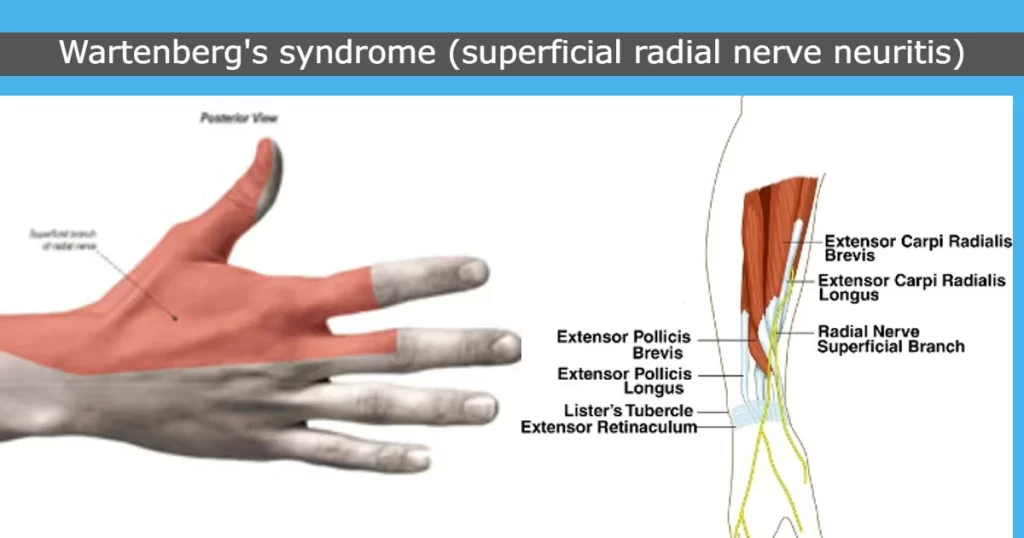
Cheiralgia Paresthetica also called Wartenberg Syndrome) is a condition that occurs mostly due to the compression or entrapment of the superficial branch of the radial nerve. This nerve, responsible for sensory functions in the back of the hand and thumb, can cause numbness, tingling, and pain on the radial (thumb) side of the wrist when compressed.
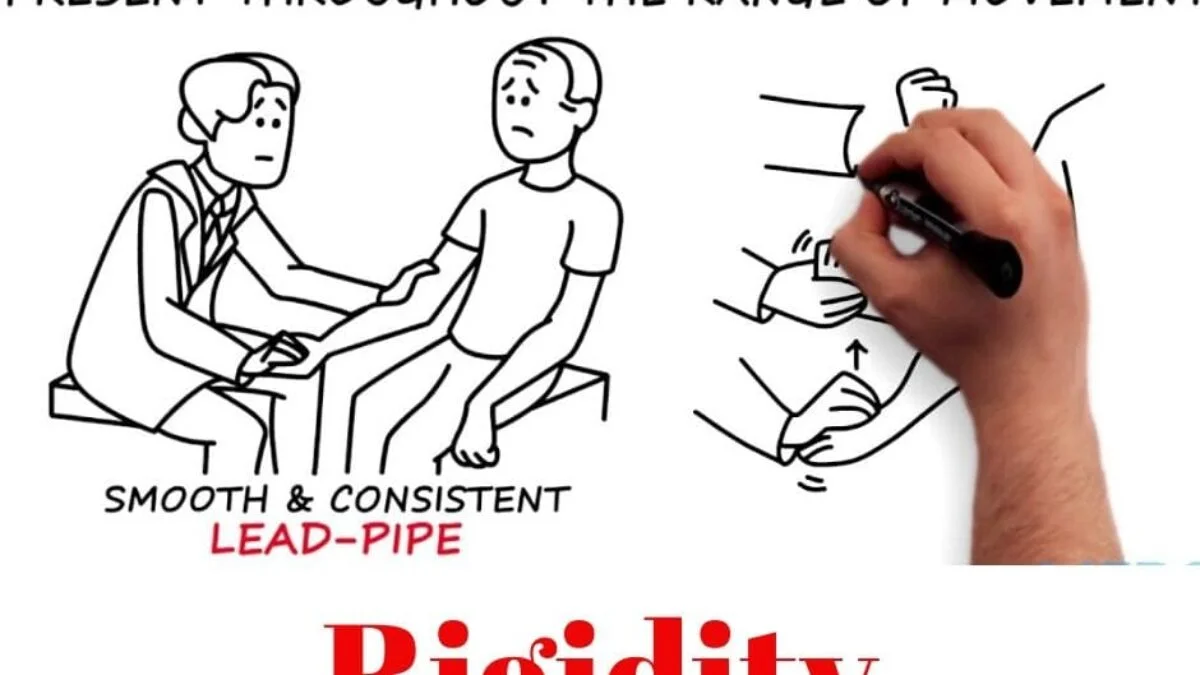
Warternberg syndrome, another name for Cheiralgia Paresthetica, is a compressive neuropathy. because of compression caused by the extensor carpi radialis longus (ECRL) and brachioradialis movements during forearm rotation, such as when turning a key. The disease comes and goes, causing prolonged periods of time possibly years without any complaints, occasionally broken up by one or more consecutive bouts. It’s regarded as a harmless disorder. Conservative therapies include rest, wrist splints, and, in certain situations, CSIs with surgical decompression.
Rarely, the incidence was less than 1 per 100,000 per year. The male-to-female ratio is 1:4, and women between the ages of 20 and 70 are thought to be more likely to have it.
Compression of the superficial branch of the radial nerve at the location where the nerve emerges from underneath the muscles results in Cheiralgia Paresthetica. Entrapment of the superficial branch of the radial nerve occurs at the lateral boundary between the brachioradialis and extensor carpi radialis longus muscles. The brachioradialis muscles rotate the nerve while closing the gap between these two muscle tendons in a scissor-like manner, causing entrapment when the forearm is repeatedly pronated. Forced pronation and wrist ulnar deviation exacerbate the pain.
Anatomy
Anatomy of the superficial radial nerve:
The radial nerve splits in the proximal forearm, and the superficial sensory branch of the radial nerve emerges between the brachioradialis and extensor carpi radialis longus (ECRL) to become superficial after traveling deep to the brachioradialis in the forearm muscle’s undersurface, about 9 cm proximal to the radial styloid.
The subcutaneous tissues still include the superficial radial nerve (SRN). It is in charge of transporting afferent sensory information from the dorsum of the thumb, index, and middle fingers proximal to the proximal interphalangeal joints. It also provides branches to dorsal digital nerves.
Branches:
The distance between the dorsal branch and Lister’s tubercle is 1-3 cm. It provides the first and second web spaces.
The palmar branch nourishes the dorsolateral thumb and crosses the extensor pollicis longus within 2 cm of the first dorsal region.
Roots of the radial nerves: T1, C5, C6, C7, and C8.
Pathophysiology:
Though the posterior border of the brachioradialis poses the greatest risk, the SRN can become stuck anywhere along its entire journey in the forearm. Trauma is also a common cause of superficial radial nerve compression, which can be caused by strain injuries to the nerve (e.g., closed reduction of a forearm fracture) or direct pressure on the nerve (e.g., by a bracelet or handcuff).
Wartenberg’s symptoms and nerve injury are related to the force exerted on the nerve and the duration of its compression.
Because of the compressive damage to the nerve’s myelin coating, microvasculature, or nerve itself.
Axonal damage and ischemia may ensue from severe compression that obstructs blood flow.
Additionally, the length of compression has an alternative effect on the nerve: 1) Temporary reductions in blood flow may result from intermittent compression. 2) Prolonged compression causes blood flow to decline over time.
Demyelination, inflammation, scarring, fibrosis, and ultimately axonal degeneration can result from these long-term alterations. For a greater chance of healing, it must be removed before significant nerve damage has occurred. Recovery from nerve remyelination may take many weeks. Axonal regeneration is quite sluggish, though.
Cause of Cheiralgia Paresthetica:
Anywhere throughout its whole length, the radial nerve is squeezed. The nerve above the lateral wrist area may be compressed by tight handcuffs and wristwatches. Additionally, distal radius fracture pieces of soft tissue tumors (such as ganglion cysts or lipomas) might crush it. Iatrogenic injuries sustained during wrist arthroscopy surgery, external fixation implantation, internal fixation of distal radius fractures, and initial dorsal compartment release can also result in nerve damage.
Comparable techniques include radial arterial line removal, cannulation, cephalic venipuncture, and acupuncture. For de Quervain’s tenosynovitis, steroid injections are administered into the tendon sheath; however, this might harm the nerve itself by causing subcutaneous atrophy.
These two tendons run parallel to one another during forearm supination action, preventing compression of the nerve. However, the extensor carpi radialis longus compresses the nerve by crossing the brachioradialis muscle during pronation action.
Wartenberg’s syndrome also develops when diabetes mellitus is present in the body. In 20–50% of cases, this syndrome is also linked to De Quervain’s disease.
Signs and Symptoms of Cheiralgia Paresthetica:
Both the dorsomedial hand and the proximal forearm are experiencing burning agony.
Repetitive wrist flexion and ulnar deviation movements also aggravate the symptoms.
Signs:
This usually happens when the intrinsic hand muscles weaken the ulnar nerve supply, namely the denervation of the nerve that supplies the palmar interosseus muscle to the little finger.
Repeated wrist flexion, ulnar deviation, and pronation movement are tested provocatively.
Differential Diagnosis:
Although the pattern of symptoms may change due to anatomical variances, patients with SRN compression experience pain or dysesthesias on the dorsal radial forearm as well as pain spreading to the thumb and index finger.
Alternative diagnoses, such as a more proximal lesion or a tumor in the radial tunnel that affects both the PIN and SRN, may be considered by the doctor if the sensory problems occur concurrently with a weakening of the muscles that are supplied by the PIN. SRN entrapment symptoms might be mistaken for de Quervain’s tenosynovitis symptoms, such as wrist pain and ulnar deviation, as compression of the SRN frequently takes place in the first dorsal compartment region. The primary sign is whether or not there is SRN compression.
De Quervain’s tenosynovitis:
Unlike Wartenberg Syndrome, wrist pronation movement does not exacerbate pain in this disease.
Dorsoradial forearm edema might be the result of this. Exacerbation and “wet leather” crepitus during repetitive wrist flexion or extension movements are the symptoms.
Arthritis of the thumb carpometacarpal joint.
Diagnosis
Physical examination:
provocative tests.
Finkelstein test: The patient is instructed by the therapist to perform an ulnar deviation movement, which is a wrist movement that is upward, and to make a fist around the thumb. 96% of individuals had worsened symptoms according to this test.
There are exterior compressions, scars, and masses.
Skin changes.
Sensation:
Light touch: This might not be typical.
Two points Discrimination: In 80% of patients, this can be abnormal. 256 Hz vibration: This might be unusual.
Muscle Strength: There are no symptoms of atrophy or motor weakness. Perhaps there is less grip strength.
Special test:
Hoffman Test: Determine the upper motor neuron dysfunction with the Hoffman Test.
Dellon Test: Active, forceful forearm hyperpronation, wrist flexion, and ulnar deviation with the elbow out to the side.
Wartenburg’s Compression Test for Neuritis.
The Radial Nerve Compression Test’s Superficial Branch.
Optional Nerve Block Examination:
The superficial branch of the radial nerve is blocked by local anesthesia:
The Finkelstein Test might turn out to be negative.
Measured grip and pinch strength might be enhanced.
Imaging Examinations:
Radiography:
If the radial nerve becomes trapped in the arm, a radiographic examination should be done to look for any tumors, healed calluses, or fractures. Radiological studies provide proof for any ailment, including cancers, arthrosis, dislocations or instabilities, elbow or forearm fractures, and posterior interosseous nerve dysfunction.
Nerve Conduction Study:
It is employed to measure the affected nerve’s electrical activity and contrast it with typical levels. It could be able to determine the location and kind of nerve damage in an inaccurate manner.
Ultrasonography:
It assists in determining the many reasons for wrist pain, such as de Quervain tenosynovitis, thumb joint arthritis, and cheiralgia paresthetica. It can also be used to locate locations where nerves are compressed or trapped.
Plain Radiographs:
They aid in locating any orthopedic disorders or bony prominences.
Magnetic Resonance Imaging:
Any constriction or expansion of the bony portion can be seen in T1-weighted pictures. Fat-suppressed density-weighted T2-weighted imaging can detect alterations in the nerve itself, such as augmentation and edema. Checking for aneurysms, ganglions, and lipomas is also beneficial.
Electromyography:
EMG aids in identifying the damaged region and tracking the time it takes for the nerves to heal. Three to six weeks following the injury, the EMG was negative. Nerve healing should be evident four months after the injury.
The abductor pollicis longus, extensor pollicis longus and brevis, and extensors indicis muscles will all exhibit abnormal function if just the lateral branch is squeezed. A localized compression site has normal function if the proximal portion is compressed, and abnormal function if the distal portion is compressed.
Treatment of Cheiralgia Paresthetica:
Medical Treatment:
Conservative Management:
The primary treatment for this illness is conservative. Removing the tight item, like a bracelet or wristwatch, is a crucial part of nonsurgical treatment if external compression is the frequent underlying cause.
Splinting,
rest,
Modification of nonsteroidal anti-inflammatory medication action.
In this disease, more individuals who receive nonoperative treatment have satisfactory to exceptional results.
Surgical management:
Surgical Decompression:
Between the brachioradialis and extensor carpi radialis longus, neurolysis and fascia band release occur:
Procedure:
To join the two muscles, draw a line. Determine the region of entrapment. Between the brachioradialis, which is located above, and the extensor carpi radialis longus, which is located below, the superficial branch of the radial nerve typically emerges.
A variety of adhesive barriers can be used to completely decompress the nerve. The barrier is cut to precisely fit the measured region of nerve compression. One might use the soft sterile dressing and continue with the multilayer closure.
Early range of motion should require postoperative care. Following surgery, physical rehabilitation should begin two weeks later. In order to lessen the creation of adhesions, desensitization, and scar massage around the scar region, it should support the early range of motion protocol and nerve gliding procedures. Following surgery, patients get treatment for four to six weeks and reach their full medical improvement sixty to ninety days later.
Physical therapy Treatment
PNS, or peripheral nerve stimulation, is used to lessen pain.
applied to the pain location via TENS or nerve stimulation.
Once a day, apply this stimulation for ten minutes.
Pulsed low-intensity infrared laser.
Splint:
suggested that the patient wear a wrist splint to prevent jerky movements and to support their hand.
Electrical stimulation:
Determine the muscle’s precise motor point first.
given a galvanic current initially, followed by a gradually faradic current.
Mobility exercise:
Less repetition is required for wrist ulnar and radial deviation as well as forearm pronation movement in this situation because the movement is limited or uncomfortable.
The therapist encourages clients to sit comfortably in a chair with support for their forearms, create a fist, and twist their forearms back and forth. Do it five or seven times, then progressively more.
The patient should next be instructed to do the wrist deviation action. Do it five or seven times, then progressively more.
Perform this exercise without experiencing any pain.
Complications of Cheiralgia Paresthetica:
Decompression surgery was unsuccessful.
Chronic numbness and pain
Dehiscence of wounds
Infection
Symptoms becoming worse
damage to the suture’s surrounding tissue.
Prognosis
Cheiralgia paresthetica treatment results are encouraging. Patients frequently experience a spontaneous remission of their symptoms. According to estimates, up to 71% of patients who have nonoperative treatment experience satisfactory to exceptional results.
There have been conflicting findings on the effectiveness of surgical care following nonoperative therapeutic failure. While Calfee et al. report relatively moderate outcomes, with 55% of patients treated operatively still experiencing symptoms at a follow-up of 3.5 years, Lanzetta and Foucher observed a 74% success rate with surgical intervention.
According to Gaspar et al., a number of individuals who have basic nerve decompression treatment do not experience consistent outcomes. Compared to other peripheral neurolysis procedures, neurolysis for entrapment of the superficial branch of the radial nerve has worse results and higher recurrence rates.
FAQs
What is the radial nerve Wallenberg syndrome?
A particular mononeuropathy known as Wartenberg’s syndrome is caused by entrapment of the radial nerve’s superficial branch. Numbness, tingling, and weakness in the thumb’s back are among the symptoms. Cheiralgia paresthetica is another name for it.
In ENT, what is Wartenberg syndrome?
The most prevalent kind of autosomal dominant syndromic hearing loss is Waardenburg syndrome. It includes pigmentary anomalies of the skin, hair (white forelock), and eyes (heterochromia iridis) as well as sensorineural hearing loss.
For Wartenberg syndrome, what kind of splint is used?
At the initial post-operative visit, patients will be put in a detachable thumb spica splint. After two to three weeks of wearing this splint, patients will start treatment. Patients might anticipate returning to their regular activities in 4-6 weeks after therapy, which typically lasts 2-3 weeks.
What is Wartenberg syndrome known by another name?
“cheiralgia paraesthetica” is another name for it. because of compression caused by the extensor carpi radialis longus (ECRL) and brachioradialis relative motion during forearm rotation.
What distinguishes radial tunnel syndrome from Wartenberg syndrome?
Wartenberg’s syndrome, the most well-known kind of SRN compression, manifests as a painful feeling in the SRN-innervated area. The areas impacted and the compressed position of the radial nerve distinguish RTS from Wartenberg’s syndrome.
Wartenberg’s Syndrome: What causes it?
Wartenberg’s syndrome can have several causes, such as: having a fractured forearm and wearing a tight cast. wearing handcuffs, watches, or tight wristbands. suffering from a slight wrist injury.
Why does Wartenberg occur?
The brachioradialis and extensor carpi radialis tendons compress the superficial radial nerve in this situation, particularly when the forearm is pronating. Perform this exercise without experiencing any pain.
Wartenberg’s migrating sensory neuropathy: what is it?
Frequent bouts of scorching pain and loss of feeling in the distribution of one cutaneous nerve at a time are hallmarks of Wartenberg’s migrating sensory neuropathy. The skin of the face, chest, and limbs are frequently affected.
A good Wartenberg sign is what?
The observation of the fifth digit abduction movement and the incapacity to adduct the fifth finger while extended are good indicators of Wartenberg’s syndrome.
Cheiralgia: What is it?
It shows up as sensory abnormalities in the dorsal and radial parts of the hand and wrist, including paresthesias. Another name for it is Wartenberg’s syndrome.
References
Physiotherapist, N. P.-. (2023e, December 13). Cheiralgia Paresthetica (Warternberg syndrome): Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/cheiralgia-paresthetica-warternberg-syndrome/
Wikipedia contributors. (2023, August 25). Wartenberg’s syndrome. Wikipedia. https://en.wikipedia.org/wiki/Wartenberg%27s_syndrome
Anthony, J. H., Hadeed, A., & Hoffler, C. E. (2023, June 5). Cheiralgia Paresthetica. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK545200/
These can vary based on your objectives or the level of fitness you wish to achieve. For example, exercises done on a yoga mat are not the same as exercises done with weights.
Mat exercises are a good place for beginners to start because they usually don’t demand a lot of strength or flexibility. You can also select the sets and repetitions that work best for you, based on your physical capabilities. In a similar vein, poses and workouts done on a yoga mat can be customized to fit the needs and preferences of each individual.
Mat activities are given to:
Encourage equilibrium
Promote stability
Activate and fortify the limbs and back.
Prepare for tasks that require function.
To get the intended outcome of the treatment program, mat exercises should be arranged in an easier-to-difficult order, and progression through the sequence should be taken into consideration. Based on the patient’s condition and degree of strength, the therapist selects the type of mat exercises that the patient will perform.
How much of an activity can be completed and how long it takes to learn depends on the patient’s abilities. It is imperative that therapists work hard to improve their patients’ agility and timing.
Benefits of Mat Exercises
There are certain general advantages to utilizing the mat for core exercises, even though the advantages of the various mat routines we mentioned above vary. Among them are:
Build up your core, gluteal, shoulder, and back muscles.
Improve stability and flexibility
alleviate neck and back pain
Boost your muscles’ strength and burn calories.
Reduce tension and worry
Here are some examples of various mat exercises for full-body training:
To improve your outcomes, you might select five to seven exercises from this list and execute them for thirty minutes at a time.
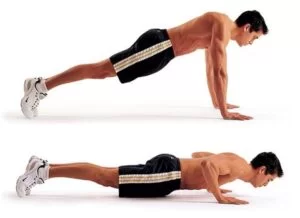
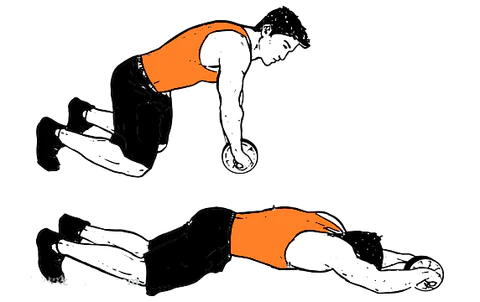
Plank
plank
If you keep proper form, planks are an excellent technique for working out your complete body in one workout. An activity mat provides enough cushioning to be comfortable on all four limbs. You might do a plank on your palms or your forearms. A variety of wrist wraps are available to support joints.
Begin by establishing a plank posture with your forearms and toes on the floor, facing down. Your head is relaxed even though you should be looking at the floor.
Maintain a firm and upright trunk and a straight body from your ears to your toes without bending or sagging. The spine should be positioned like this. Verify that your shoulders are relaxed and not tucked in toward your ears.
