Trigger Points in Lower Back
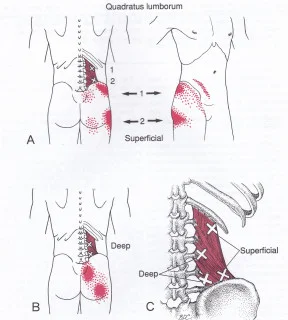
Trigger points in the lower back are tight, sensitive areas within muscle fibers that can lead to pain, stiffness, and restricted movement. These points often develop in muscles like the quadratus lumborum, erector spinae, and gluteal muscles due to factors such as poor posture, overuse, or stress. A trigger point is what? A trigger point…








