Using both hands, hold the dumbbell at the desired weight so that your hands create a triangle.
- Hold the dumbbells over your chest with your elbows slightly bent to avoid hyperextension.
- As you controllably lower the dumbbell as far over your head as you can, contract your core muscles.
- Start raising the dumbbell back to its initial position.
Concussion
A blow to the head or body that causes the brain to tremble inside the skull is known as a concussion, one kind of traumatic brain injury. This shaking may cause brief brain activity alterations, resulting in headaches, dizziness, disorientation, and memory loss.
Your query doesn’t make it apparent whether there is a particular link between concussions and the teres major muscle. To receive the appropriate diagnosis and treatment for a possible injury involving both a concussion and the tear’s major muscle, it’s critical to seek medical assistance. The most qualified person to evaluate and handle any problems with these matters would be a healthcare professional, such as a physician or physiotherapist.
FAQ
Why is it called teres major?
Positioned above the latissimus dorsi muscle, the teres major muscle (derived from the Latin teres, meaning “rounded”) aids in the extension and medial rotation of the humerus.
What is the main function of the teres major muscle?
The teres major’s primary job is to move the humerus at the glenohumeral joint. Specifically, it drags the humerus’ anterior surface medially in the direction of the trunk or internally rotates it. It also can extend the arm from a flexed position.
How do I relax my teres major?
Lay your upper arm over the side of the seat, just behind your ear and over your head. Make sure your palm is facing away from the bed and let your arm dangle down. A stretch will be felt directly behind your armpit. Roll your upper shoulder forward toward the bed’s surface to lengthen the stretch.
What causes teres major pain?
A typical reason is overuse or stress on a muscle. The following are some causes particular to this muscle: hefty steering wheel maneuvering. both forward and overhead reaching, particularly while moving heavy objects, as when cutting wood. sleeping for extended periods with the arm medially rotated.
What is another name for Tere’s major muscle?
The lateral edge of the scapula is accompanied by a little muscle known as the teres major (TM). It is often called “lat’s little helper” because of its complimentary function with the latissimus dorsi.
Is Tere major a parallel muscle?
The latissimus dorsi and infraspinatus muscles that border the teres major run parallel to the teres major muscle fibers. The teres major muscle in the arm attaches medially to the latissimus dorsi muscle’s insertion, within the intertubercular sulcus on the anterior aspect of the humerus.
Is the teres major abduction or adduction?
The teres major is a fusiform muscle that provides internal rotation, extension, and adduction of the shoulder. The subscapularis muscle is responsible for the internal rotation of the humerus; its upper part affects abduction and its lower part affects adduction.
What is the difference between lats and teres major?
On the rear of the torso is a big, strong muscle called the latissimus dorsi. Because teres major is a tiny muscle whose primary function is to help latissimus in certain of its functions, it is frequently mentioned in conjunction with latissimus.
Is Tere major a back muscle?
The lateral edge of the scapula is accompanied by a little muscle known as the teres major (TM). It is one of the seven scapulohumeral muscles that help to improve shoulder motion by encircling the glenohumeral joint.
What is the teres major connected to?
comes from the inferior angle of the scapula’s posterior surface. It affixes to the humerus’s medial lip of the intertubercular groove.
What is the difference between teres minor and a major?
The quadrangular space is located beneath the shoulder joint, and the margins of the axilla’s two intermuscular spaces make up the teres minor muscle. Its superior border is made up of teres minor, while its inferior border is bounded by teres major, the humeral shaft laterally, and the long head of the triceps medially.
Is teres major tough?
Meat from highly active animals is typically harder. But because the teres major is located just below the leg of the cow, it keeps its melting texture and all the culinary benefits of the leg. Handle this cut with extreme caution. After seasoning it with salt and pepper, roast or grill it whole to your preferred doneness (we like medium rare).
What exercise targets the teres minor?
To sum up, the teres minor muscle plays a crucial role in maintaining the stability and mobility of the shoulder. Exercises like external rotations, stipulation, face pulls, reverse flys, and YTWLs that target this muscle can help you strengthen and enhance the health of your shoulder.
Why does my teres major hurt?
A typical reason is overuse or stress on a muscle. The following are some causes particular to this muscle: hefty steering wheel maneuvering. both forward and overhead reaching, particularly while moving heavy objects, as when cutting wood. sleeping for extended periods with the arm medially rotated.
How to self-message teres major?
It is okay to go a little overboard in this case. Rather, I suggest utilizing a massage ball. Turn your afflicted side toward the wall. To get onto the teres major, position the ball on the wall and press with the side of your body, at the level of your armpit.



One Comment