Hold this stance for ten seconds. Let go to the ground.
Bridges
bridge
This mat exercise requires you to bend your back into a bridge, as the name would imply. If you’re looking for some abdominal exercises, we suggest trying this one.
If you have a mat, place it in an open spot on the floor and lie on your back.
To tighten your abs and buttocks, press your lower back on the floor.
Your belly button will come closer to your spine if you flex your abdominal muscles.
Lean your hips back to return to the beginning posture.
Crunches
Crunches-exercise
It tones the rectus abdominis, which is the muscle that makes up your abs, as well as the muscles in your back. However, to make it more comfortable, you may also perform it on a yoga or fitness mat.
Put yourself on your back. Ensure that your feet are hip-width apart. Tense your abdominal muscles as you take a breath.
With your head and neck comfortably in place, exhale and raise your upper body.
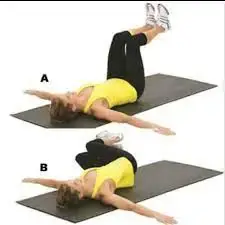
Leg Raises
Straight-leg-raise-
By strengthening and stabilizing the affected area, leg lifts while lying down can also alleviate lower back discomfort.
You must lie down in a supine position with your arms by your sides to begin this workout.
Now spread your legs apart.
Exhale and lift your legs.
Hold this position for 5–10 seconds.
You will breathe in and control your legs as you descend, keeping your lower back in contact with the floor. Keep your feet floating off the ground as you descend from the exercise, and then perform the previous three steps ten times.
Superman
Superman Exercise
Face down on the floor, position your arms aloft, palms facing each other, legs straight, toes touching the floor, and pinkies lying on the ground.
Maintain a neutral neck position and focus on your eyes while using your back, core, and glutes.
After a two-second pause at the peak, carefully drop your arms and legs to begin again.
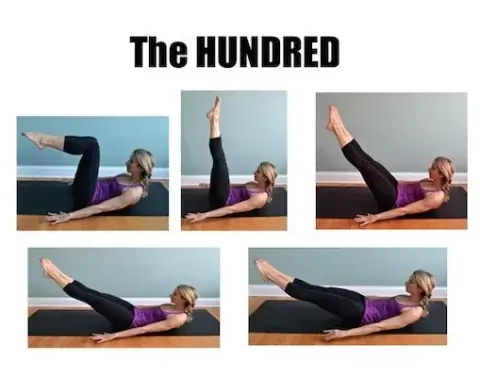
Pilates 100s
Pilates-hundred
If there are no Pilates mat exercises included in the mat workout, it is not complete. Thus, this is the final move that novices are frequently advised to make.
The exercise gets its name from the fact that you have to do 100 arm muscle beats while extending your legs and lifting your head and shoulders off the mat. You may also use the hundred as a high-intensity warm-up before doing core and lunge exercises.
Take up a prone posture. Assume the tabletop posture by raising your legs and bending them at the knee while keeping your shins and ankles parallel to the floor.
Inhale.
Take a breath and release it. Raise your chin and head to shoulder blade level, then utilize your abdominal muscles to lift your upper back off the ground. Maintain an engaged back and downward-flexed shoulders. Peer down into the scoop of your abs. Hold on while you inhale.
Take a breath and release it. Draw your abs deeper while simultaneously extending your arms and legs. For more complicated operations, you can raise them higher or lower as needed. Make sure you only lower your legs to the extent that it doesn’t cause you to tremble or cause your lower back to rise off the mat. Arms should be straight and lowered so that your fingertips are only a few inches off the ground and pointed towards the far wall.
Maintain your position. Inhale five brief breaths, followed by five short exhalations. During this workout, pump your arms up and down a little yet quickly. Keep your neck and shoulders relaxed. The strongest muscles should be found in the abdomen.
Ten full breath cycles should be performed. Every cycle consists of five quick inhalations and five quick exhalations. The arms pump up and down in a 6- to 8-inch pump in sync with your breathing. Maintain a flat back, a scooped abs, and a head pointed down to stretch your spine. Breathing deeply is important. Breathe deeply into your back and sides. Practice your lateral breathing if you’re not familiar with it.
Finally, keep your spine curved while raising your knees to your chest. Breathe in deeply, then out.
Seated Russian Twist
seated-twist
A wonderful approach to improving your shoulder and core muscles is to perform Russian twists while seated. Even though it can be used as a beginner’s yoga mat practice, the workout is not that simple.
You’ll need a lot of help and strength to accomplish it.
Next, lean backward such that your upper body is angled 45 degrees in the direction of the floor. Throughout this exercise, it will be easy to hunch your shoulders forward but fight the impulse to keep your back straight. Join your hands in front of your chest while bracing your core. Move your arms singly, then the other way around. That is equivalent to one rep.
Mountain Climber
mountain-climber
You’ll look like you’re running against the ground. Once you get the hang of this move, you can try mountain climber versions.
When you initially start, try the classic variation of the exercise:
Hold a plank position, evenly distributing your weight between your hands and feet. Aim for a flat back, align your head, and place your hands shoulder-width apart.
As near to your chest as you can, try to bring your right knee.
Pull one knee out and bring the other in to do a leg switch.
Keep your hips down and move your knees in and out as quickly as widely as possible. Breathe in and out alternately with each leg shift.
Cat-Cow
Cat-and-Cow-Stretching
For people who are sedentary at work, this is the ideal workout.
Begin with both hands and the knees, knees beneath your thighs, hands under your shoulders, or slightly forward.
Press through the base and fingertips of your fingers as you extend them.
In a cat stance, exhale, draw in your belly, raise your side waists, turn your back, and lower your head to the floor.
When you forcefully push the floor away, feel the stretch in your back.
Exhale and return to your initial neutral stance by taking a step.
Following multiple repetitions of the Cat-Cow pose, the Cow stance is frequently utilized to warm up the spine.
Downward Dog
Downward-Facing-Dog-Pose-Adho-Mukha-Svanasana
Your entire body is stretched during the activity, improving your flexibility and balance.
You can practice this pose anywhere there is a yoga mat available.
Squeeze your fingertips to your forearms after spreading your fingers.
Rotate your upper arms outward to make your collarbones larger.
Allow your head to drop loosely as you move your shoulders from your ears to your hips.
Firmly contract your quads to take the weight off your arms. This movement designates this as a resting stance.
Turn your thighs inside, keep your tail up, and press your heels down toward the earth.
Make sure your hands and feet are at the proper distance apart by bringing yourself forward into a plank position. The distance between the hands and the feet in each of these stances should be the same. Refrain from stepping the feet toward the hands in Down Dog to bring the heels to the floor.
Double-Leg Stretch
If you find this exercise too challenging, try working on one leg at a time. An alternative would be to fully extend the legs while bending the knees slightly.
To lengthen your lower back, bring both knees to your chest while holding onto your ankles.
Make a middle drawing.
Breathe out and raise your legs and arms to the sky, staying in the same position as shown.
Hold the stance for ten long, deep breaths, and then release.
Do this ten times over.
Single-Leg Circles
Your core strength and pelvic stability are tested with the single-leg circle. In addition, it strengthens the quadriceps and hamstrings and promotes a healthy hip joint. If you can’t raise the leg straight up towards the roof, just stretch it as far as you can.
Raise and extend your right leg.
Extend your left leg from beneath you.
If possible, grip the toes with both hands. Should you be unable to maintain your balance on your toes, grasp onto your thigh or calf, and raise your heel to the ceiling?
Hold this position for ten counts.
Spread your arms and hands to your sides after releasing your grip.
With your leg outstretched, make ten little circles in each direction.
Proceed to the other side.
Hip-Opening Exercise
frog-jump
The frog is a hip-opening exercise that you can do while seated or reclined. Either way, hip openers help your hips and spine stay flexible and in balance.
As far apart as seems comfortable, extend your knees.
As you rest, take slow breaths and keep your knees apart.
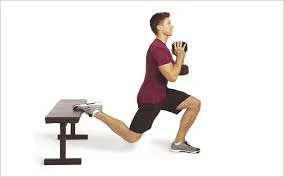
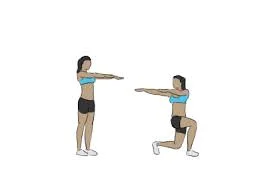
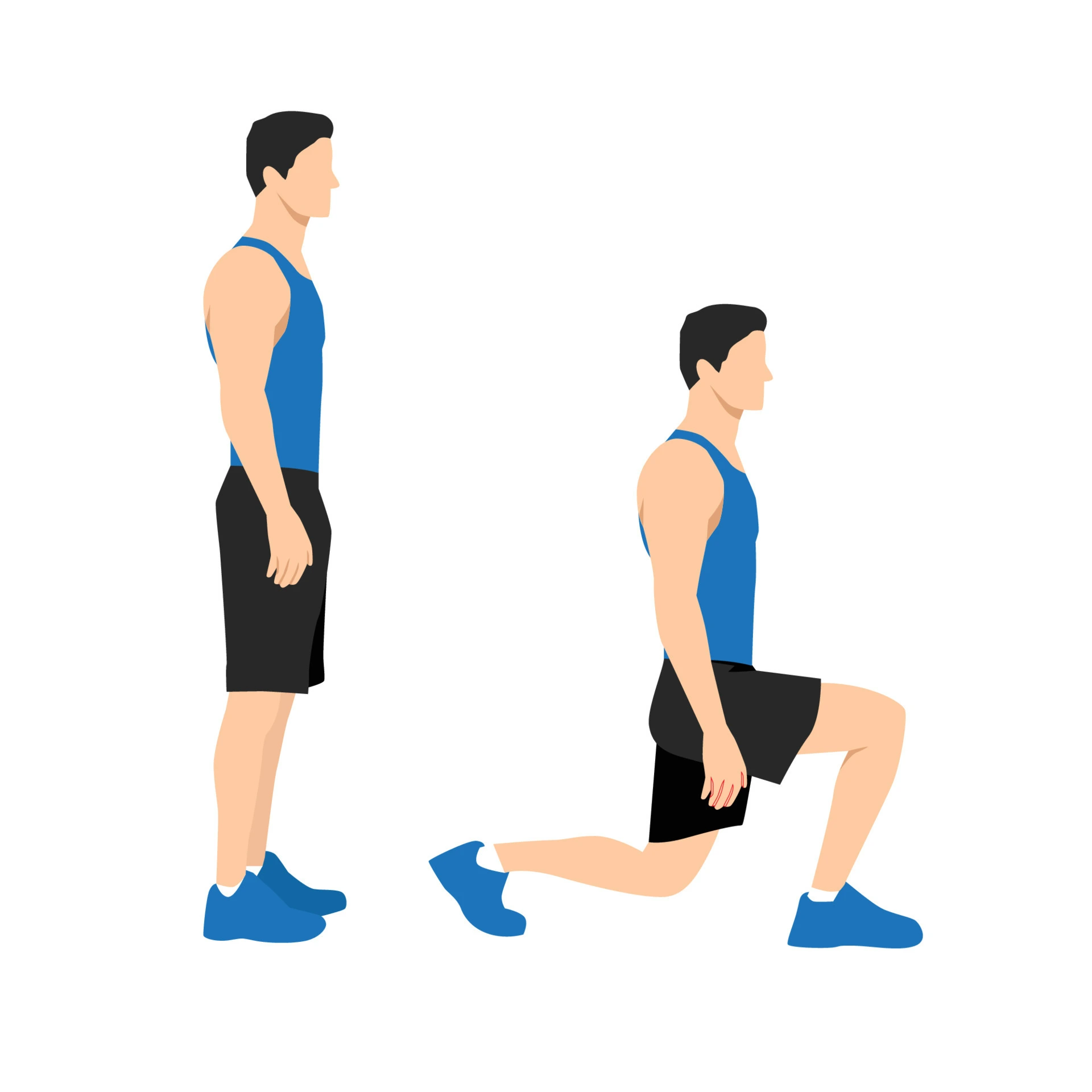
Split Squats
Bulgarian-split-squat
Spread your legs wide apart and take a big stride forward.
Now lower yourself to the floor with equal weight on both legs.
A 90-degree angle is formed between your thigh and calf when your front leg is at its lowest point.
Next, place your rear leg in front of you to reverse the leg positions.
Burpees
burpee
Strike a push-up position.
To complete a push-up, instead of lowering your body to the ground, spring forward with your feet until your knees nearly touch your elbows.
Then lift your arms off the floor and lower yourself into a squat.
Push yourself up from the squatting position using the strength of your leg muscles to jump up.
Your legs should be perfectly straight and your tiptoes just above the ground when you are at your tallest position.
Then, repeat the entire operation backward until you reach your starting point.
You can make this exercise more intense by holding your push-up or squat position for a little while longer.
Push-ups
Push-ups
Every one of the four limbs ought to be grounded.
Place your hands on the ground.
Now extend your legs backward, being sure to tense every muscle in your body.
Place your arms at chest height, about shoulder-width apart.
Flex your arms and drop yourself until your nose nearly touches the floor from this posture.
When finishing the exercise, make sure to tuck your elbows securely into your chest.
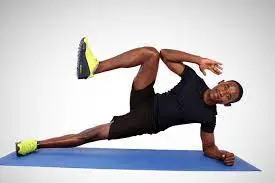
Side-Plank Crunch
Side-plank-crunch
Begin in the side elbow plank position by placing your right hand behind your head and your left elbow bent.
Raise your waist and raise your right leg to your shoulder to lightly tap your right elbow while keeping your trunk firm.
To finish a repeat, extend your right leg back to its starting position.
After thirty seconds, switch sides for a further thirty seconds and finish as many repetitions as you can.
Seated Knee Tuck
U-Boat
Take a seat on the floor or a weight bench to start this exercise. Place your hands about an inch behind your back with your fingers pointing forward.
Elevate both feet off the ground and lengthen both legs while lowering your upper body at the same time. Make sure your legs and hips are completely extended.
Return to the starting position by carefully bringing your legs back to your chest without letting your feet touch the ground.
Plank With Lateral Arm Reach
Side-plank-with-a-reach-under
starts this workout by lying on a plank.
Reach your left arm out to your side gradually while keeping your trunk stable. Hold this stance for ten seconds. Try shifting your right hand from under your right shoulder to under the middle of your chest if you feel unstable.
Return your arm to the plank position while keeping your trunk steady. Don’t round your back or bend your spine.
Repeat with the second arm after bringing the right to your side. There is only one repetition in this case.
Plank With Alternating Arm and Leg Raise
Maintaining a straight posture with your arms and legs, place your shoulders over your wrists to assume a plank position.
While keeping control, raise both your left leg and your right arm off the ground simultaneously.
Avoid rotating your upper body and hips. Hold on a little while longer.
To restore control and go back to the beginning position, lower your right arm and left leg.
Bird-Dog
Bird-Dog-Exercise
Maintain a straight back.
Before extending your right hand, extend your left leg.
Bring your left leg under your chest and your right elbow together by bending your head and back. One iteration is finished with this.
Diamond Sit-Up
In a supine posture, spread your knees wide and press the soles of your feet together to form a diamond-shaped set of legs, often known as butterfly legs. Straighten your arms above your head.
Inhale deeply to raise your trunk, and slightly extend your glutes by tapping the floor in front of your feet.
Return to the starting position gradually.
It has only occurred this once.
Reverse Crunch
reverse-crunches
While in a supine position, extend your legs and bend your knees. Keep your hands by your sides.
Utilizing your lower abdominals, slowly raise your hips off the floor and into your chest without using any force.
One rep is awarded for this.
T-Cross Sit-Up
Twisting-Sit-Ups
Start by lying on the floor and spreading your arms broadly to the sides of your body to create a T.
Get comfortable. Rotate such that your left hand is close to your right toe after raising your right leg. Roll slowly back down and then reverse the motion.
One iteration is finished with this.
Straight-Leg Sit-Up
Lay flat on your back, arms stretched to the ceiling and legs spread wide.
When you roll up into a sitting position, pay attention to your abdominals. Carefully roll one vertebra at a time to the mat.
This completes one rep.
Runner’s Crunch
As you roll up to a nearly sitting posture, keep your core tight and bring your right knee up to meet your left elbow.
It should feel almost like you’re jogging.
Let your knee stretch comfortably, then progressively sag your back vertebra by vertebra until your shoulders are the last to make contact with the mat.
For one rep, switch up your leg movements.
V Crunch
V Crunches
While on your back, raise your arms and legs to the lofty position. Stretch your hands toward your feet and lift your upper back off the floor.
Raise your arms and bow your knees to the ground as you
maintain your lower back pressed into the mat and your shoulders off of it.
Perform the crunch movement one more.
Double Crunch
KeeLay flat on your lower back on the floor, maintaining a 90-degree angle between two limbs.
Tense your abdominal muscles to raise your shoulders and pelvis off the ground. Feel your toes with your fingers.
Keep your core active the entire time as you gradually lower them back to the beginning position to complete one rep.
Scissor Abs
Scissor-Abs
Lie down in a supine position. Stretch your arms out to the sides of your body, pressing your palms into the earth, or bend your elbows and place your hands behind your head. Draw your knees into your ribcage by flexing them. It will be simpler to actively press your lower back flat on the floor and pull your navel in toward your spine as a result.
Raise both legs straight up toward the ceiling while maintaining firm abs and a flat lower back on the floor. Maintain a firm core as you gradually lower your right leg toward the floor until it is only a few inches above the ground. Next, progressively scissor your legs so that your left leg descends toward the floor and your right leg rises back up. One iteration is finished with this.
Oblique V-Crunch
With your right hand on the floor and your left hand behind your head, lie on your right side.
Lift your straight legs off the ground and press down into your right hand while bringing your body towards your legs.
Go back to where you were before. This completes one rep.
Tabletop to Reverse Pike
When you first sit on your bum, place your hands eight inches behind your head. Place your heels about a foot away from your hips and bend your knees. Make sure there is a hip-width gap between them.
Breathe deeply, then raise your hips off the floor until your torso is parallel to the ground and your arms are straight. Make any little adjustments required to guarantee that your ankles are beneath your knees and your hands are positioned directly beneath your shoulders. To improve the stretch in your neck and chest, lower your head behind you. Breathe out, letting go of tension in your hips, and extend your legs until your hips are hovering above the ground. Keep a straight arm motion while holding your breath. Try to keep your spine long and contract your abdominals while you balance on your hands and heels. Inhale deeply, then exhale again as you thrust yourself back into the beginning position.
Modified Windshield Wipers
Lying on your back, position your arms at a 90-degree angle with your palms facing away from your shoulders to help support your spine and shoulders.
Lift your legs off the ground and bend your knees to a 90-degree angle so that they resemble a chair.
Step your feet softly and deliberately to one side. Connect your navel to your lower back. Your spine will raise slightly off the ground as you turn but try to keep it as close to the ground as you can.
Bring your legs back to the beginning position by contracting your abdomen.
Lower to the other side, then do it again. This completes one rep.
Windshield Wiper Abs
Windshield-Wipers
Lay on your back with your arms 90 degrees out from your shoulders, palms facing down, and firmly pressed into the ground to help stabilize your shoulders and spine.
Straight legs and relaxed feet are ideal. Try to keep your hips at a 90-degree angle throughout the workout.
Carefully and gently, lower both of your legs and feet to one side. To reach your spinal column, grab your navel. Your spine will lift slightly off the ground when you turn but try to keep it pushed into the ground as much as possible.
Repeat after lowering yourself to the other side. There is only one rep left in this.
Boat Pose
Place yourself on your mat. You can balance on your buttocks by lifting your feet off the ground and bending your knees. Maintain a straight spine and legs as much as possible to avoid curving the back. If this is too hard, you can still activate your core by keeping your knees bent.
Hold on for 30 seconds.
Hollow Body Hold
Place your legs straight and your arms high, starting from the rear.
Your belly button should be brought into your spine as you firmly push your lower back onto the floor.
Breathe deeply, then slowly raise your shoulders, arms, and legs off the ground. Hold your hands and heels as low as you can while keeping your lower back pressed into the floor. Maintain firm abs and glutes. It’s acceptable to bend your knees if maintaining straight legs is too much for you. This is the position you have to stay in for thirty seconds.
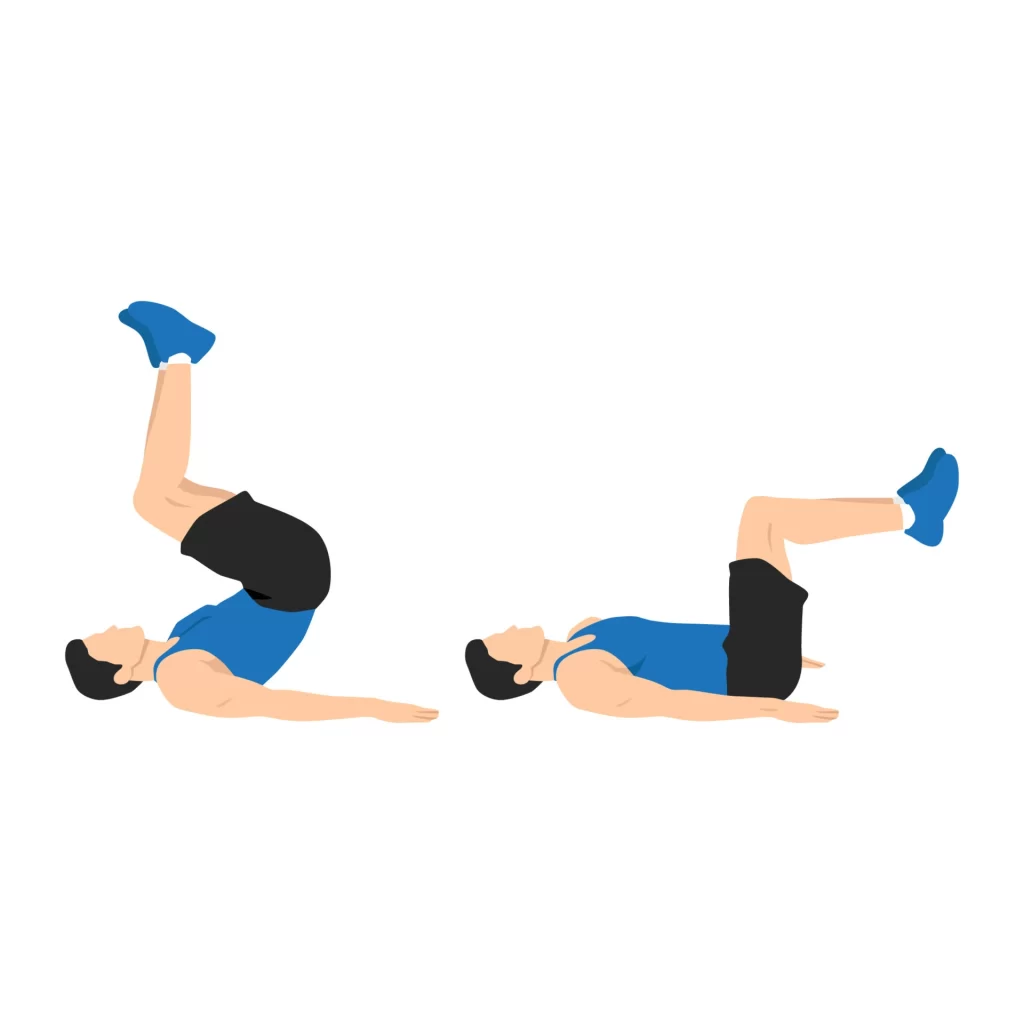
Dead Bug
Dead bug
With your hips and knees at right angles and your spine in a neutral position, lie on your back and press your palms into your thighs just above your knees.
Keeping your pelvis and rib cage in place, stretch your right arm and leg until they are almost parallel to the floor, drawing your abs in towards your spine. Keep your body and spine perfectly stable while your arm and leg move.
To finish one rep, go back to the beginning position and repeat on the left side.
Extended Dead Bug
Assume a hollow body hold position and raise your arms and legs to the ceiling.
Press your lower back onto the floor with your abs while pulling your navel to your spine.
Lower your left leg and right arm as far down as you can without letting your back arch off the ground. Extend your arm backward and stretch your leg out the other way.
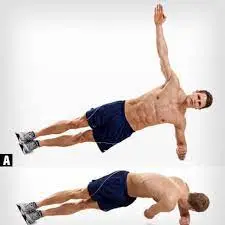
Twisting Side Plank
Stack your feet one on top of the other and place your weight on your right elbow to form a side plank position on your right side. Spread your fingers apart from your body, palm down.
To ready, breathe deeply and place your left arm behind your head.
Exhale and bring your navel to your spine to engage your deep abdominal muscles and rotate your left rib cage towards the floor. To strengthen your abdominal connection, stay there for a moment and then pull your navel in even closer to your spine.
Switch sides after completing eight total repetitions, or seven more times beginning at the beginning.
Figure Four Bridge
Figure-Four-Bridge
Assume a supine position, bending at the knees and placing your feet level on the floor with your heels only inches from your buttocks. Cross your right ankle over your left knee and stretch your arms in a low “V” next to your torso, palms up. Raising your hips a few inches off the surface requires you to push through your left heel. After a little pause, return your hips to the mat with caution.
Precaution
Here are some fundamental safety measures to follow when performing the yoga mat exercises:
Make sure your posture is correct.
Take your time with the exercises.
Avoid mat workouts like downward dog and planks if you are pregnant.
Before starting a mat workout, see a doctor if you have shoulder or back problems.
Consume no food before or following any of these workouts.
FAQ
What kind of exercises are mat exercises?
Mat exercises, especially for wheelchair users, are a fantastic place to start when it comes to strengthening the core and improving posture. It also provides an opportunity to practice fundamental postures and gait patterns that will help with daily tasks such as getting into and out of bed.
What advantages do mat activities offer?
builds up the core muscles. improves elasticity and equilibrium. Enhances alignment. Increases Total Power and Stamina. Promotes Weight Loss. Reduction of Stress. Enhanced Cognitive Performance.
Are mat workouts effective?
When you do the basic Pilates movements mindfully, you’ll find that you become more formed, flexible, and powerful. for learning the proper muscle activation techniques as well as strength training.
What materials are used to make exercise mats?
Material: Exercise mats can be made from PVC, rubber, foam, or even fabric. Rubber mats may be less soft than PVC mats, but they are more likely to stay in place. Though both are wonderful, the choice ultimately comes down to how you want to utilize this mat.
References:
Tirgar, P. (2023c, December 31). Top Mat Exercises for a Full-Body Workout. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/top-mat-exercises/
Dip, P. (2023, July 31). Training with The Exercise Mat – All Benefits and The 10 Best Exercises. Pullup & Dip. https://www.pullup-dip.com/blogs/training-camp/exercise-mat-exercises
Findley, D. (2024, February 4). Mat Exercise Program for Strength and Flexibility – 17 Movements. Over Fifty and Fit. https://overfiftyandfit.com/mat-exercise-program/
Ryan, M. (2020, April 28). 32 No-Equipment Ab Exercises You Can Do on a Mat. Popsugar. https://www.popsugar.com/fitness/ab-exercises-you-can-do-on-a-mat-47181352
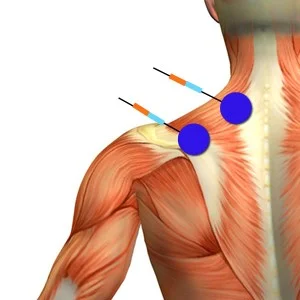
Trapezitis, also known as trapezius muscle strain or trapezius myalgia, is a condition characterized by inflammation and pain in the trapezius muscle, which extends from the back of the neck to the shoulders and upper back.
Neck soreness and spasms are further symptoms of trapezius, an inflammation of the trapezius muscles. It is growing more and more prevalent among those who use computers and work at desks, as well as those who perform manual labor or frequently strain their neck and back muscles. Understanding trapezitis’s causes, symptoms, and suggested treatment is crucial for efficient management.
Although the muscle is responsible for many of our body’s primary activities, raising the head and shrugging off the shoulder are the two most crucial ones. In addition, the bulk of the muscles in the back help to stabilize, rotate, and move the shoulder blade. The largest portion of the upper back and the lower part of the neck are covered by the broad, flat muscle that gives discomfort to the back. However, because the trapezius is a large muscle, inflammation or trapezius in it can cause severe pain and hinder the movements that go along with it.
Usually lasting three to five days, the pain associated with trapezius is temporary. Two of the primary reasons for the soreness are fatigued muscles and stress. Not only that but one of the main causes of discomfort is also thought to be poor posture. People who must hold their heads steady for extended periods are more likely to develop trapezitis. Therefore, the majority of people who drive long distances or work on computers for extended periods suffer from trapezitis.
Trapezius Muscle Anatomy
The huge, agreeable muscle known as the trapezius extends from the base of the skull to the lower thoracic vertebrae and continues laterally to the scapular spine. There are three useful components to it:
Upper (descending) fibers: These fibers enter the clavicle from the base of the head. They aid in head rotation and raise the scapula.
Middle (transverse) fibers: These fibers enter the acromion process of the scapula after emerging from the spinous processes of the upper thoracic vertebrae. They aid in shoulder adduction and scapula retractions.
Lower (ascending) fibers: These fibers enter the scapula’s spine after emerging from the spinous processes of the lower thoracic vertebrae. They aid in shoulder rotation by depressing the scapula.
The ventral rami of C3 and C4 as well as the spinal accessory nerve (cranial nerve XI) innervate the trapezius muscle. It is supplied by the transverse cervical artery as well as the dorsal scapular artery.
Numerous actions require the trapezius muscle, such as:
Elevation of the scapula
Depression of the scapula
Retraction of the scapula
Rotation of the scapula
Elevation of the clavicle
Depression of the clavicle
Rotation of the head
Adduction of the shoulder
Extension of the shoulder
Lateral flexion of the neck
Additionally, the trapezius muscle aids with balance and posture maintenance. It keeps the shoulders level and supports the weight of the upper body.
Nerve supply of trapezius muscle:
Two distinct nerves innervate the trapezius muscle:
The spinal accessory nerve, also known as Cranial Nerve XI, gives the trapezius muscle its motor innervation, which enables it to contract and carry out its different tasks.
The trapezius muscle receives sensory innervation from the ventral rami of the C3 and C4 spinal neurons, enabling it to perceive pain, temperature, and proprioception—the awareness of one’s body’s location in space.
Blood supply of trapezius muscle:
Three major arteries give blood to the trapezius muscle:
The main blood supply to the trapezius muscle is the transverse cervical artery. The superficial and deep cervical arteries receive their branches from the subclavian artery.
Scapular dorsal artery: The bottom portion of the trapezius muscle is supplied by this artery. It originates from either the third segment of the axillary artery or the subclavian artery.
The bottom portion of the trapezius muscle receives increased blood flow from the posterior intercostal arteries, which originate in the thoracic aorta.
What Causes Trapezitis?
The moniker refers to the muscle’s trapezoid shape. Bands of muscle fibers comprise the trapezius. The superior, middle, and inferior muscle fiber bands make up the three bands. The condition known as trapezitis occurs when a person experiences inflammation in any one of these three bands.
The following are a few typical causes of trapezius:
long-term employment in the same role.
spending a lot of time reading a book in an uncomfortable position.
long-distance driving.
spending a lot of time watching television in a fixed or uncomfortable position.
Breastfeeding mothers are also susceptible to trapezius, particularly if they bow their shoulders when nursing their infant.
Some persons may also get trapezius as a result of weak neck and back muscles brought on by traumas or other medical disorders. Trauma, falls, and impacts to the neck or back can all cause trapezitis.
Acute pain and problems might result from straining the body’s trapezius muscle for the reasons listed above. In today’s world, a lot of people get pain from overusing or misusing their muscles at work or at home.
The signs of Trapezitis:
The first signs and symptoms of trapezius are usually minor and start with some neck pain.
Among the symptoms of trapezius that people frequently encounter are:
The head of the neck hurts, commonly in the evening or at night after a long day of driving or working.
The only way to repair or treat tense, stiff muscles is to give the patient a good night’s sleep or a nice massage.
People are known to continue to experience the following issues after the early stages of trapezius have passed;
Additionally, neck spasms may make it difficult to move.
When trapezius discomfort persists for a long time, it becomes increasingly problematic and can be triggered by even the smallest tension or trigger in the trapezius.
A person may experience neck and trapezius muscle pain and tightness for three to five days on average.
The patient may also report hand and arm pain during this stage of trapezitis.
In certain cases of trapezius, especially those involving prolonged standing, the persistent muscular contraction may also result in nerve compression. This frequently leads to further Trapezitis symptoms in the affected person, such as tingling, numbness, or even weakness in the arms, hands, and fingers.
The symptoms listed above are some of the typical ones that people with Trapezitis may experience. It is advised that patients who are frequently observed to be experiencing these symptoms consult a specialist and begin a workable treatment plan.
How do I know it’s the Trapezius?
To ascertain whether or not the Trapezius is affected, one must look for certain signs and symptoms. The following are typical signs of trapezius pain:
Excruciating spots or tight bands in the upper back
Upper back and neck pain
fluid retention
Spasms or twitching of the muscles
trouble with head twisting or neck movement
Headache
Arms weakness
Instead of being typical, these symptoms point to the involvement of Trapezius. Indeed, the medical practitioner may request certain diagnostic procedures, such as X-rays or, if necessary, MRI or CT.
Diagnosis of Differentiation
The following are common differential diagnoses or disorders that may exist in addition to trapezius pain:
Cervical spondylosis – Neck pain may be the first sign of cervical spondylosis, a degenerative disease of the vertebral body and intervertebral disc.
Cervical osteoarthritis – Osteoarthritis of the cervical region is a degenerative condition that is typically brought on by aging.
Cervical radiculopathy – For a variety of reasons, the nerves that emerge from the cervical region may get pinched or irritated, resulting in discomfort in the neck that typically radiates down the arm, sometimes stopping at the elbow and other times ending in the tips of the fingers and thumb.
Thoracic Outlet Syndrome – Innumerable thoracic and cervical blood vessels and nerves can travel via the thoracic outlet, which is the area between the first rib and the collarbone. Thoracic outlet syndrome occurs when the gap narrows and the structures that pass through it are compressed as a result of certain illnesses. disorders of the shoulders, such as tendinitis, tendinopathy, osteoarthritis, and rotator cuff injuries.
Impingement syndrome – Bony spurs or soft tissue damage may cause the nerve to become inflamed along its journey.
Herniation of the cervical disc – The intervertebral disc between the vertebrae may protrude from its position and irritate the nerve roots it compresses.
How to Treat Trapezitis
Conservative treatment for Trapezitis involves the use of medications such as muscle relaxants, analgesics, and anti-inflammatory drugs during painful neck spasm episodes. This should be used in conjunction with rest or physical therapy.
Using a variety of techniques (such as ultrasound, moist heat, ice, IFT, TENS, ACLT, etc.) or teaching you proper posture, neck stretching, or strengthening exercises, particularly for the Trapezius muscle, a physiotherapist may assist you in releasing the muscle spasm by releasing the trigger points.
To help the stretched trapezius muscle fibers relax, take a break.
To reduce swelling and inflammation, apply a cold compress or ice pack to the affected area for ten to fifteen minutes.
To avoid harming the skin and making the issue worse, avoid putting the pack directly on it.
In the morning, practice breathing techniques like yoga to enhance posture and encourage healthy blood flow in the region. This will lessen the likelihood that the issue will repeat and aid in a speedy and healthy recovery.
Use a comfy pillow to keep your neck and spine in the right alignment, maintain good posture, or avoid back or neck pain or strain.
To avoid trapezius muscle spasms, apply heated coconut oil or olive oil to the sore spot.
Avoid carrying heavy objects on your back.
The pain caused by Trapezitis can be reduced by wearing a cervical collar. Additionally, it stops needless movement and keeps the problem from getting worse. Only the first week following the issue is spent wearing this cervical collar. I advise against using a cervical collar for an extended period because it can lead to more issues.
Physiotherapists to ease the Trapezius Muscle Pain
Postural correction using ergonomic guidance and taping technique.
postural correction by taping
Stretching:
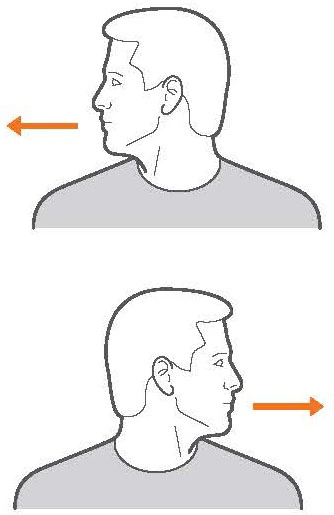
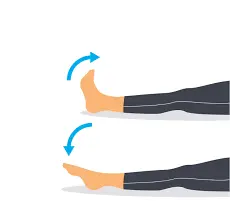
Neck Turn
Maintain a straight head and back while sitting or standing. To align your head with your shoulder, gently move it to the right. Return to the middle. The identical move must be repeated to the left.
Apply a light, leisurely motion. The position is not required of you. Your joints may become more flexible as a result of the exercise, which also relieves muscle stress.
Both sides of your neck should be stretched.
Trapezius Muscle Stretch
With your nose pointing forward, tilt your head to the left while sitting or standing. Cover your ear with your left hand and apply a slight pressure. Make a crawling motion with your other hand under your shoulders. To make sure you’re keeping it down and to the back, touch your shoulder blade. For 30 seconds, maintain the position.
Likewise, bend toward each other’s right. Don’t let your head fall to your shoulder; instead, tilt it.
Hug yourself like a bear.
bear hug stretch
Get to your feet. Hold your right shoulder while extending your left arm over your chest. Oppositely use your right arm. Employing your right hand, apply under pressure to your left shoulder region. To stretch the muscle, tilt your head forward and to the right while you do so. For 30 seconds, maintain the position.
On the opposite side, repeat the procedure.
Put a pencil between your shoulders and act as though you are.
Get to your feet. Bring your shoulder blades back and together as though you were attempting to hold a pencil there. Once you have retracted your shoulders, push them into your ribcage.
After a few seconds of holding this position, begin again at the beginning. To stretch your muscles, repeat the exercise multiple times.
To relieve tension, wrap a long, wide belt around your back.
You can join two ordinary belts or use a yoga belt. Place it above the central region of your back, just below your upper back. The end that emerges from the right should pass over your right shoulder. Take the two ends in front and hurl them over the corresponding shoulders. Move each end across your back and back to the front once more. To tighten the straps across your stomach, gently tug. Whenever you do your best to help your trapezius muscles take it easy and get out. Once the two ends of the belt are back in front, you can also buckle it. Put it on for as long as you want and tighten it as much as feels comfortable.
Using techniques for self-massage
To warm the area, apply wet heat or dry heat.
To warm the muscle, try placing a heating pad over it for 20 minutes or so. As an alternative, consider soaking your shoulder muscles in a warm bath or shower for five to ten minutes. Additionally, you can use items from your home to create your heating pad.
The sides and back of your neck should be kneaded with the other hand.
With your left arm folded over your chest, raise your hand to your right shoulder. As you would with dough, massage the muscle below the shoulder. As you carefully slide your arm behind your right shoulder, kneel. Put on just enough pressure to feel it, but not enough to cause pain. On the opposite side, repeat the procedure. If you’d like, you can repeat both shoulders two or three times.
Get on your knees and carefully move your arm down your right shoulder.
Press down on the area that is hurting using your fingertips. Hold for up to a minute after pushing down until you feel it. It should begin to relieve the strain.
The typical trigger points are located in the middle of your spine, directly above the area where your shoulder blades meet, or to the right or left of your spine, wherever your shoulder blades and neck meet in the back.
An alternative is to use a pressure tool, like a Backnobber, which is a long, curved stick with knobs on the end for massaging your own back if you’re having problems getting to the area with your fingertips. These allow you to exert pressure on different areas of your back because they are longer.
altering one’s lifestyle to alleviate suffering.
During the day, sit and stand upright.
Make sure your head is back and your shoulders are down as you do this. Imagine your body being raised by a thread, which would keep you standing.
Your trapezius muscles will be less stressed if you have proper posture. Additionally, refrain from doing things that cause you to hunch on one or both shoulders, such as carrying a phone on one shoulder.
Sleep on your side so that your head stays up straight.
Your head is always turned to one side when you sleep on your stomach, which strains your trapezius muscles. Instead, try sleeping on your side, which prevents your head from turning to the side.
You can also sleep on your back if your head doesn’t tilt to one side.
Avoid bringing a bulky shoulder bag or backpack.
Your trapezius muscles might be strained by a heavy bag. Try a belt purse instead, and only bring the necessary items.
If you have a piece of bigger luggage to handle, consider a rolling briefcase.
Make careful to swap off shoulders if you have to carry a shoulder bag. In a similar vein, your trapezius muscles may be overworked by tight bra straps. Be sure to get a bra fitted correctly.
To avoid sagging, raise your electronics.
Your trapezius muscles may become uncomfortable from slouching over, and you may find yourself drooping a lot while using a computer or smartphone. Even while you might have to hold your smartphone in front of you, it’s preferable to sagging.
To raise your laptop or screen to eye level or higher if you work at a desk, consider purchasing an elevated stand.
Make that the armrests and keyboard are at the proper height.
Because the weight of your arms can eventually strain your muscles, work in a chair with armrests. Additionally, when you sit upright with your elbows at a correct angle, make sure your arms are level with your keyboard. Typing shouldn’t need you to raise your arms. Consider using a keyboard shelf if you must lower your keyboard.
Enhancing Range and Strengthening:
trapezius positional release method.
Exercises were difficult for Theraband.
workouts to strengthen the upper body.
Lifestyle Modifications for Pain in the Trapezius:
There are easy methods to lessen or avoid pain in the trapezius muscles, such as How quickly the activities are conducted It is an easy method to prevent overuse injuries. Give your muscles enough time to recover and relax by taking frequent breaks from your work or activities. If you’re a student, for example, you can time your studies such that you write for an hour or two, take a quick break to stretch your muscles.
Stretching Every Day
Include stretching in your everyday activities. This helps to maintain the muscles’ flexibility and lessen their tightness. Because of the slouched posture that is so popular these days, the trapezius is the most used and tight muscle in the body. Aside from this constant sitting employment, trapezius workload has increased due to hunching over computers, laptops, and mobile devices for business and play.
Biofeedback
Every two to three hours, you can evaluate your posture on your own. For instance, when using a computer or laptop, try to maintain a neutral head position, relaxed shoulders, and relaxed wrists and forearms. You can use sensor devices that notify you when your posture may be off-kilter or work in front of a mirror.
Precautions and Safety
Stop the stretch and exercise you are doing if the patient feels any discomfort, numbness, or even pinching while completing any of these stretches.
As you relax the muscles in your face, neck, and shoulders, take deeper, more even breaths.
FAQs
Trapzitis: What is it?
Inflammation of the trapezius muscles causes Trapezitis, which also causes neck pain or spasms.
What signs of Trapezitis are present?
Among the symptoms of Trapezitis are: Neck or trapezius muscle pain or stiffness Pain in the upper shoulder area Excruciating neck ache
Which Factors Lead to Trapezitis?
exhaustion, stress, or tension Defective activities of daily living (ADL) and strenuous repetitive motions Sitting for extended periods without back support Head posture forward lugging around bulky bags or backpacks
Is it possible to heal Trapezitis?
Physiotherapy is a rapid treatment for trapezitis. The most frequent cause of this inflammation of the trapezius muscle is improper activity during yoga or gym poses, however, it can also be brought on by stress, poor posture, or a heavy workload from a desk job.
How can Trapezitis be recognized?
The first signs and symptoms of Trapezitis are usually minor and start with some neck pain.
Does a massage relieve discomfort in the trapezius?
It has been demonstrated that massage improves mobility in the afflicted areas and lessens pain related to trapezius strain.
How severe is trapezius pain?
Maintaining an active lifestyle, stretching frequently, and maintaining proper posture can reduce your risk of suffering from a trapezius muscle strain, which can be excruciating and restrict your range of motion. A trapezius muscle strain is usually treatable at home, but if the pain is severe or continues, you should consult a physician.
Pansari, Y. (2022, August 10). Trapezius Muscle Pain Cause, Treatment, Exercise | Mobile Physio. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/trapezius-muscle-pain/#How_can_I_be_certain_it_is_the_Trapezius
Bertolotti Syndrome is a condition characterized by the presence of a congenital anomaly known as a lumbosacral transitional vertebra (LSTV). This condition occurs when there is an abnormality in the development of the lumbosacral junction, where the lumbar spine meets the sacrum.
Four to eight percent of people may have Bertolotti syndrome, according to a 2023 literature study. Nevertheless, some specialists think the true prevalence may be higher and that the illness is underdiagnosed.
The 33 little bones that together makeup vertebrae, which are found in the spine, are divided into five sections. The portion of the sacrum, which connects the pelvis at the very base of the spine, helps the body withstand weight coming from the upper body.
Medical professionals refer to the partial or complete fusion of the sacrum with the lowest lumbar vertebrae (L5) as Bertolotti syndrome. Both or just one of the bony segments surrounding the vertebrae may enlarge, causing this.
Those L5 vertebrae may fuse with the sacrum if one or both of the bony segments at their sides mature.
Added to that, Bertolotti syndrome could have been associated with a larger range of motion in the vertebrae above L5. The subsequent factors may cause the disc that absorbs the gap between the vertebrae to degenerate more, raising the risk of a slipped disc.
What Are the Bertolotti’s Syndrome Causes?
The cause of Bertolotti syndrome is yet unknown. The discovery of lumbosacral transitional vertebrae in multiple family members may have a hereditary component. It is believed that aberrant LSTV originates from the HOX10/HOX11 molecules. The vertebral column is divided into multiple levels by HOX genes, also referred to as homeobox genes.
Plus, the distribution of an individual’s body weight among the SI joints is one biomechanical element that affects the establishment of the lumbosacral junction. The currently known etiology of Bertolotti syndrome is thought to be complex and needs more research.
The particular reasons consist of:
Congenital Anomaly
Altered Biomechanics
Nerve Compression
Degenerative Changes
What symptoms does Bertolotti’s syndrome present with?
Regarding Bertolotti’s disease, the degree of inflammation in the lumbosacral transitional vertebral (LSTV) and the severity of associated issues may affect the symptoms. Common indications and symptoms include:
Reduce Backache: Chronic, ongoing lower back ache accounts for the most common symptoms. The interface around the lumbosacral joint is where discomfort is most frequently experienced.
Characteristics similar to sciatica: Some people may have pain that radiates down their legs and buttocks from their lower back. This occurs when the surrounding nerves are compressed or irritated by the malformation.
Decreased Adaptability and Range of Motion: The abnormal spine’s structure and mechanics might result in a rigid lower back with little range of motion.
Pain During Physical Activity: Certain physical activities, such as lifting, twisting, or bending, have the potential to exacerbate pain. Prolonged standing or sitting might sometimes make symptoms worse.
An uneven pain distribution: Because of the unique form of the transitional vertebra and how it interacts with the surrounding tissues, one side of the lower back or buttocks may feel more pain than the other.
Muscle spasms: For some people, lower back muscle spasms might make their back pain and suffering worse.
Intermittent Pain: This kind of pain can fluctuate in intensity and can develop worse in reaction to specific motions or postures.
Bertolotti’s Syndrome can be misdiagnosed by imaging testing for various reasons when a patient has no symptoms at all. However, when symptoms do appear, they can significantly impact daily functioning and necessitate medical care.
Epidemiology as a field of study:
It has been determined that four to eight percent of the population in its entirety suffers from Bertolotti syndrome. On the other hand, an LSTV is far more common and can range from 4% to 30%.
Many experts believe that this disparity has resulted in a significant underdiagnosis of Bertolotti syndrome. Despite this variation, men are over twice as likely as women to have an LSTV that is connected to discomfort.
Pathophysiology of Bertolotti’s Syndrome:
In addition to an LSTV, which can be unpleasant, another person with the Bertolotti phenomenon may also have abnormal lumbosacral junction architecture and mobility.
Bertolotti syndrome could be brought on by a single iliolumbar ligament defect. The iliolumbar ligament aids in maintaining the stability of the spinal column in a normally functioning, anatomically normal spine. A new study shows that the iliolumbar ligament, which is located on the side of the aberrant articulation in patients with Bertolotti syndrome, is considerably underdeveloped compared to its contralateral counterpart.
Although two associated causes of pain and lumbar radiculopathy might complicate the clinical picture, transitional articulation may appear to be the main source of pain. It has been discovered that the existence of an LSTV is connected to disc herniations and facet joint degradation at the spinal level above the LSTV.
The disc immediately above the transitional segment, most likely L5-S1, has often degraded at considerably higher rates than the disc between the sacrum and the transitional vertebra.
People with Bertolotti syndrome often have intervertebral foramen stenosis, probably caused by degenerative changes at the facet joints above the long sagittal plane.
Diagnosis of Bertolotti’s Syndrome:
History
Despite being frequently reported by people with Bertolotti syndrome, back discomfort is sometimes confused with other types of pain. A specific examination is required to ascertain whether the patient is simultaneously experiencing radicular, sacroiliac, facet, or other forms of back pain.
Physical Inspection
When someone is suspected of having Bertolotti syndrome, they should thoroughly examine their spine to rule out other conditions such as lumbar spondylosis, neurogenic claudication, degenerative disc degeneration, and lumbar radiculopathy. During a physical examination, there may be painful regions to the touch or non-specific discomfort. They can also have a limited range of motion in the workplace. Provocation movements, reflexes, sensibility, and muscular strength should all be carefully evaluated to rule out alternative neurological causes of pain.
Evaluation
A physician will use radiography, a form of X-ray imaging, to evaluate the lumbar spine and pelvis to precisely diagnose Bertolotti syndrome. In most cases, this should give them enough details to identify the problem, if one exists.
Additionally, a physician may elect to perform additional imaging tests, including a CT scan. As a result, they will be better equipped to determine the extent of fusion between the sacrum and lower vertebrae.
Medical practitioners can determine whether Bertolotti syndrome is the underlying cause of other disorders by performing an MRI scan. Degeneration of the cartilage between the vertebrae may be one of these.
When creating treatment plans, physicians can gain a better understanding of a patient’s spine by combining CT and MRI imaging.
When to visit a physician:
There are numerous conditions that can result in chronic lower back pain, including Bertolotti syndrome. Therefore, anyone who has chronic lower back discomfort needs to think about making an appointment with a physician. To assist in identifying the underlying reason, they might do tests.
It may be necessary for other sections of the spine to support the entire weight of the upper body if treatment for Bertolotti syndrome is unsuccessful. This can overstress the spine and result in disc rupture or degeneration of the intervertebral cartilage.
Through early detection and treatment, an individual might acquire techniques to lessen the probability of future issues. A physician might advise physical therapy, prophylactic stretches, and sustaining particular levels of physical exercise, for instance.
Chronic pain needs to be decreased to treat Bertolotti syndrome appropriately and prevent future issues.
Bertolotti’s Syndrome Treatment:
Adjusting one’s lifestyle to include regular rotation and extension might lessen the burden on the spine’s injured sections.
OTC pain relievers such as Aleve, Advil, or Tylenol. The use of local anesthesia and occasionally corticosteroid injections are used under fluoroscopic guidance to minimize swelling along the afflicted nerves or directly into the pseudo-joint. Another diagnostic tool that is available is fluoroscopy.
An injection known as platelet-rich plasma (PRP) therapy is used to reduce pain and inflammation and aid in the repair of broken joints. It is administered under fluoroscopic supervision.
As a part of heat therapy, apply hot packs to relieve discomfort.
Short Wave Diathermy (SWD) is the modality. Therapy that Interferential (IFT)
A different kind of treatment known as prolotherapy involves injecting dextrose plus a strong local anesthetic into the afflicted area. area where the body’s innate capacity for self-healing might be strengthened.
Through exercise treatment, certain parts can be made stronger and their range of motion increased.
Conservative techniques:
The main course of medication for Bertolotti disorders must involve conservative measures. Nonsteroidal anti-inflammatory medications are generally well accepted, provide substantial relief, and are reasonably priced.
At the time of diagnosis, physical therapy (PT) may also be recommended. Treatments aimed at improving spinal mobility, strengthening core muscles, and providing additional pain relief methods may be included in PT. If the patient’s symptoms are not alleviated by NSAIDs and physical therapy, an injectable treatment plan could be recommended. Under fluoroscopic supervision, directed corticosteroid injections into the aberrant articulation can effectively relieve discomfort and provide long-lasting relief.
In addition to helping determine the origin of a patient’s pain and offering advice for effective management, injection treatment also has the potential to provide therapeutic effects. The only patients who have surgery are those who have tried and failed with the conservative procedures previously mentioned. Surgery, especially unilaterally or bilaterally, maybe the first course of treatment if the discomfort is solely due to improper articulation.
Direction of Surgery:
Surgery is a potential treatment for Bertolotti’s Syndrome. Even while surgery is a useful treatment option when it is required, there are risks involved. One of the most common treatment methods is lumbosacral transitional vertebral resection, sometimes known as a “Processectomy.” Patients with LSTV who have back pain due to mechanical strain on their articulation or pseudo-articulation can benefit from this therapy.
Physiotherapy Intervention:
To alleviate pain:
Manual of Diseases therapy: Approaches such as soft tissue mobilization, joint mobilization, and myofascial release promote stability and lessen stiffness.
Electrotherapy: TENS (Transcutaneous Electrical Nerve Stimulation) and ultrasound therapy are useful for reducing the body’s pain and inflammation.
Anatomical alignment and ergonomics:
Postural training: To prevent exacerbating the symptoms, avoiding poor posture is critical. Physical therapists can assist in preserving spinal alignment throughout daily tasks.
Ergonomic tip: When lifting or sitting, change postures.
Exercises to Strengthen and Stabilize:
Core strengthening: It’s critical to strengthen the muscles that support our back, such as those in the pelvic or abdominal region, to reduce discomfort.
Exercises for spinal stabilization include hip abduction, pelvic tilt, and bridging. These assist manage symptoms by stabilizing and aligning your spine.
Having flexibility and Mobility:
Stretching: To relieve stress and increase flexibility, perform light stretches that target the hip flexors, lower back muscles, and the hips.
Mobility exercises: To avoid stiffness, it’s critical to perform exercises that maintain or expand the hips’ and spine’s range of motion.
Lifestyle modifications:
Patient education: Teaching those who have this disease about their condition, the importance of regular exercise, and how to cope with discomfort is an important part of managing it over the long term.
Movement adjustments: It’s critical to advise patients to cut back on or refrain from activities like prolonged sitting or heavy lifting.
Advanced Physiotherapy Treatment:
Dry needling is one method for easing myofascial pain brought on by the tightness of the surrounding muscles.
Using athletic taping techniques can assist reduce lower back pain and offer support throughout different types of exercise.
Patient education and prevention:
From birth, the Bertolotti syndrome manifests itself. Therefore, patients have little influence over whether they may have discomfort in the transitional period in the future. Early and regular patient education may help prevent the aftereffects of chronic pain, even in cases when prevention is not possible. This emphasizes how important it is to correctly and promptly diagnose this illness.
The patient should be informed right once of any unusual anatomy or connections in the spine, and they should then be given guidance on how these things can affect their mobility and overall quality of life. Patients should also be instructed on the need to maintain their level of exercise and given information on preventative stretching and massage techniques to reduce any muscle tension brought on by the wrong spinal connection.
Issues related to Bertolotti’s Syndrome:
The LSTV is a SOURCE for abnormal mobility and spinal mechanics in cases of Bertolotti syndrome. As a result, the stress is often distributed more evenly among the surrounding motion segments. Higher pressures applied to the adjacent segment, arthrosis, and quicker disc and facet joint degeneration can all lead to neural stenosis.
When treating Bertolotti syndrome surgically, there are typical hazards involved. Infection, bleeding at the surgical site, and the need for follow-up procedures if the first one is unsuccessful are among the dangers connected with surgery. There is an added risk of nerve damage from these procedures because the spinal cord and nerve root canal are so close to the surgical site.
Surgical issues are rare, but it is important to discuss them with the patient.
At-Home Counseling:
Put on some hot packs.
Exercises for stretching and strengthening muscles should be done.
Use only light weights when lifting.
Rest well.
Summary:
Bertolotti syndrome, also known as lumbosacral transitional vertebra (LSTV), is a congenital disorder that frequently results in persistent back pain at the waist level. When the transverse process (or processes) of the fifth lumbar vertebra articulate with the sacrum, it causes abnormal spinal motion and associated pain.
This disease is characterized by an uneven spinal structure and can cause patients to have prolonged pain and discomfort. Less than 10% of people have this ailment, which often goes undiagnosed because it is mistaken for sacroiliitis. A knowledgeable specialist in spine care can use modern spinal healthcare to treat Bertolotti’s illness, which is an extremely rare cause of back pain.
FAQs
What happens if Bertolotti syndrome is not treated?
If left untreated, symptomatic Bertolloti’s Syndrome can cause early degeneration of the lumbar spine, increased discomfort, and difficulties with daily tasks. In the long run, this could cause radiculopathy, spondylosis, and disc herniations in your spine, among other problems.
Can sciatica develop from Bertolotti?
Bertolotti’s illness is one of the rare causes of sciatica that is sometimes misdiagnosed. It should be ruled out in people with back pain who do not have disc herniations or other localized illnesses that are visible on lumbar MR scans.
What sort of disability does Bertolotti syndrome cause?
Conversely, a study conducted in a clinic setting on low back pain (LBP) discovered that men had a higher probability of 9.1%6,8,9 of developing Bertolotti syndrome. Patients frequently have symptoms such as lower back soreness, gluteal pain, S1 radiculopathy, and severe functional impairment.
Why does Bertolotti syndrome result in pain?
The pain caused by Bertolotti’s Syndrome is not always present and is the consequence of many diseases caused by the LSTV. Among these conditions are quadratus lumborum and iliopsoas muscle strains, as well as joint arthropathy.
Bertolotti syndrome is treated by what kind of doctor?
Choosing a spine physician with expertise in correctly differentiating it from other back pain causes, such as facet joint discomfort, degenerative disc disease, lumbar disc problems, and sacroiliac joint pain
What causes Bertolotti syndrome to occur?
A congenital condition known as Bertolotti syndrome causes back pain because of a lumbosacral transitional vertebra (LSTV).
What’s happening the onset of Bertolotti syndrome?
Although it is a congenital disorder, symptoms typically don’t appear until one is in their late 20s or early 30s. Some of Bertolotti’s cases, on the other hand, manifest symptoms somewhat earlier in life.
Does Bertolotti syndrome benefit from heat?
There may be periods when Berlotti’s syndrome symptoms subside, followed by what are known as flare-ups. While some patients utilize pain medication, others get relief from symptoms by applying heat and ice therapy to the affected area daily.
References
Pandya, D. (2023, October 21). Bertolotti’s Syndrome – Cause, Symptoms, Treatment. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/bertolottis-syndrome/
Physiotherapist, N. P.-. (2024, August 6). Bertolotti’s Syndrome – Cause, Symptoms, Treatment. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/bertolottis-syndrome/
Vevers, S. (2023, November 29). What to know about Bertolotti syndrome. https://www.medicalnewstoday.com/articles/bertolotti-syndrome
There may be certain difficulties and experiences associated with growing up with Ehlers-Danlos Syndrome that are not always apparent to others. From seemingly straightforward activities to more intricate facets of everyday life, people with EDS frequently acquire unique viewpoints influenced by their condition.
In this article, we’ll look at 23 indicators that show how having Ehlers-Danlos Syndrome as a child might affect a person’s mental and physical health. Gaining knowledge of these indicators can help one better understand the lived experiences of people with EDS and increase empathy and understanding of the difficulties they face.
What Is Ehlers-Danlos Syndrome?
The skin, joints, and blood vessels are among the connective tissues in the body that are impacted by the rare genetic illness known as Ehler-Danlos syndrome.
Connective tissues are flexible because of the proteins and other materials that comprise them.
People with Ehler-Danlos disease have reduced collagen’s tensile strength.
Even though Ehler-Danlos syndrome is a congenital condition, a patient may not be diagnosed for years.
Variants Associated with Ehlers-Danlos may be inherited.
Types of Ehlers-Danlos Syndrome
There are thirteen forms of Ehler-Danlos syndrome (EDS), most of which are rare.
Hypermobile EDS (hEDS) is the most common form of Ehler-Danlos syndrome.
Symptoms of hEDS include:
Hypermobility of joints
Joint instability and dislocation risk
Joint pain and clicking sounds
Skin that bruises easily
Digestive problems, such as heartburn
After getting up, feeling dizzy and experiencing a faster heartbeat
Incontinence of the urine
Is Elhers-Danlos Syndrome Genetic?
Ehler-Danlos syndrome is influenced by genetics. Over 20 genes have been connected to EDS.
Genes that have been linked to Ehler-Danlos syndrome include:
COL1A1
COL1A2
COL3A1
COL5A2
These genes provide instructions on how to make different types of collagen.
Changes (variants) in these genes can cause weak bones, skin, or other body tissues by interfering with the generation or processing of collagen.
There are 23 signs that you were born with EDS (Ehlers-Danlos syndrome).
Ehler-Danlos syndrome may be the cause of these symptoms for some people, while other people may think they are related to another underlying medical condition.
23 commonly observed signs are:
High flexibility of the joints.
Clumsiness.
Frequently tripping or falling.
Commonly occurring joint dislocations, particularly to the knee or elbow.
Being able to bend your thumb or fingers back.
A higher risk of bone fractures.
Knees that are overextended.
Experiencing double-jointedness.
Having a fear of dislocation that prevents you from relaxing your joints.
Foot problems that keep coming again, primarily pain and discomfort.
Bloating, diarrhea, acid reflux, and other digestive issues.
Extreme fatigue.
Use a different grip while using a pen or pencil to avoid pain, discomfort, or dislocation of your finger joint.
Spend more time on your everyday chores.
Headaches, vision issues, or postural orthostatic tachycardia syndrome (POTS) growing.
Early onset of persistent physical pain.
Running in a style that makes you stand out from the crowd.
You are picky about what you wear to protect your sensitive skin.
In joints, a popping or clicking sound is created.
Ankle pain that is becoming worse with time.
Not being able to move fast.
Treatment for Ehlers-Danlos Syndromes
There is no cure for Ehler-Danlos syndrome.
Controlling the symptoms and preventing more issues are the main objectives of therapy.
Treatment options for Ehler-Danlos syndrome include:
Medication: Over-the-counter pain relievers are usually the cornerstone of EDS therapy. Additional medications may be required in cases of serious damage.
The goals of medical treatments for EDS are to control certain symptoms and avoid consequences. To increase skin suppleness and lessen irritation, for example, you can be prescribed lotions or ointments if you have skin issues.
An essential part of treating EDS is managing pain. However, since certain medicines might worsen symptoms or produce unpleasant effects, it’s crucial to know which ones to avoid if you have EDS. People with Ehler-Danlos syndrome have delicate blood arteries.
Physical therapy: People with Ehlers-Danlos are more prone to experience dislocations in joints with weak connective tissue. It may be recommended that physical therapy be undertaken to strengthen muscles and stabilize joints.
Recall that the purpose of therapy is to enhance your quality of life in addition to managing your EDS symptoms. You may better control your symptoms and live a satisfying life by collaborating with your healthcare team and making the required lifestyle changes. See our page on EDS therapies to learn more about your choices for therapy.
Surgery: People who often dislocate their joints or burst their organs or blood vessels may require surgery. Throughout their disease, people with EDS usually get assistance from a wide range of medical professionals.
Surgery may be considered in extreme circumstances or when medicines and lifestyle changes are ineffective. These can involve joint replacements or operations to fix organs or blood arteries that have been injured. To fully comprehend the possible dangers and advantages, it is imperative that you have a detailed discussion with your healthcare physician about these alternatives.
The EDS healthcare team usually consists of a physical therapist, an occupational therapist, and counselors. Genetic counseling can help people better understand their condition, how it is inherited, and whether they can pass it on to their children. Many of the symptoms of EDS may be managed, despite the fact that there is no particular therapy for it.
Lifestyle Modifications
Changing one’s lifestyle is essential for controlling the symptoms of EDS. Striking a balance between exercise and relaxation is crucial. Frequent mild exercise helps build your muscles, increase cardiovascular health, and stabilize your joints. However, it’s also crucial to stay away from activities that require abrupt or startling movements or that have a significant risk of harm.
For instance, because of the possible effects on blood vessels, vEDS, contact sports, hard lifting, and activities that have a high risk of falls, such as skateboarding or skiing, should be avoided.
Physical therapy could be helpful if joint hypermobility is one of your symptoms. By strengthening the muscles surrounding your joints, some workouts can lower your risk of dislocations and other problems. For further information, see our guide on EDS physical therapy.
Summary
Ehler-Danlos syndrome (EDS) is a rare hereditary disease that affects the body’s connective tissues.
Although Ehler-Danlos syndrome is a congenital disorder, affected individuals may not experience symptoms for years or even decades.
There are around thirteen types of Ehler-Danlos syndrome, with hypermobility EDS (hEDS) being the most common.
Ehler-Danlos syndrome is a genetic condition associated with more than 20 genes, including COL1A1 and COL1A2.
Most Ehler-Danlos patients are unaware of their disease because they cannot identify signs such as simple skin bruises and joint dislocation.
FAQs
Should individuals with EDS become parents?
Patients may also have a higher chance of experiencing serious bleeding after giving birth, depending on the kind of EDS. You might want to talk to your doctor and a genetic counselor about your reproductive choices because of the possible hazards of getting pregnant and passing the sickness on.
Do those who have EDS suffer mental health problems?
Additionally, individuals with EDS are more likely to have mental health issues like mood disorders and suicidal thoughts and actions, as well as pains like headaches, muscular soreness, neuralgia, stomach pain, and malaise.
Which odd symptoms are associated with EDS?
Other skin traits and symptoms, such as atypical skin texture, skin fragility, very thin skin, delayed wound healing, and irregular scarring, may also be present in people with a particular kind of EDS. Skin hyperextensibility or unique skin traits are not present in all people with an EDS type.
Which facial characteristics are characteristic of EDS?
The characteristic facial traits of a tiny nose, thin upper lip, short earlobes, and large eyes are frequently shared by people with vascular Ehlers-Danlos syndrome. The underlying blood vessels are highly apparent through the skin in those with fair complexion.
Do those who have EDS appear younger?
Many people with EDS don’t get wrinkles as they age because their skin’s collagen is so elastic. In addition to making the skin feel incredibly smooth, this collagen may help EDS sufferers seem younger. The skin is even described as “velvet-soft” by doctors.
Can someone with Ehlers-Danlos lead a regular life?
For the remainder of your life, you should anticipate managing the symptoms of Ehlers-Danlos syndrome. EDS has no known cure. However, after you learn to control your symptoms, you should be able to engage in all of your regular activities. Certain types of severe physical exercise, such as contact sports, may need to be avoided.
What effects does Ehlers-Danlos have on hair?
Both the scalp and the body may have scant hair. It often grows slowly, is fragile, and has a pale color. It might be difficult to handle, curled, coiled, and extremely delicate. Male beard development and body hair throughout adolescence could not be impacted.
Why do medical professionals not accept EDS?
Although the precise etiology of EDS is unknown, experts are aware that it is a hereditary illness. Chronic Ehlers-Danlos disease can last for years or even a lifetime. EDS does not have a diagnostic test. Doctors may find it challenging to correctly identify EDS in affected persons due to a lack of official diagnosis guidelines.
How do EDS sufferers feel?
Since individuals with EDS seem healthy on the outside but suffer from pain and fatigue that can make daily activities like cooking or dressing feel difficult, the condition is known as an “invisible” sickness.
How was the diagnosis of Ehlers-Danlos syndrome made?
The most common types of EDS are as follows: Hypermobile EDS is commonly characterized by joint hypermobility, velvety, easily bruised skin, and persistent bone or muscle pain. Classical EDS: Signs and symptoms might include weak muscles, hypermobile joints, delayed development, and easily bruised, elastic, stretchy skin.
Do those who have EDS appear younger?
Yes, having Ehlers-Danlos syndrome might make you appear younger. People with EDS do not get wrinkles because of the collagen’s increased flexibility. Their skin is smooth and young as a result.
Which facial characteristics are characteristic of EDS?
Additionally, its skin is translucent and sensitive, making it extremely vulnerable to damage.
References
Physiotherapist, N. P.-. (2023d, December 13). 23 Signs You Grew Up With Ehlers-Danlos Syndrome. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/23-signs-you-grew-up-with-ehlers-danlos-syndrome/
Life, X. (2023, March 28). 23 Signs You Grew Up With Ehlers-Danlos Syndrome. https://www.linkedin.com/pulse/23-signs-you-grew-up-ehlers-danlos-syndrome-xcode-life-sciences/
23 Signs You Grew Up with Ehlers-Danlos Syndrome | Relief Now. (n.d.). https://www.reliefnow.com/articles/23-signs-you-grew-up-with-ehlers-danlos-syndrome
Steppage gait, which is additionally known as high stepping or neuropathic gait, is an improper gait type that results in foot drop or ankle equinus because of its absence of dorsiflexion. When walking, someone must elevate their leg higher than usual because the foot hangs with the toes facing downward, scraping the ground.
Foot drops could be caused by disruption to the deep fibular nerve. This pattern of walking is frequently observed in people with peripheral neuropathy, spinal cord injuries, muscular dystrophy, multiple sclerosis, neurological disorders, or other conditions that cause nerve loss or muscle weakness in the lower limbs. Steppage gait is often treated by addressing the underlying source of the difficulty, which may entail surgery, physical therapy, or bracing.
What is Steppage Gait?
A sign of an irregular gait or walking pattern is steppage gait, which is defined by excessive toe and foot raising during the walking swing phase. Various other names for it include foot drop gait or drop foot gait.
The foot is raised and the toes are pointed upward during the swing phase of normal walking to clear the ground. In contrast, in patients with steppage gait, the muscles that lift the foot and toes are either weak or paralyzed, giving in a high-stepping gait in which the foot is raised higher than necessary to clear the ground.
One reason that leads to the Steppage gait is the trouble in elevating the foot when walking due to decreased muscle strength regulating the ankle joint’s dorsiflexion. Comparable to foot drop, however, foot drop is uncommon. When the muscles that lengthen the foot when walking suddenly weaken, this is the typical appearance of the patient.
The medical record usually comprises a fracture-causing incident, prolonged inactivity, unusual behaviors, surgical procedures, or a lower limb in a severely tight cast. A previous diagnosis of collagen vascular disorders resulting in nerve ischemia is one of the additional factors. Foot drop is an additional indicator that upper motor neurons have been damaged.
The most common cause of peripheral neuropathies, which can result in either unilateral or bilateral foot drops, is diabetes. The same justification applies to hemiplegia and aphasia.
Statistics
Men are typically more likely than women to be suffering from peroneal neuropathy; their probability is 2.8 to 1. Ninety percent of peroneal lesions are unilateral, meaning they don’t favor one side over the other.
The incidence after total knee arthroplasty (TKA) varies between 0.3 and 4%.
Three to thirteen percent of patients may experience foot drop following proximal tibial osteotomy.
What causes the Steppage Gait?
People with lower limb nerve injury or muscle weakness, such as those suffering from peripheral neuropathy, spinal cord injuries, muscular dystrophy, or multiple sclerosis, frequently exhibit this kind of stride.
Additionally, several neurological illnesses that influence the neurons controlling the ankle and foot muscles may be contributing factors.
Foot drop occurs when the anterior tibialis muscle, which is situated in front of your shin bone, weakens or paralyzes.
Among the most prevalent causes are injuries caused by trauma, pelvic bone fractures, tibia or fibular head fractures, tightened plaster casts, long-term lithotomy positioning during surgical procedures, compression from a space-occupying lesion, vascular impairments like those linked to lupus, or Waldenstrom macroglobulinemia, which can result in vasculitis and nerve ischemia.
Primary demyelinating neuropathies can also be inherited or hereditary. They may be largely demyelinating, mostly axonal, or a combination of the two.
Primary demyelinating neuropathies, whether acquired or congenital, are also common.
Toxin exposure to radiation, infections from bacteria or viruses, and chemotherapy medications like vincristine or vinblastin are the primary contributors to axonal neuropathies.
Combined peripheral polyneuropathies can result from several illnesses, including diabetes, alcoholism, and renal failure.
Cerebrovascular accident (CCA) symptoms include dysphagia, dysarthria, and hemiplegia or hemiparesis.
The “cock-walk gait,” which is the screening of the upper motor neuron type, has a high steppage stance and a drop in the foot.
What are the signs of Steppage Gait?
People who walk with a steppage stride may show.
A foot that is raised excessively even with walking.
The dragging of toes.
A gait that is awkward or erratic.
Heightened the chance of falls and trips.
Foot drop (incapacity to elevate the forefoot).
What is the diagnosis of the Steppage Gait?
In the event of trauma, the diagnostic evaluation should include routine X-rays of the pelvis and tibia or fibula to identify any fractures or dislocations.
\When plexopathies are suspected, the results of an MRI may be suggestive.
Rheumatoid factor, an antinuclear antibody (ANA), and other relevant laboratories should be investigated in patients with collagen vascular disease.
To rule out sepsis, the total blood count, differential count, and SMA 18 should be taken into account.
Electromyography (EMG) and nerve conduction velocity (NCV) investigations will discover denervation potentials and motor units. Peroneal neuropathy has nothing to do with tibialis posterior weakness; instead, it is triggered by lumbar plexopathy, a lumbosacral trunk lesion, and L5 radiculopathy.
It is easier to differentiate the lateral trunk of the sciatic nerve involvement in peroneal neuropathy from the short head of the biceps because that portion is weaker over time. For an evaluation of both of these muscles, EMG is beneficial.
What are the treatments for the Steppage Gait?
Conservative Treatment
Medication:
Medications may be recommended to treat any underlying medical conditions that may be the cause of the steppage gait. For ailments such as peripheral neuropathy or multiple sclerosis.
Physical Therapy:
Physical therapy recommendations for pain management, ankle range of motion (ROM) exercises to prevent stiffness, and strengthening exercises for weak muscles are all crucial in moderately intense circumstances.
Surgical Interventions:
When there are serious nerve damage or structural problems surgery may be necessary.
Nerve Decompression: If nerve compression is the root of the steppage gait, the pressure can be released surgically.
Tendon Transfer: A healthy tendon is transferred to improve the anterior tibialis muscle’s function.
Ankle Fusion: In certain situations, the steppage gait can be corrected by fusing the ankle joint.
Physical therapy for the Steppage Gait
Physical treatment is essential to regulating steppage gait.
Gait training teaches appropriate walking strategies to correct foot drop.
Balance and coordination training helps to improve overall stability and reduces the danger of falling.
Stretching helps to maintain lower-limb flexibility.
Assistive devices, such as canes or walkers, may be advised for increased mobility and safety.
Exercises for the Steppage Gait
Dorsiflexion
Dorsiflexion/Plantarflexion
Flexing your ankle forward toward the surface of your shin is known as ankle dorsiflexion, and it’s a basic ankle-strengthening exercise. This step will bring back your ability to walk properly.
Start by adjusting your knee.
Simply point your foot down near your nose while moving your ankle. Continue until you feel pain or can walk correctly with the assistance of this action.
Hold this position for fifteen seconds.
Return to your normal posture now.
Plantar flexion
Your ankle goes downward and outward when your plantar flexes. Increasing your range of motion (ROM) might be feasible.
To start Adjust your knee.
All you have to do is stretch your ankle by directing your foot moving forward. Keep doing this until you feel uncomfortable or you’ve reached your limit.
Hold this position for fifteen seconds.
Restore your position to normal.
Inversion
ankle-eversion-and-inversion
When you point your ankle inside near your body, you execute an inversion. To turn your foot internally, move your ankle upward while preserving your toe pointed.
The bottom of your foot should be facing the opposing leg. Until you start to experience pain or can no longer bend your foot inward, continue going.
Hold this position for 15 seconds.
Return to your typical position.
Inversion and eversion
Eversion
It is the motion of the ankle, which encompasses the leg’s outward movement. This exercise will aid in increasing your ankle’s range of motion.
Continue your toe pointing and slowly rotate your ankle to turn your foot away from your other leg.
Continue this exercise until you either lose the ability to turn your foot outward or start to feel pain.
Hold this position for 15 seconds.
Return to your normal posture now.
Calf-raising while seated
seated-calf-raises
By using partial weight-bearing in these exercises, you can put extra strain on the damaged ankle.
They also aid in strengthening the ankles. Ten repetitions of this should be made in a single set of exercises.
You must be in a comfortable seat with your injured foot resting on the ground.
Try to lift your heel as high as you can while preserving your steady posture.
Return your heel to the floor.
Weight shifting while standing.
Weight-shifting-in-standing
Initially, you may need to lessen the weight you put on the wounded leg. This ensures that your ankle is safe while it repairs.
After that, you can progressively raise the weight on your wounded ankle. Because weight changes strengthen the ankles, they are perfect for this kind of workout.
You can stand up straighter if you hold onto something sturdy.
Your affected foot must carry some of your body weight.
Hold the position for 15 seconds.
One leg Standing
One leg Standing
By doing these ankle-strengthening exercises, you can put greater weight on the wounded foot. Make sure your ankle can handle the strain before putting all of your weight on it. Lift the normal foot off the ground and stand on the damaged foot.
Hold the position for 15 seconds.
As you return your weight to your strong foot, maintain your center of gravity.
Perform every ten times in a row.
Calf raising in standing
calf-raise
Once your complete body weight can be maintained, try calf raises.
Raise the healthy foot off the ground and place it on the foot that is injured.
As you get up, lift your heel off the ground and place your foot just on the injured foot’s ball.
Hold the position for 15 seconds.
Restore your weight to your strong foot while maintaining your sense of equilibrium.
Sidestepping
Stepping from side to side is an exercise that strengthens the ankles. Lay a rolled towel or other short object on the ground next to the injured foot.
While standing on the suffering foot, cross over the towel.
Then use your uninjured foot to cross over the stuff and raise yourself.
When you step back over the towel, stay on the foot that is not injured.
After that, stand up straight with both feet and cross the injured foot over the towel once more.
As your recuperation advances, you can intensify this workout.
Neuromuscular Electrical Stimulation
Foot drops are frequently treated using neuromuscular electrical stimulation (NMES), a form of electrical stimulation. It is a type of electric stimulation that helps your muscle learn to contract correctly again by artificially contracting it.
When using NMES, your therapist will probably mention a few basic steps.
The basic process is as follows.
Keep your anterior tibialis muscle visible at the front of your shin.
Your physical therapist will apply tiny adhesive electrodes on the front of your shin.
After that, an electrical stimulation device will be linked to the electrodes.
Your physical therapist will next activate the equipment and raise the stimulation level.
Your shin’s front may probably begin to tingle.
Until you can see your anterior tibialis muscle contracting, you should increase the intensity. Your ankle will inadvertently flex upward.
Try to raise your ankle and toes even higher while using the NMES device to bend your ankle.
Use of Assistive Devices
Ankle-foot orthoses
Ankle foot orthoses (AFO)
To help you walk correctly, your physical therapist could suggest that you utilize an aid. For this, a wheeled walker or a quad cane, which has a base with four modest feet, can be utilized. The proper use of your aid can be verified by your physical therapist.
Sometimes you may become permanently paralyzed by your anterior tibialis muscle. If so, you may benefit from a specific kind of brace called an ankle-foot orthosis (AFO).
By helping to lift your foot and toes off the ground, this brace reduces the chance that you will trip over your toes. You should no longer have a high steppage stride when you wear an AFO.
Elastic Band
As a short-term solution for anterior tibialis weakness, raise your foot when walking with an elastic band.
Tie the band around your leg just below the knee and wrap it around the ball of your foot. As you swing your leg forward, the elastic band keeps your foot up. Raising your toes off the surface no longer requires a high step.
Naturally, wearing an elastic band around your leg all day might not be feasible. However, you can continue to move securely if you use it as a temporary solution.
Summary
The excessive lifting of the foot and toes during the swing phase of walking is a characteristic of steppage gait, a form of aberrant gait or walking pattern. With the correct diagnosis and a comprehensive treatment plan that includes physical therapy, patients can improve their walking patterns and reduce their risk of falling, even though steppage gait can seriously reduce movement and living standards.
FAQs
What is the difference between a slap gait and a steppage stride?
When the foot touches the ground, the gait becomes slapping. Occasionally, when walking, he attempted to raise his thigh to clear his toes, resulting in a steppage stride.
Which muscle is weak with a steppage gait?
Steppage gait requires a greater-than-normal bending of the knees, which raises the feet off the ground. Muscle atrophy and weakness typically affect the intrinsic foot and peroneal muscles as well as the leg muscles.
For what reason does steppage gait happen?
Although most people think that this disorder is related to foot issues, it is caused by a spinal injury or underlying condition. Steppage gait and drop foot are frequently caused by: ALS, amyotrophic lateral sclerosis MS, or multiple sclerosis.
What is the steppage gait known by another name?
A type of gait anomaly known as steppage gait (high stepping, neuropathic gait) is characterized by foot drop or ankle equinus as a result of lost dorsiflexion.
What kind of nerve injury results in a high gait?
Muscle atrophy or peroneal nerve injury (from spinal stenosis or a herniated disc, for example) can result in steppage gait.
References
Patel, D. (2023c, May 5). Steppage Gait – Cause, Symptom, Treatment, Exercise – Samarpan. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/steppage-gait/
Wikipedia contributors. (2024a, May 5). Steppage gait. Wikipedia. https://en.wikipedia.org/wiki/Steppage_gait
Nori, S. L., & Das, J. M. (2023, August 7). Steppage Gait. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK547672/
Compound exercises are multi-joint movements that engage multiple muscle groups simultaneously, making them highly effective for building strength, improving coordination, and enhancing overall fitness.
Unlike isolation exercises that target a single muscle, compound exercises, such as squats, deadlifts, and bench presses, work several muscles at once, leading to better functional strength and more efficient workouts.
A strong foundation of strength throughout the body benefits bodybuilders, athletes, and even casual lifters. Lifting heavier weights, especially in complex exercises, will eventually lead to increased muscle mass, improved performance, and an improved quality of life. Although isolation exercises are useful, they don’t exert the same demands on one’s ability to balance and coordinate, bear weight, activate several muscle groups, or train the body in a broad “functional” manner as compound exercises.
Even though there are many great compound lifts, a strength and hypertrophy training program should emphasize some exercises over others. These are more complex workouts that use a variety of joints and muscles in a broad range of motion. Rather than recommending what you believe to be the best compound lifts to engage the specific muscle groups efficiently. If you want to acquire absolute strength, you can do the majority of these massive difficult exercises for one rep max without losing any strength.
This is one way that they are different from other smaller compound lifts. Your fundamental lifts should be the main focus of your training, with the weaker compound and accessory workouts utilized as a complement. Last but not least, these are your main complicated lifts, therefore you’ll likely just be using a barbell and plates.
Lifting heavier items is possible when you use a barbell. Dumbbells and machines work best for smaller compound exercises and isolation exercises, except beginners, who will probably benefit from dumbbells the most, and intermediate to advanced lifters who use machine and dumbbell compound lifts for muscle building or any other purpose specific to their training targets.
How should intricate exercise regimens be included in your daily schedule?
No matter how often you work out, your training regimen should include compound motions. Compound motions are quite versatile and easy to include in everyday activities. They don’t always need to be loaded, either. Exercises like the barbell back squat are challenging, especially when performed bodyweight. This enables you to modify your difficult exercises’ muscle focus, load, and intensity every time you work out. Compound movements offer a multitude of setup choices, making them extremely user-friendly.
Before performing any isolation exercises, concentrate on a large compound action, such as a squat or deadlift. This will ensure that you are concentrating on your most taxing exercise when your energy is at its highest. Depending on the severity of the exercise, Sung suggests three to five sets of five to twelve repetitions for beginners; if you’re using heavier weights, lower the rep count.
Should an individual only do compound exercises?
Even while hypertrophy, strength, fat loss, and endurance are the most important and desired attributes for most people, a training routine that just consists of compound lifts is usually not the best option for people who want to achieve a variety of fitness goals. So, isolation exercises have a purpose.
Since larger muscle groups are primarily responsible for the general movement patterning, more complicated motions could not adequately target specific muscle groups. It might be challenging to address particular deficits and muscle imbalances when complex lifts always put the stars in the spotlight. You can be quad-dominant during back squats and hamstring-dominant during deadlifts, so your glutes must work.
Furthermore, it’s possible that during complex lifts, some muscles exhaust themselves before others. Your legs may tire out before your lower back muscles do. To keep your lower back from tiring out before your legs and glutes in this situation, isolate it and strengthen it with hyperextensions. You may also need to do more isolated leg workouts, such as leg presses, to target your quadriceps. Assistance lifts are also available, although these should not be mistaken with more isolated compound motions; more on this later. Furthermore, you could find that some muscles need extra attention because the complex lifts aren’t working them through their full range of motion, which is advantageous for hypertrophy.
You may find that bent-over rows are not enough for your biceps, and that bench press and overhead press are not enough for your triceps and side/rear delts. For these tiny muscle groups, isolation workouts are essential for both muscular growth and aesthetic appeal. Even while you may have powerful shoulders by simply completing the overhead press, your side delts will stay undeveloped since the exercise primarily targets your upper chest and anterior deltoid, not your broad, popping shoulders.
Another significant advantage of isolation workouts is their capacity to activate certain muscles without adversely influencing other muscles that need to rest. You may avoid overusing or underusing specific muscle groups by performing the solo exercise. It will also help you reach the appropriate volume for each muscle group. Finally, isolation workouts are essential for the recovery of injured individuals.
Compound exercises
Barbell back squat
barbell-back-squat
You can get a lot of strength and muscle growth in your three primary muscle groups-hamstrings, glutes, and quadriceps by performing barbell back squats. Barbell back squats enhance body awareness and coordination, lower back and core strength, and injury resilience by fortifying the joints, ligaments, and tendons that surround your knees and hips.
Both have advantages and disadvantages, including the low bar. You can generally lift bigger weights in a back squat because of the greater center of gravity, and the high bar allows you to After a deep squat, stand with your feet hip-width apart.
How to conduct: For intermediate and experienced exercisers, begin with a barbell that is either empty or loaded. Bodyweight squats should be moved to a heavier weight as the exercise becomes more comfortable. In the muscles closest to your neck and upper back, your trapezius, place the bar as you approach the rack.
Take a step or two backward. That’s one rep.
Reps and sets: three eight-to-ten-rep sets.
Pullover
Bent-Arm-Pullover
How to conduct: Using both hands, firmly grasp the dumbbell’s ends. It could seem safer to hold a larger dumbbell vertically with both hands wrapped around one end. Lift the dumbbell over your head and place it gently on the ground. The enormous latissimus dorsi muscles are the main target of this vertical pulling exercise. Save this exercise for a great dumbbell session since it may be difficult to recognize dumbbell vertical pulls.
Dumbbell Deadlift
dumbbell deadlift
Equipment required: To boost effort, a barbell option can be supplemented with weights.
How to conduct: Place the barbell so that your toes are beneath it on the floor, keeping your feet hip-width apart. To get back up, keep a strong core and push through your heels. Make sure your glutes are tight as you get closer to the top of the squat. Keep your spine straight and avoid bending it. Hold onto the bar with both hands. On the bar, place your hands just a little wider than your thighs. Make sure your heels are firmly on the floor and your knees are relaxed when you stand up. Raise yourself till the bar almost reaches your hips. Finish by putting your glutes in a raised position at the top. Take a minimum of 30 to 60-second break and repeat exercises 10 to 12 times in between sets. Complete three sets of tasks.
Reverse lunge to balance with bicep curl
reverse-lunge-to-balance-with-biceps-curl
Required equipment: dumbbells
Hold the dumbbells in each hand. Flex your arms, and hands facing your body. To regain your equilibrium, stride forward with your right foot and plant your left foot firmly on the ground. Raise your right foot off the ground while maintaining a strong planted left foot for balance. Once the left side is complete, take a 60-90 second rest. Complete two or three sets.
Squat
sumo-squat
Required equipment: not one
How to conduct: According to Toes, you should begin with your feet somewhat wider than hip-width apart. Push through your heels to return to your starting position while keeping your chest up and your core firm. At the top, clench your glutes. Perform ten to fifteen reps. Complete three sets of tasks.
Front lunge with twist
front-lunge-with-twist
Equipment needed: none
target muscles: abs, glutes, hamstrings, and hips
How to conduct: Assume a high stance, with your feet shoulder-width apart and your arms out in front of you. Make a diving motion with your arms while leaning your right foot forward. Your knee shouldn’t go past your toes, and your front leg should be at a 90-degree angle. Additionally, your back leg will be inclined by ninety degrees. Take a deep breath, thrust forward, turn your upper body to the right, and return to the center. Complete three sets of tasks
Dumbbell shoulder press on an exercise ball
Dumbbell-shoulder-press-on-exercise-ball
Workout balls, dumbbells, and abs are essential.
How to conduct: Using an exercise ball, take a seat and start to squeeze your abdominal muscles. Make sure the dumbbells are 90 degrees away from your body. Reposition your arms at a 90-degree angle and gradually elevate your elbow to shoulder height. Avoid lowering oneself below this posture as this may cause soreness in the shoulder joints. Perform 12 to 15 reps. Complete three sets of tasks.
Rotating high plank T-spine
Rotating high plank T-spine
Required equipment: not one
muscle worked: abs and shoulders
How to conduct: To maintain a tight core, begin by putting your arms beneath your shoulders. When doing this exercise, maintain a hip-width distance between your legs. As you tense your thighs and glutes, maintain a firm grip with your right palm on the ground. Lift and press your left arm toward the ceiling while keeping your hips and shoulders oriented to the left. Finish the three sets of assignments.
Dumbbell press squat
dumbbell-squat-press
How to conduct: Raise your arms to shoulder height, bend at the elbows, keep the weights near your ears, and spread your legs a little wider than hip-width apart. Flex your knees while maintaining the position of your toe and heel to make them feel like a chair.
Stepping Lunge
lunges
How to conduct: To maintain your erect posture and feet together, place ten-pound dumbbells at your sides. Beginners may practice walking lunges with just their body weight. Step forward with your left leg while keeping both knees bent at a 90-degree angle. Drop your hips to the ground. It is ideal to have your front knee just above your ankle and your back knee pointed toward the ground but not contacting it. As you take a firm stride into an opposite-side lunge, pull your right leg forward with your right foot and press your left heel into the ground. That’s one rep.
lateral lunge With Bicep Curl
lateral-lunge-with-biceps-curl
How to conduct: With your hands facing inward and your feet together, start standing. Maintain a dumbbell in front of your shoulders. Point the toes and heel of your left foot forward as you sidestep. Holding dumbbells, stretch your left leg to the floor on both sides. Your back should stay flat, and your abs should continue to be firm.
Curl the dumbbells up to your shoulders, plant your left foot close to your right, then push off your left foot to stand back up. That’s one rep.
Barbell deadlift
barbell deadlift
The deadlift is the most effective compound exercise you can do because it involves lifting the largest weight. That should be your strongest lift without a doubt.
One of our favorite barbell exercises, the deadlift, can help build stronger, larger muscles in both the upper and lower body. The quadriceps, glutes, hamstrings, and back are the primary muscles used, even though the entire posterior chain is covered. Naturally, grip strength and bone strength are developed as a result of having to hold onto the barbell.
Deadlifts, like squats, will enhance anabolic hormones. Additionally, deadlifts boost neurological strength, which is beneficial for harder upper and lower body exercises like barbell bench presses and squats. Your deadlift will get better with each pull, leading to stronger lifts all around. It is the strongest available booster. You should look into alternatives to deadlifting if you are unable to perform them for any reason (lower back pain during deadlifting is typical; this is a high-risk, high-reward sort of workout).
Steps to Take: If your shins do not come into touch with the bar, they should. Stretch your back from the waist after placing your buttocks on the bars on either side of your legs. Make an overhand hold with both hands. Remember to keep your hips and shoulders aligned. Put pressure on your shoulder blades to release tension from the bar and straighten your spine. As the weight is increased, keep your grip on the bar tight. Tighten your glutes such that your knees, hips, and shoulders are stacked on top of each other.
Repetition and Sets: Start with six to eight repetitions in three to six sets.
Barbell benchpress
barbell-bench-press
This is the most effective upper-body workout and the best compound lift for the chest.
Your chest will get stronger and more muscular if you press horizontally, as in the barbell bench press. Given that the chest is one of the strongest muscular regions in the body, this is unquestionably the best lift you can get for the money.
You will be able to shift your chest in different ways as you push your arms straight and then drop them down. Your posture and back strength will increase, your chest will get stronger and longer, and muscle growth will be encouraged. The bench press engages multiple muscle groups in addition to its primary one. Your quadriceps, lats, and anterior deltoids will all get stronger as a result. It also strengthens your core. The amount of stimulus your muscles experience during a bench press is also influenced by your grip.
How to do bench press: Sitting on the bench, make sure your feet are level with the floor. Pull your belly button back toward your spine to keep your glutes and core strong. To begin, set a barbell or dumbbell directly above your shoulders. Breathe deeply and keep your forearms parallel to the floor by bending your elbows as you lower yourself.
Exhale and push yourself up. Sets & reps: Begin with three sets of eight to twelve reps.
Dumbbell bench press
dumbbell-bench-press
How to conduct: Return to the bench and press each dumbbell against your thighs with one hand. Hold the dumbbells shoulder-width apart over your chest, keeping your forearms and upper arms at a 90-degree angle. The hands should face forward. Exhale as you bring the dumbbells up to arm’s length. Please wait a moment. That’s one rep. Do ten repetitions twice a day.
Dumbbell military press
Dumbbell-military-press
Strength and powerlifters employ this last Big Four compound workout. This additional workout allows you to perform heavy weightlifting at your one-rep maximum.
The military push is an intense vertical pressing exercise that tones your shoulders. It’s one of the most challenging exercises you’ll ever do, and it includes the finest compound raise for the arms.
It tones your biceps, lats, upper chest, and triceps in addition to building shoulder strength and mass. It also works wonders for strengthening the glutes and abdomen because when pushing hard pressure past the head from a standing position, these muscles must work extremely hard to maintain stability.
The military press should only be able to function when people are seated.
This is a crucial workout for athletes since it generates a lot of early power and strength. You’ll be able to exert pressure without having to accelerate first. The military press can be thought of as a reverse deadlift. It exercises the entire body. Additionally, the military press works every muscle that the deadlift fails to reach. The military press, along with the barbell squat, deadlift, and bench press, is one of the hardest exercises for building muscle and strength. The four exercises listed above are sufficient for powerlifters, but extra compound workouts are needed for individuals who want to address hypertrophy and strength training more thoroughly.
How to conduct: After consuming your meal on an elevated bench, raise some dumbbells. Verify that the back of the bench is 90 degrees angled. Once seated, place a dumbbell on each leg. Try to keep your back and shoulders as straight as possible. Dumbbells should be raised to shoulder height after being lifted off your thighs. Raising each thigh independently will help you handle hefty weights. Lifting a hefty dumbbell with just your arm could cause an injury. If that is how you want to execute a dumbbell press, you can also do it with your hands facing your body.
Dumbbells should be pressed above the head until the arms reach their maximum length. After a few seconds of holding the dumbbells above your head, bring them down to shoulder height. Execute the required quantity of iterations. Do one set of eight to ten repetitions if you’re just getting started. After eating on a raised bench, pull up some dumbbells. Verify that the back of the bench is 90 degrees angled.
How to conduct: Pick up some dumbbells after eating on an elevated bench. Confirm that the bench’s back is at a 90-degree angle. Once seated, place a dumbbell on each leg. As you sit, make sure your lower back is firmly placed against the back of the bench. Try an effort to keep a straight back and shoulders. Dumbbells should be raised to shoulder height after being lifted off your thighs. Raise each thigh separately to aid in the carrying of large weights. Lifting a hefty dumbbell with just your arm could cause an injury. If that is how you want to execute a dumbbell press, you can also do it with your hands facing your body. Be sure the ground is at the same height as your forearms. Pressing dumbbells above the head will cause the arms to fully expand. After a few seconds of holding the dumbbells above your head, lower them to shoulder height. Execute the required quantity of iterations.
Pull-up
Pull-Up
Pull-ups are essential for anyone who works a full-time job, is a bodybuilder, powerlifter, weightlifter, cross-fitter, or does anything else. Pull-ups are fundamentally an important piece of the puzzle that powerlifters frequently ignore because their results don’t directly translate into overall strength. A pull-up is a test of your relative strength, or your ability to raise your body weight. If you find that you are unable to perform pull-ups, try our pull-up progression program.
Because pull-ups primarily target the lats and biceps, two muscular groups that have not historically been the primary focus of training, they are vital. Pull-ups not only target these muscles, but they also function best when done in specific forms, like chin-ups and neutral-grip pull-ups. Furthermore, similar to all of our other important complex workouts, pull-ups work more than just two muscle groups. Pull-ups will help strengthen your traps, rhomboids, deltoids, and core. Therefore, the following time you exercise,
Make sure you reach the pull-up bar. Since you are using your full body mass to raise the weights, your biceps may lift more weight than you should be able to with a barbell. Make sure your biceps are the center of attention by bringing your shoulder blades down and tightening your core muscles.
Coach’s Suggestion: Just picture tucking your elbows, just a little, into your back pockets. Reps & Sets: Repeat three or five times.
Barbell bent over row
The bent-over barbell row works your posterior in a similar way to how the bench press works your front upper body. Rowing is one of the fundamental motions, similar to pressing.
Your rhomboids, teres major, teres minor, rear delt, infraspinatus, lats, and the muscles between your shoulder blades will all gain strength and size from a bent-over barbell row. Your forearms are also needed for grip strength because it’s a pulling motion, and your biceps will be employed to propel the activity. When performed in reverse order, the bench press and a bent-over barbell row provide the equilibrium needed for both strength and good posture. Not to mention the appealing design.
Why isn’t one of the top compound exercises for powerlifting on the list, you might wonder? Despite being one of the best compound activities for the back muscles, the bent-over row is rarely used in powerlifting regimens because of process breakdown. Reaching a real 1 rep maximum in rowing without cheating or sacrificing form is quite challenging. Bending over the row would be pointless if you restricted your range of motion, stood up with the bar while pulling, or simply use your momentum and quick motions.
The lift-up is obtained from the starting position in each scenario. Even if there might still be a few little form issues, cheating is practically impossible. All things considered, the fundamental goal of powerlifting is pure strength, and perfect technique might be difficult to maintain during training. Rows are therefore merely support exercises used to enhance deadlifts, which are the actual back movements in a powerlifting program.
Exercise tip: The bent-over row is a better option than a deadlift because it targets the mid-upper back more specifically and allows for a wider range of motion. Additionally, it’s a very important lift for building back muscles, and different variations of bent-over rows can also be helpful.
Why it rocks: By strengthening your back with this upper-body dumbbell workout, you can lift larger weights than you could have with earlier programs.
How to conduct: Stretch your arms out to the sides while keeping your feet shoulder-width apart, holding a dumbbell in each hand. Bend forward at the hips and press your gluteal area rearward while keeping your core stable. should refrain from flexing their knees and twisting their shoulders. Your hamstring and hip range of motion determine how much you can bend over. Make sure your neck is in the right position by checking the ground a few inches in front of your feet.
During the hardest part of the exercise, squeeze your shoulder blades and push your elbows toward your body. One rep is awarded for this. Perform 10 rounds twice a day.
This classic dumbbell back exercise increases the size of your stabilizing core muscles by working your lats, rhomboids, and biceps. When added to any program that asks for more push-pull or back exercises, it’s a great supplement.
Reps and sets: three eight-to-ten-rep sets
Lowercase row
Lowercase row
How to conduct: Maintain a hip-width distance between your strides while holding a dumbbell at your sides. To maintain your core taut, flex forward at the hips and push back on your buttocks. Refrain from moving your shoulders when flexing your legs. Your hip range of motion and hamstring flexibility will determine how much bend you can get.
Look a few inches ahead of your feet to maintain a comfortable neck position. For a row, you should form properly by raising the weights to your chest. Make sure your elbows are out past your back as you raise the weight to your chest. Raise your arms to the floor softly as you progressively decrease the weights. One rep is involved. Perform 10 rounds twice a day.
Compared to the regular row, this rowing variant engages your lattisimus dorsi and biceps more.
Alternate bent-over row
alternative-bent-over-row
Why it rocks: Compared to other upper-body dumbbell routines, this workout makes use of your body’s strong back, which enables you to lift more weight.
What it does: This exercise targets your mid-to-lower traps, back deltoids, and lats.
How to conduct: Take a dumbbell in each hand and turn it inside out to assist oneself up. Bend forward with your legs slightly bent, keeping your body at or near floor level. Your abdominal muscles would tighten as you pushed your gluteal area back and lowered your chest.
To start the workout, pull your shoulder blades back, put your elbows behind your torso, and exhale. The correct position is to point your thumb toward your ribcage. Once your elbows are nearly parallel to your torso, you should begin moving the dumbbells in that direction.
finishing each set with 10 to 15 repetitions.
Barbell hip thrusts
barbell-hip-thrust
For individuals who believe that squats and deadlifts aren’t giving their glutes enough attention or who just desire a nice, muscular body, the barbell hip thrust is one of the best exercises for building glute mass.
It also improves deadlifts and squats, not replaces them, which is another important advantage. Exercises like deadlifts and squats demand a vertical hip hinge, but this one requires a horizontal one. A targeted exercise program is necessary for general hypertrophy since your gluteal muscles. Your hamstring and gluteal muscles are mostly employed because it’s a hip-hinging movement.
The barbell hip thrust is very good for your glutes since it provides the maximum amount of contraction stress. There’s not a similar exercise. One disadvantage of the barbell hip thrust is that it does not provide much stretching stress. As such, the squat is superior for tension during stretching, even if it is superior for tension during contraction. This makes each of these exercises equally crucial and advantageous for the glutes. This is a helpful cue to fully tighten your glutes when performing back squats.
If you are unable or unable to execute barbell hip thrusts, think about these alternatives.
How to conduct: If you are unable to perform barbell hip thrusts or simply do not want to, think about these alternatives. Towels or shoulder cushions are optionally placed on the bar for comfort. Once the barbell is exactly over your hip joints, move it back and forth across your thighs. Apply an inner brace. Once your knees and hips are parallel to one another, plant your heels firmly on the ground and utilize your glutes to raise your hips to full extension. return to the floor, but cautiously. That’s one rep.
Instead of tilting upward, your neck should be level with your body.
Push-ups
Pushup
why: the pushup is a popular bodyweight exercise that works much more than simply the chest. According to Sung, anyone can include the workout in their schedule since it is so versatile. Additionally, there are several choices for different emphasis points.
Steps to Take: With your back straight, your wrists curled beneath your shoulders, and your palms flat on the floor, begin the high plank pose. Think about pressing your hands into the ground. Just beneath you, maintain a neutral neck position. Make a straight upward strike.
Reps and sets: 3–4 sets of 12–15 repetitions.
AB wheel
ab-wheel-rollout
why: This little gadget packs a powerful punch. If you have access to an ab wheel, don’t be afraid to utilize it. This workout targets almost every muscle in your body, including the shoulders, abs, and glutes.
Steps to Take: Begin on your knees, with your palms on the roller. Move your body as far away from the object as you can without causing strain on your back, much like you would if you were doing a plank. If your hips start to raise or overextend, you’ve gone too far. Make sure you move precisely and slowly.
Reps: Three to five sets of five repetitions
Kettlebell overhead press reverse lunge
kettlebell-reverse-lunge-with-overhead-press
How to conduct: Using your left hand, hold a five to twenty-pound dumbbell or kettlebell at shoulder height. To execute a reverse lunge, take a step back with your left leg and then stand back up. Raise the kettlebell above your head while maintaining a small bend in your elbow once you are upright. Retain your arm near your head instead of allowing it to swing widely. To bring the left arm back to its initial position, lower it. That’s one rep. Do ten repetitions twice a day.
Knee Drive Deadlift
deadlift-with-knee-drive
You can do this workout without any weights if you’re a novice. Get a set of dumbbells out for harder workouts.
How to conduct: Hold the dumbbell in both hands and raise it. By bending at the hips and keeping your spine neutral and your core active, you may push them backward. Do not point your toes; instead, keep your left foot flexed and your left knee pointed downward. As you maintain your hip bend, your back and the bottom of your leg should be parallel to the floor.
Your left foot should still naturally dorsiflex. Maintain a straight posture with a solid core throughout the workout. That is comparable to one repetition.
Hex Bar deadlift
hex-bar-deadlift
Select the weight that you wish to give the hex bar. If this is your first time doing this exercise, begin with simply the bar and no weight added. How to conduct: Place yourself in the center of the hex bar with your hips separated from one another. Maintaining your legs level, raise your hips a little to tighten your hamstrings and back.
To stand tall with your shoulders flat and your back relaxed, press your heels into the ground. To ensure full hip extension at the end of the practice, engage your glutes. Hold on to the grips as you gently lower the weight to the ground. You should have an open chest and a flat back. This counts as a solo effort. Make eight to ten attempts twice every day.
Bulgarian Split Squat
Bulgarian-split-squat
If you’ve never used this approach previously, simply use your body weight. If you’re more experienced, acquire a 10-pound pair of dumbbells. Straighten your right leg while placing the toes of your left foot on a chair, box, bench, or stairway. As before, the knee rests precisely above the ankle. Bend your right knee and tighten your left glute while lowering your pelvis as low as possible to the floor or until the front of your thigh is level. with the floor. That’s one rep.
Slider knee tuck with Push-Up
slider-knee-tuck-with-push-ups
How to conduct: Start by placing a slider beneath each foot and assuming the plank posture. If you don’t have sliders, you can use a cloth and a hard surface to complete this exercise. Return to your previous location. Proceed to do a push-up. With every action, your back should stay neutral as your abdominal muscles contract. That’s one rep. Make eight or ten attempts twice a day.
Burpee squats press
burpee-squat-press
How to conduct: To begin, stand up and grasp a 10-kilogram dumbbell on either side of your torso. If you notice that this is too heavy and your form is improper, use less weight. Perform a burpee while lowering yourself while gripping the dumbbells. If you believe this workout is too strenuous on your hands or wrists, you can place dumbbells in front of you. A newbie may do a simple burpee.
Elevate your body off the ground and cautiously raise the dumbbells. Aim for a neutral spine and an active core before pushing yourself off the ground. Maintaining a tall stance and a clenched stomach, bend your arms, place the dumbbells on or just above your shoulders, and then drop yourself into a squat. Standing, raise both dumbbells above your heads. That amounts to one rep. Twice a day, make eight or ten attempts.
Arnold Press
Arnold-press
Bend your arms 90 degrees and place dumbbells in front of your face to begin. Lift the weights straight and extend your arms as far as they will go. You can start afresh by reversing the movement entirely. That’s one rep. Make eight or ten attempts twice a day.
Upright Row and deadlift
upright-row-and-deadlift
How to conduct: Place your knees hip-width apart and bend them slightly as you stand. Extend your hips, contract your core, and descend the weights down your shins while keeping your spine neutral. Rise to your feet gradually. Until you reach the top, raise your arms to your chest while maintaining your elbows out to the sides. That amounts to one rep. Perform 10 rounds twice a day.
Squat, curl, and press
squat-curl-press
How to conduct: Position your feet directly beneath your hips and grasp a dumbbell in each hand. Squat until your thighs are parallel to the floor to get back into a sitting position, being careful not to allow your knees cross your toes. Once you have brought the weights to your shoulders, perform a bicep curl after lifting with your heels to stand back up.
Goblet Squat
goblet-squat
How to conduct: When standing, spread your feet wider than shoulder-width apart and tilt your toes slightly outward. Lower your entire body until your thighs are perpendicular to the floor while maintaining an active core. This asks you to push your hips back and bend your knees.
As you rise to the starting position, ensure that your heels are supporting the proper amount of weight. Do two sets of 10 repetitions to finish one rep. The relevant muscle is that:gluteus medius, gluteus minimus, gluteus maximus, vastus lateralis, vastus medialis, and vastus intermedialis, as well as the rectus femoris.
Reverse lunge with one leg raise
Reverse lunge with one leg raise
How to conduct: Stand with your feet shoulder-width apart and contract your core. Reposition your right foot so that the heel touches the sole and leaves the ground. Lower yourself into a lunge by flexing both knees at a ninety-degree angle. Raise your right arm forward while bending your elbows with your left arm slightly out behind. Maintain an inner curvature of your hips; do not try to extend your buttocks using your related abdominal muscles.
With your left foot, bring your right knee to your chest, then hop as high as you can. After landing softly in the typical posture on your left foot, move to enable you to execute another lunge. One rep consists of ten executions. Complete every repeat on a single side. After that, reverse lunge and switch sides to get back to the single-leg hop.
Benefits of compound exercises
Although some unskilled fitness enthusiasts might think that doing isolated exercises is enough to build muscle and strength, this is not a smart approach for every muscle group. The first step in any successful fitness program is to incorporate compound exercises, or routines that enhance foundational activities. This affects even the most skilled weightlifters and sportsmen.
Even if isolation exercises are easier and less strenuous, compound lifting is more suitable for healthy beginners. Compound lifts remain the greatest option, although isolation exercises can be helpful for athletes with a strong foundation in strength and bulk.
Train many muscle groups simultaneously: The essential point is not that training becomes more effective when difficult lifts or compound workouts are performed. Working out many muscle groups simultaneously and using heavier weights might help you gain more muscle mass and improve your overall strength. Gaining muscle bulk and power is substantially easier with most complex activities. Compound lifting is the greatest way to define functional fitness.
Greater Ease in Gradual Overload: Compared to isolation workouts, compound strength exercises enable you to increase the weight much more quickly, so you may notice a faster improvement in your muscles whether you are a rookie or even an expert lifter! Compound lifts have a significantly higher ceiling.
Boost Growth Hormone and Testosterone: Compound lifts produce noticeably higher quantities of these two anabolic hormones than single sessions do. Their ability to grow muscle is further enhanced by that element.
Stronger, Denser Bones: You may strengthen your bones and muscles at the same time by lifting heavier weights. You develop whole-body strength in this way.
Enhances Intermuscular Coordination: In compound workouts, you can teach your muscles and joints to function as a single unit instead of as a robot by employing more advanced lifting techniques. They both produce and control force together. This will greatly improve your movement efficiency, balance, and coordination. This is particularly helpful if you wish to improve as an athlete. Even if you’re not interested in sports, compound workouts are helpful movements that help you become ready for life in the real world, which is something we all experience.
Increase Calorie Burn: Because compound workouts require a greater range of motion and a larger net energy expenditure than isolated exercises, they burn more calories. The best course of action is to complicated workouts if you value reducing weight. Moreover, having more muscular mass will increase your resting metabolic rate. That is a fat-burning double punch.
Enhances Flexibility and Mobility: A lot of people don’t know that compound lifts are actually a type of dynamic stretching. Stretching and contracting your muscles with each repetition of compound movements that require a wide range of motion can help you increase joint mobility and flexibility. Check your mobility.
Boost Your Muscle and Strength: Because numerous muscle groups work together to accomplish the exercise, you may load complicated motions with more weight than you would when isolating a single muscle. A reliable way to gain strength is to apply the progressive overload principle, which forces your muscles to grow and adapt in response to increased tension. You’ll be able to use larger motions to challenge the muscles more.
Effectiveness: Compound exercises target many muscle groups at once, so you may train your complete body with fewer exercises than an exercise program that just consists of isolation exercises. While the hamstrings and glutes are used to generate hip extension, making a deadlift predominantly a lower-body workout, your back muscles are also critical for load stabilization as you draw from the floor. Your pectoral and triceps muscles cooperate to push the weight over your head during the bench press exercise. Your pecs adduct as your triceps extend your elbows. Additionally, you will burn more calories when you use all of these muscle groups at once. All things considered, you will get more value out of your money with these workouts.
Solidity: Because compound motions require you to use multiple joints simultaneously, stability is essential to good performance. Our smaller stabilizing muscles will contract to keep our joints moving in the desired direction while our bigger muscles generate the force for the movement. Increased neuromuscular coordination and a high degree of stability are almost always required for compound exercises.
Energy: If you’ve ever been weary after completing a set of front squats, don’t confuse this feeling with being out of shape. You will use a lot more energy when executing a set of complex exercises as opposed to individual workouts. Their cardiovascular systems are stronger in them.
Exercises such as lunges, deadlifts, and squats put a great deal of strain on the neural system. The central nervous system will also be strongly activated during complex workouts. When you implement these significant changes, you will experience this type of tiredness, thus you must approach them from a different angle.
Maximal Hypertrophy: By targeting big muscle groups, compound lifts increase total strength and muscle growth.
Saving Time: Complex lifts are a faster way to finish your exercise than isolating particular muscles. They target many muscle groups simultaneously, enabling you to do more.
The common mistakes occur during compound exercises
Compound Exercises Cannot Be Done in One Size That Fits All
Not every advanced exercise is appropriate for everyone. Despite being one of the most popular exercises in programming, the barbell back squat might not be a suitable fit for your body type and level of experience. You could not benefit from common workouts if you have restricted movement, an anatomy that makes some motions difficult, or a history of injuries. Fortunately, there are alternative ways to get your complex lifts in, including moving the weights or rearranging the equipment.
Don’t Go Overboard
If someone is new to strength training, it may take some time for them to establish a baseline for how an exercise should feel. This is because inexperienced lifters lack the muscle endurance and stability necessary to maintain a proper form throughout a lift. Correctly adjust the weight, sets, and repetitions. You may be used to watching fitness enthusiasts and sportsmen do maximum barbell squats and deadlifts, even when they are not required to. Many eventually had terrible first failures. They also don’t have the patience or understanding of how draining failing may be. While it’s acceptable to give yourself a quick rep at first, you should make the most of each rep to build that foundation over time.
Don’t Underperform
Beyond just not lifting large weights, a typical error made by many is not pushing oneself on more challenging compound exercises. There are various ways to increase the difficulty of compound exercises without adding additional plates, such as by slowing down the eccentric part of a workout or adding pause reps. These workouts will help you build muscle and strength since they will prevent you from performing the same sets and repetitions with the same weight.
Safety
If you have any issues regarding the proper technique for doing a complex exercise, speak with a physiotherapist or other fitness professional at your club. They can illustrate the appropriate way to avoid getting hurt. For the fitness routine, they can provide a safe workout schedule. Compound exercises, like deadlifts, require certain techniques to keep you safe and avoid injury.
Work with a trainer or fitness specialist before performing these exercises, particularly if you haven’t done the move previously. They can observe you to make sure you’re taking the right strategy. You may eventually be able to safely complete the tasks on your own. Still, working out with a partner who can see you is a wonderful idea.
If you’re new, consult a trainer or other fitness specialist at your gym. They can help you figure out what the right beginning weights should be. Starting with a lightweight that you can comfortably perform 10 to 15 repetitions within a set is a decent general rule of thumb.
Increase the weight for the second and third sets if it seems steady and comfortable for you. You should feel burned out during the last few repetitions, but you should never waver. In between sets, stop the workout and sip some water if you feel lightheaded, exhausted, or ill.
Conclusion
Compound exercises are a great method to get the most out of your gym sessions. Try to vary your routine and include some new complex workouts every few weeks.
Because of the diversity, you’ll be able to engage more muscle groups and prevent frustration and plateauing. Ask a trainer or other fitness specialist at your club if you have any questions about how to do a complex exercise correctly. They can illustrate the appropriate way to avoid getting hurt. See your doctor before starting a new exercise regimen; they should provide a safe program plan for your level of fitness.
Your program’s core consists of compound lift exercises. These workouts will correctly train and overexert your major muscle groups. Your overall strength and size increase come from them. The more isolated exercises are meant to help you target specific muscles or portions of muscles that need more attention. They are there to help you with your overall look, inconsistent strength, and weak muscles.
FAQs
Why Use Compound Exercises?
If you want to improve your overall strength and have a productive workout, an exercise regimen that mostly consists of compound motions might help you achieve the required outcomes. If your aims or requirements are more specific, separation is often more suitable. A very effective strategy can involve combining isolation exercises to target different muscle groups as the top layer of training and complex motions as the basis.
What is a compound workout?
Many muscle groups cooperate to execute a movement in a complex exercise, such as the dumbbell shoulder press exercise. This exercise simultaneously works the pectoralis major, deltoids, abdominals, and triceps brachii. Compound exercises and isolated exercises are not interchangeable. These focus on a single muscle group at a time.
Which five compound workouts are the golden ones?
The five movements that make up the Big 5 of strength training are the pull-up, shoulder press, squat, bench press, and deadlift.
Can we perform complex workouts every day?
If you’re a healthy adult, you should be able to conduct strenuous workouts two or three times per week. Focus on distinct muscle groups every day. Between strength training sessions, give your muscles at least 48 hours to heal.
Should Someone perform every compound workout?
If you want a full, productive, and practical workout, devote the majority of your training time to compound exercises. However, there are situations in which it is both required and advised to isolate a particular muscle, muscle group, or joint.
Does one lift per day be sufficient?
This program might be somewhat boring at times because of the lack of diversity and variation in the exercises, but it works wonders for gaining muscle. Powerlifters might also gain by performing one exercise every day because their main goal is to be the strongest in the three major lifts: the deadlift, bench press, and squat.
References:
Mandaliya, D. (2023, December 13). Compound Exercises – The Best Way to Build Muscle and Burn Fat. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/compound-exercises/
Chertoff, J. (2019, November 13). How to Add Compound Exercises to Your Workout Routine. Healthline. https://www.healthline.com/health/fitness-exercise/compound-exercises
Icohen, & Broser, E. (2020b, August 25). The 10 Best Compound Exercises for Strength. Muscle & Fitness. https://www.muscleandfitness.com/workouts/full-body-exercises/top-10-compound-lifts-maximum-size-and-strength/
Perthes disease is a rare childhood condition affecting the hip joint, specifically the femoral head, which is the rounded end of the thigh bone. It occurs when the blood supply to this part of the bone is temporarily disrupted, causing the bone tissue to die, a process known as avascular necrosis.
Perthes is actually a multi-stage, intricate process that might take years to fully develop, even though the word “disease” is still often used. The femur’s head gradually regains its blood supply, and the bone starts to regenerate.
The goal of Perthes treatment is to encourage the bone to reshape into a more rounded form that yet allows it to fit into the hip joint’s socket. By doing this, hip issues in adulthood can be avoided and the hip joint can move more naturally. In most circumstances, children with Perthes have an excellent long-term prognosis. Most youngsters return to their regular activities without significant limits after receiving therapy for 18 months to 2 years.
The illness affects kids between the ages of two and fourteen. Both early osteoarthritis and lifelong deformity may result from the illness. Though it affects males five times more frequently than girls, it is most likely to cause more serious bone injury in the former. 10% to 15% of instances involve damage to both hips.
The dead bone starts to be removed by new blood vessels as the healing process progresses.
As a result, the femoral head becomes weaker and bone mass decreases. As new bone and tissue replace the necrotic bone, it may also result in bone deformities.
The ball experiences a fracture of the supporting bone as bone death manifests. This fracture marks the beginning of the body’s reabsorption of bone.
Pathology
The femoral head weakens and bone mass is lost as a result of new blood vessels penetrating the dead bone and eliminating the necrotic bone over time.
Adults who have osteoarthritis are more likely to have a persistent malformation of the femoral head as a result of Perthes.
Causes of Perthes disease
Although LCPD is an idiopathic condition, since its discovery more than a century ago, several ideas on its underlying causes from congenital to environmental, from traumatic to socioeconomic have been put up. Abnormal bone development patterns, fibrinolysis, and thrombosis have all been linked to LCPD.
Additionally, it’s linked to anomalies in the Insulin-like Growth Factor-1 Pathway, recurrent microtrauma, mechanical overloading caused by the child’s hyperactivity, extremely low birth weight, or short stature at birth.
A type II collagen mutation is one genetic cause that some research proposes, whereas other studies indicate mother smoking during pregnancy along with other prenatal and postnatal risk factors.
It’s possible that any or all of the previously listed reasons are necessary for LCPD.
Clinical Features of Perthes Disease
Limp: These youngsters usually have a psoatic limp as a result of psoas major weakening. The limp gets worse during physical activity and gets better after taking breaks. Late in the day, after extended walking, the limp becomes more apparent.
Pain: During the acute phases, the kid frequently experiences pain. Usually, the pain gets worse later in the day and when one is more active. Pains during the night are common.
ROM: The child’s active ranges of motion in abduction and extension will be reduced.
Unusual high activity level: Children with LCPD typically exhibit high levels of physical activity, and a notable proportion of them suffer from attention deficit disorder or real hyperactivity.
Abnormal growth patterns: In relation to the upper arm, the hands and forearms are comparatively short. In relation to the tibia, the feet are rather short.
Stages of Perthes disease
Early in the 20th century, Waldenström divided the progression of LCPD into four stages. Joseph et al. then further divided each of the first three stages into early (A) and late (B) substages to further categorize the disease’s evolution and pinpoint specific changes that occurred at different points.
Stage I: Initial stage or avascular necrosis (± 1 year)
IA: Early
Head of the femur radiolucency.
IB: Late
flattening of the femoral head’s summit
IIA: Early
There is early fragmentation.
IIB: Late
There is more fragmentation when a dead bone is resorbed.
The femoral head has an uneven contour and seems more flattened.
might seem to subluxate.
Reossification stage III (two to three years)
IIIA: Early
Along the femoral head’s outside perimeter, new porous bone grows.
Increases in density IIIB: Late
Towards the center, the freshly produced bone progressively fills up.
The femoral head’s contours and form become more distinct.
Stage IV: Healed
The final shape (the extent of flattening or deformity) and fit of the femoral head into the socket at this point largely dictate the long-term outcome.
Diagnosis of Perthes disease
MRIs are typically ordered to confirm the diagnosis, however, x-rays can also be used to see where the femoral head is positioned.
An imaging method that can forecast the outcome in the early stage of the illness, before considerable deformity has arisen, is preferable because the outcome of LCPD is varied.
At the early stages of LCPD, there was no association between the degree of femoral head involvement seen by non-contrast and contrast MRI, suggesting that they are evaluating two distinct aspects of the disease process. Contrast MRI gave a more accurate picture of the affected region during the early stages of LCPD.
Novel three-dimensional (3D) magnetic resonance imaging (MRI) reconstruction and volume-based analysis can be utilized to measure femoral head deformity in individuals with LCPD.
The femoral head distortion in LCPD may be accurately quantified and modest alterations (less than 10 percent) can be shown using the 3D MRI volume ratio approach. This technique might be helpful in assessing how a therapy affects the morphology of the femur head.
Treatment
Medical Treatment of Perthes Disease
The treatment plan is a contentious one. The prognosis for the condition must be clearly understood before determining if surgery is required.
Psychological aspects are also taken into account. Compared to their counterparts, those with a history of LCPD had a 1.5-fold increased risk of developing attention deficit problems.
Physical therapy management of Perthes disease
Regarding the potential advantages of physical therapy for individuals with learning disabilities or the optimal stage at which to use it, there is a lack of agreement.
While some studies discuss physical therapy as a pre-and/or postoperative intervention, others view it as a conservative measure used in conjunction with other therapies including plaster casts, orthoses, and skeletal traction.
Children with a mild course of the condition received physical therapy in trials comparing various therapies. The following were the patients’ characteristics:
Children in Caterall groups 1 or 2 who have less than 50% femoral head necrosis
Children under six years old with excellent (>80%) femoral head covering but more than 50% femoral head necrosis
Herring class A or B
Type A Salter Thompson
Physical therapy can enhance muscle strength, articular dysfunction, and articular range of motion in people with mild cases. Among the physical therapeutic interventions were passive mobilizations to extend the hip’s muscle.
Exercises including straight leg raises are useful for strengthening the hip muscles involved in flexion, extension, abduction, and adduction.
After eight sessions, they moved on to isotonic exercises from isometric ones.
Conservative management of Perthes diseases:
Active Assisted Hip Knee Flexion
It has been demonstrated that physical therapy therapies increase this patient population’s strength and range of motion.
Compared to people who get either a home exercise program or no training at all, individuals who engage in supervised clinic visits show better progress in muscular strength, functional mobility, gait speed, and quality of exercise performance.
People who get encouraging comments from their physical therapist on a daily basis are more likely to stick with an additional at-home exercise regimen.
Improve ROM in Perthes disease:
Moving ROM
To preserve a newly achieved range of motion, do AROM and AAROM (active assistive range of motion) after passive stretching.
Increase your strength
Start with isometric exercise, work your way up to isotonic activities in a posture that lessens your gravity, and then go on to isotonic workouts that defy gravity. Both concentric and eccentric contractions are acceptable.
Start each exercise with two sets of ten to fifteen repetitions, then proceed to three sets of the same exercise.
When a kid has LCPD, it is best to prevent the hip overloading pattern.
When LCPD first manifests between the ages of 6 and 8 with Herring B involvement, brace-based non-surgical therapy is a dependable substitute for surgical treatment. They were unable to determine, nevertheless, if the positive outcomes were due to the brace or to the patients’ favorable prognosis.
Post-operative management of Perthes disease
The many phases of rehabilitation are mentioned while describing the rehabilitation.
Initial Phase (0-2 weeks post-cast removal) Goals of the Initial Phase
After passive stretching, perform AAROM and AROM to keep the newly acquired ROM.
Boost your strength in the knee, ankle, and hip flexion, abduction, and extension.
Start with hip-level isometric exercises and work your way up to isotonic workouts while reducing your gravitational force.
Start with isometric workouts for the knee and ankle, then go on to isotonic exercises while reducing your gravitational force. Eventually, you can advance to isotonic exercises that defy gravity.
Start each exercise with two sets of ten to fifteen repetitions, then work your way up to three sets of each exercise.
improve functional mobility and gait
Observe the WB status.
ADL’s Gait training with the proper assistive device, emphasizing safety and independence, includes transfer training and bed mobility to optimize independence.
enhancing the integrity of the skin
If possible, a warm bath to restore skin integrity after cast removal in a home setting.
With your arms immersed, start slowly strolling in the chest-deep pool of water.
Enhancing the Integrity of the Skin
Continue massaging and desensitizing scars.
Swimming is allowed if the referring physician gives the okay.
Advanced Phase(6-12 weeks post-cast removal) :
Goals
Reduce pain (refer to “initial phase”)
Isotonic hip, knee, and ankle movements, involving concentric and eccentric contractions, performed in postures that reduce gravity and defy gravity
Start functional dynamic single-limb movements supported by the upper extremities (e.g. step-ups, side steps)
If your WB status permits, go to single-limb closed-chain exercises with minimal resistance after finishing double-limb closed-chain exercises with resistance.
Using a stationary bike while upright or reclined and maintaining a hip flexion angle of less than ninety degrees
Use a step-to-pattern to independently negotiate stairs while receiving upper extremity (UE) help.
Enhance balance to at least 69% of the maximum Pediatric Balance Score (39/56) or to the unaffected side’s single-limb stance.
enhancing functional mobility and gait.
FAQs
What are Perthes disease exercises?
Activities to improve balance and coordination. How to incorporate regular low-impact activities into your child’s routine, such as walking and stationary cycling.
Is Perthes illness inherited?
Sometimes mutations in the COL2A1 gene cause the characteristic bone abnormalities associated with Legg-Calvé-Perthes disease.
What should you stay away from when it comes to Perthes disease?
Runs, jumps, and other high-impact sports that might hasten hip deterioration should be avoided by kids with Perthes disease. crutches. Your youngster may occasionally need to refrain from putting weight on the injured hip.
Perthes disease affects which gender?
The majority of individuals with Legg-Calve-Perthes disease are men; the male to female ratio ranges from 4:1 to 5:1. Ten to twenty percent of afflicted instances are bilateral. Bilateral cases are typically asymmetrical and identified at separate phases of the illness.
For kids with Perthes disease, what kinds of activities are beneficial?
While riding and swimming are still permitted, the majority of doctors advise limiting some activities, such as impact sports like running and leaping. Physical therapy is occasionally advised to reduce muscular weakness and assist with stretching.
References
Physiotherapist, B. (2023c, December 13). Perthes Disease: Cause, Symptoms, Physiotherapy management. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/perthes-dieases-and-physiotherapy-management/#google_vignette
Legg-Calve-Perthes Disease. (2024, September 10). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/legg-calve-perthes-disease
Lead pipe rigidity is a type of muscle stiffness commonly associated with neurological disorders, particularly Parkinson’s disease. It refers to a uniform resistance to passive movement throughout the entire range of motion, resembling the resistance encountered when bending a lead pipe. This condition results from the hyperactivity of muscle tone, causing an inability to relax the muscles.
Unlike other types of rigidity, lead pipe rigidity is characterized by constant tension without fluctuations, making movement difficult and often leading to discomfort or stiffness for the individual affected.
What is Rigidity?
Rigidity, a common muscle tone problem characterized by resistance to passive movement regardless of posture and velocity, is frequently used by numerous authors as a synonym for hypertonia. The primary objective of the defining characteristics of Parkinson’s disease, it is commonly observed in extrapyramidal disorders. Both agonists and antagonists are equally impacted.
It can be observed in –
Parkinson’s Syndrome
Corticobasal Degeneration
Huntington’s Disease
Multiple System Atrophy
Stiff Man/limb Syndrome
Niemann-Pick Disease – Type A
Orthostatic Hypotonia Shy-Drager Disease
Spinocerebellar Ataxia – type 43, 17, 2
Definition:
Stable resistance across the range of motion characterizes rigidity, a hypertonic state independent of movement velocity. Inappropriate recruitment of upper motor neurons or supraspinal drive targets alpha motor neurons, while spinal reflex tools are typically normal. Typically, tendon jerks are normal in Parkinsonian stiffness.
When all of the following criteria are satisfied, hypertonia is referred to as “rigidity”:
An instantaneous resistance to reversing the direction of movement about a joint is indicative of simultaneous co-contraction of agonists and antagonists.
The limb does not have a propensity to revert to an excessive joint angle or a stable position.
even though rigidity may worsen, involuntary motions about the tight joints are not caused by voluntary activity in distant muscle groups.
Pathology of Lead Pipe Rigidity:
Resilience results from the excessive supraspinal drive (upper motor neuron facilitation) operating on alpha motor neurons, even though the mechanisms underpinning spinal reflexes are normally normal. The typical reciprocal inhibition is disturbed. Stiffness and involuntary movements, together with abnormalities of posture and associated movement, are symptoms and signs that arise when the balance between excitation and inhibition in the motor cortex and basal ganglia is upset. However, our current knowledge of the pathophysiology of the basal ganglia is insufficient to explain the two other hallmarks of Parkinson’s disease: rigidity and tremor.
Several factors can contribute to rigidity, some of them are as follows:
incapacity of the patient to unwind and stop muscular activity
exacerbated rigidity as a result of the muscles’ changed viscoelastic characteristics
aberrant agonist-antagonist muscle group co-activation
enhanced reflexes for stretching
reduced amounts of dopamine
Rigidity Types:
Different forms of stiffness have been noted in a range of medical situations. Among the prevalent kinds are:
Lead Pipe Rigidity: Lead pipe rigidity is a uniform, uniform resistance when a limb moves passively. It happens to come about by the untimely death of dopamine-producing neurons in the brain and is frequently associated with Parkinson’s disease.
Cogwheel Rigidity: The resistance experienced during passive movement is characterized by sporadic disruptions. It creates the impression of a succession of little catches or jerks, akin to the motion of a machine’s cogs. Cogwheel rigidity is another hallmark of Parkinson’s disease.
What Causes Rigidity?
Stress frequently causes muscles to become inflexible.
Polymyalgia rheumatica is a common condition that causes pain and stiffness in older persons.
weariness and weight loss that cannot be explained.
Reduced dopamine levels are considered to throw off the equilibrium between the muscles that contract and relax with each movement in those with Parkinsonism.
What exactly Rigidity Signs and symptoms Are There?
difficulty getting out of a chair or bed, turning in bed, and turning while walking.
Joint pain may be linked to rigidity.
The rigidity of cogwheels and lead pipes is different in the following ways:
Lead pipe stiffness is defined as a consistent resistance to motion over the entire range of motion.
The ability to resist changes in strength as the limb is moved through its range of motion is referred to be “cogwheel stiffness”.
The examination of Lead Pipe Rigidity:
The person conducting the examination should use one hand to hold the registered hand above the wrist and hold it there. He slowly rotates along the hand’s long axis while holding the fingers and palm with the other hand. The person being inspected will encounter resistance when moving if there is rigidity. The person conducting the examination will notice a pause or repeated catch throughout the movement if the cogwheel phenomenon is positive; if it persists without any interruption or change in velocity, it is lead-pipe rigidity.
Management of Rigidity:
Medical Care
When levodopa (L-Dopa) is taken in these various combinations to treat Parkinson’s disease, bradykinesia and rigidity are significantly decreased.
It has been demonstrated that deep brain stimulation in the globus pallidus and subthalamic nucleus improves rigidity.
Physiotherapy Intervention:
For most patients, reducing stiffness early in the session facilitates a more seamless course of treatment. Therefore, when movement therapy is administered during the “on” phase of a premedication cycle, the results are expected to be more long-lasting.
Relaxation methods such as slow, gentle rocking, trunk and limb rotation, and the benefits of yoga appear to be effective in lowering stiffness. Sitting or standing may be the greatest way for persons with Parkinson’s disease to relax because lying down may make them more rigid.
Because the proximal muscles are sometimes significantly more involved than the distal ones, a distal-to-proximal transition may help understand relaxation. Exercises with rhythm have been demonstrated to lessen stiffness. Using your hands or feet to make circles and clapping your hands are two examples.
To help relax stiff muscles, use a heating pad or hot compress to the afflicted area.
Stretching your tense muscle will help it relax.
avoiding demanding activities that could cause the muscles to stiffen up again.
Stretching and relaxation exercises:
It is also advised to perform exercises that incorporate soft rocking and slow, rhythmic rotation. movement transition from passive to active aided and active movement using a rhythmic initiation strategy.
whereas lying supine, cautiously turn your head from side to side. Rotate the lower trunk when hook laying.
Lay sideways and rotate your upper and lower trunks.
The exercises are designed to increase the range of motion in your lower limb joints, boost your strength and balance, and activate your legs’ natural tendency to repeat motion while you walk.
Exercises for Gait Training:
Walking on a treadmill.
Lifting your legs.
Sitting down.
Standing up.
Stepping over objects.
Home Treatments
Home remedies are usually effective in treating muscle stiffness brought on by minor injuries, strain, or overuse. These could include the following:
Apply a warm compress or heating pad to the affected area to assist relax tense muscles.
Steer clear of demanding tasks that can make your muscles tense up again.
promoting relaxation of the muscles via massage, yoga, or tai chi.
An overview
One particular kind of muscle rigidity seen in some neurological disorders, most notably Parkinson’s disease, is lead pipe rigidity. It is thought to be one of the main motor signs that set Parkinson’s disease apart from other movement disorders. Degeneration of dopamine-producing neurons in the substantia nigra, a part of the brain involved in motor control, causes this stiffness.
Lead pipe rigidity is typically diagnosed by a clinical examination and the observation of characteristic motor symptoms in patients with Parkinson’s disease or other neurological conditions. Lead pipe stiffness helps diagnose Parkinson’s disease along with other symptoms including bradykinesia (slowness of movement) and resting tremors.
Lead pipe rigidity in Parkinson’s disease is frequently treated with drugs that increase dopamine levels in the brain or mimic dopamine’s effects. These drugs help enhance a patient’s mobility and overall quality of life by lowering stiffness and other motor complaints.
FAQs
What is the stiffness of lead pipes?
Rigidity in lead pipes is defined as a continuous resistance to movement across the whole range of motion (ROM).
What pathology underlies the stiffness of lead pipes?
“Lead-pipe” rigidity is the neurological trait of impulsive muscle rigidity that remains constant even when existence is passively regulated. It is caused by harm to the basal ganglia. Numerous other neurological conditions, especially Parkinson’s disease, are linked to this.
How does the stiffness of lead pipes feel?
Muscle Rigidity: Cogwheel and Lead Pipe Rigidity Your muscles can feel tense, and you might have problems moving. Muscle spasms are another example of how they may unintentionally stiffen. This stiffness may also cause soreness in the muscles and joints.
What is the stiffness of lead pipes and cogwheels?
The maximum amount of deductions prevalent sign of Parkinson’s disease is this. The body no longer moves smoothly for extended periods, and the muscles become rigid. Lead-pipe rigidity happens when stiffness lasts, whereas cogwheel rigidity happens when muscle action becomes jerky. It is no longer possible to conduct immediate moves.
What is the symptom of rigidity?
When muscles lose their flexibility, they become rigid. This disorder, sometimes referred to as facial masking or Parkinson’s mask, affects the muscles in your face. It’s among the primary markers of Parkinson’s disease.
How can stiffness be increased?
Regular movement and activities throughout the day, such as clearing out a closet, hiking, strolling to the mailbox, yoga, dancing, cycling, or watering your plants, might help reduce stiffness.
References
Dr.RaviPatel. (2023, August 3). Lead Pipe Rigidity – Type, Treatment, Exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/lead-pipe-rigidity/
Physiotherapist, N. P.-. (2024a, July 4). Rigidity: Type, Cause, Symptoms, Treatment, Exercise. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/rigidity-physiotherapy-treatment/#Difference_Between_Spasticity_Rigidity
Plantar fasciitis is a common foot condition that causes heel pain at the bottom of the foot. It occurs when the plantar fascia—a thick band of tissue that runs along the sole—becomes inflamed or irritated. This tissue supports the arch of the foot and absorbs shock during movement.
Repeated strain or excessive stress can lead to small tears, resulting in inflammation and discomfort. Plantar fasciitis is often associated with long periods of standing, improper footwear, or activities like running. The pain is typically worse in the morning or after prolonged inactivity.
It causes pain in the heel and ball of the foot, which is often worse during the first few steps of the day or just after rest. Bending the foot and toes up towards the shin also often results in pain.
Anatomy of Plantar Fasciitis
It is a thick white band made up of collagen fibers that are stretched lengthwise. It splits into five distinct bands as it moves toward the toes, ending at the proximal phalanges, or the toe bones that are nearest to the foot. On each proximal phalanx, the deeper layer reaches to include the digital flexor tendons.
Three parts of Plantar Fascia:
The medial part
The central part
The lateral part
Between the comparatively thinner and less noticeable medial and lateral sections lies the biggest and thickest region, which is called the center part.
The plantar fascia of young adults is also connected to the tendinous extension of the lower leg muscles, known as the calf muscle, or the Achilles tendon. It attaches to the posterior surface of the heel bone (calcaneum) after passing behind the ankle.
These two anatomical components are not directly impacted by one another since they have different, specialized attachments on the heel bone. Nonetheless, the Achilles tendon is indirectly tightened by the upward movement of the toes. Plantar fasciitis, a painful inflammation of the plantar fascia, is treated using this link.
Pathophysiology
The medial process of the calcaneal tuberosity gives rise to the thick, fibrous band of connective tissue known as the plantar fascia. It inserts at each proximal phalange as it continues toward the forefoot.
According to current thought, microtears in the plantar fascia develop, indicating a structural breakdown that is not just the result of inflammation. People may be more susceptible to the illness due to the foot’s anatomical makeup.
Any structural irregularity to the foot might result in an asymmetric stress on the plantar fascia, which can cause chronic, recurring injury.
Causes of Plantar Fasciitis:
The most frequent cause of plantar fasciitis is an injury to the foot’s sole ligament from repetitive tension. Inadequate footwear, excessive running or walking, and landing injuries from leaping can all result in strain injuries.
Sign & Symptoms of Plantar Fasciitis:
severe heel pain
sneaky heel pain that typically appears right after getting out of bed and makes you want to walk on your toes at first
worse at the end of the day following extended standing and eased by walking Symptoms are frequently bilateral.
restricted ankle dorsiflexion owing to a tight Achilles tendon tenderness at the origin of abductor hallucis sensitivity to palpation at the medial tuberosity of the calcaneus pain with palpation rises
a tiny percentage of individuals with symptoms suggestive of irritation or entrapment of the first branch of the lateral plantar nerve (Baxter’s nerve).
Risk factors
Age: 40 to 60 years old
Certain types of exercise: Exercises that put a lot of strain on the heel and attached tissue, like long-distance running, ballistic jumping, ballet dancing, and aerobic dance, can cause plantar fasciitis to develop earlier.
Foot mechanics: A high arch, flat feet, or even an unusual gait style might change how your weight is distributed when standing and increase strain on your plantar fascia.
Obesity.
Occupations that keep you on your feet:- People in manufacturing, education, and other professions who spend most of their working hours on hard surfaces may suffer plantar fascia injury.
Differential Diagnosis:
Achilles tendonitis
Morton neuroma
Calcaneal stress fracture
Inflammatory arthropathy.
Diagnosis:
Radiographs
Although infracalcaneal spurring is more commonly an accidental finding and is not necessary for diagnosis, radiographs may reveal it.
When there are radiographic or clinical indications of rheumatoid arthritis, laboratory testing for rheumatoid factor is advised.
If there is any indication of a spondyloarthropathy (e.g., ankylosing spondylitis, Reiter disease), laboratory testing for HLA-B27 is advised.
If radiographs are not definitive in the diagnosis of stress fractures or if the patient is not improving with conservative therapy, technetium bone scans may be recommended.
When heel pain is resistant (pain persists for more than a year) or when soft tissue or osseous masses are palpable or visible in previous imaging examinations, an MRI is advised.
For the identical indications as MRI, ultrasound is a newer research that may be utilized instead. In patients with plantar fasciitis, ultrasound testing shows a thickness of the plantar fascia of at least 4 mm. Enthesopathy and hypoechogenicity have also been shown by ultrasound studies.
Treatment of Plantar Fascitis:
Medical Treatment
Pain relievers, primarily NSAIDs, such as Aleve (naproxen) and Advil or Motrin (ibuprofen), can help lessen the pain and swelling associated with plantar fasciitis.
Side effects: especially if used for an extended length of time. The most prevalent problems are related to the digestive system, such as nausea and heartburn. Hypertension, liver or renal damage, and allergic responses are less frequent but nevertheless dangerous adverse effects.
For severe pain and inflammation that do not improve with nonsteroidal medicine, cortisone injections are used for plantar fasciitis. adverse effect: The fat pad protecting the heel bone may decrease or the plantar fascia may tear as a result of repeated injections.
Surgical Treatment
As a last option, plantar fasciotomy is frequently used after six months of conservative therapy has not resolved the problem. There are endoscopic and less invasive methods for plantar fasciotomy, but they need to be performed by a professional with experience using specific equipment.
These surgical methods are not widely available at this time. According to a 2012 research, 76% of patients who had endoscopic plantar
Fasciotomy resulted in few complications and total symptom alleviation. There is no evidence that removing the heel spur during a plantar fasciotomy improves the surgical result.
There are several causes of plantar heel pain, and in certain situations, a lateral plantar nerve branch release may be carried out in addition to a plantar fasciotomy. Plantar fasciotomy may result in nerve damage, instability of the foot’s medial longitudinal arch, calcaneus fracture, extended recuperation period, infection, rupture of the plantar fascia, and inability to relieve pain. Recently, a different surgical strategy for treating plantar fasciitis that is resistant to therapy has been suggested: coagulation surgery.
Physical therapy Treatment
Ice is a quick and easy way to lessen pain and swelling. During the first phase, or if you feel that your injury is heated or hot, please apply for 20 to 30 minutes every two to four hours. You may use a frozen water bottle as an ice foot roller and get a little massage for your plantar fascia at the same time.
Shoe wear Modification (Running shoes): Running shoe modifications include a flared, sturdy heel to aid with heel stability management. The heel is softly cushioned and raised 12–15 mm above the sole. Achilles pad that is well-molded. Steer clear of stiff leather dress shoes since they put more strain on the Achilles tendon.
Viscoheels: Cushioned Heel Inserts for Plantar Fasciitis Treatment. Soft cushions are inserted and removed from the patient’s footwear. Eventually, patients with aberrant lower extremity biomechanics, such as pes cavus or pes planus, may find relief by wearing specially cushioned orthotics.
Taping for plantar fasciitis: Taping is another helpful pain-reduction method. By lowering the strain on your plantar fascia, this method lessens your pain. You will get immediate pain reduction after using this tape procedure.
Exercise of Plantar Fascitis:
Standing calf stretch:
Standing calf stretch
As though you were pigeon-toed, turn your rear foot slightly inward. Go back to where you were before. Do this three times. Perform this workout many times per day.
Seated plantar fascia stretch:
Seated plantar fascia stretch
Cross your wounded foot over your other leg’s knee while seated in a chair. Hold for 15 seconds, then do it three times.
Plantar fascia massage:
Cross your wounded foot over your other leg’s knee while seated in a chair. Massage the bottom of your foot with your other hand, working your way from the heel to the toes. Spend three to five minutes doing this. Begin slowly. As your tolerance for pressure increases, apply additional pressure to the bottom of your foot.
Achilles stretch
Achilles stretch:
On a stair, stand with one foot on the ball. Using your heel, reach toward the step below until your foot’s arch feels stretched. After 15 to 30 seconds of holding this position, release your tension. Do this three times.
Towel pickup:
Let go. Do this ten to twenty times. Once this becomes simple, place a book or small weight on the towel to increase the resistance.
Heel raise:
Heel Raises
Get up on your toes and hold for five seconds while using the chair or counter as support. Then, without clinging to the support, gently descend. (Retaining the assistance if necessary is OK.) Try doing this exercise while standing just on the affected leg if it starts to feel less uncomfortable. Do this fifteen times. Perform two sets of fifteen.
How to prevent Plantar Fascitis?
Rest: Take a break from your routine if you begin to experience foot pain.
Ice and elevation: To lessen swelling, it’s crucial to freeze your foot often and elevate it if you continue to perform activities that put weight on it, such as walking.
Don’t try to ignore the pain.
Avoid going barefoot.
Complications
Chronic heel pain that interferes with daily activities can be caused by ignoring plantar fasciitis. In order to prevent plantar fasciitis pain, which can result in issues with your feet, knees, hips, or back, you need probably alter the way you walk.
Prognosis
As soon as you begin treating your plantar fasciitis symptoms, you should see an improvement. However, it may take a few weeks to many months for your plantar fascia to recover.
Try your previous at-home remedies if you feel better but your symptoms come back. If your symptoms seem different or worse than they used to be, speak with your healthcare professional.
Conclusion
If you experience heel or foot pain that doesn’t go away after a week, consult a healthcare professional. They will assist you in locating at-home remedies to lessen your foot’s pain and swelling.
Being informed that you must miss a week or more of your favorite sport or hobby is always inconvenient. However, take your time returning to the court or field. If you overstress your foot before it heals, you might re-injure your plantar fascia.
FAQs
What is plantar fasciitis’ primary cause?
When the fascia, a thick band of tissue on the bottom of your foot, is overstretched or under severe strain from recurrent tension from activities like standing or jogging, plantar fasciitis develops. Significant weight gain, especially during pregnancy, may also result in it.
Is plantar fasciitis reversible?
With conservative therapy, which includes stretching, icing the affected region, and avoiding or reducing uncomfortable activities, the majority of patients with plantar fasciitis heal in a few months.
Does walking help people with plantar fasciitis?
Walking may actually exacerbate plantar fascia inflammation, necessitating a longer course of therapy. Although walking by itself won’t cause the ligament to worsen, choosing inappropriate footwear or overexerting oneself might cause plantar fasciitis to worsen.
How bad is plantar fasciitis?
In most cases, plantar fasciitis is treatable and not a chronic or permanent ailment. After a few months of conservative therapy, the majority of patients fully recover. Conservative treatment methods are effective in many plantar fasciitis instances.
How can someone who has plantar fasciitis sleep?
Avoid sleeping in a prone posture (face or belly down) if you have plantar fasciitis in order to avoid contracturing your calf muscle and Achilles tendon. Rather, choose to sleep on your side or back, with a cushion between your legs or beneath your knees, accordingly.
Is it natural for plantar fasciitis to heal?
The good news is that basic home remedies may typically be used to cure this ailment. Surgery is only recommended for around 5% of patients with plantar fasciitis, and only after conservative measures have failed.
How is plantar fasciitis massaged?
Pull each toe gently away from the foot, beginning with the big toe. Finally, give the heel a last circular massage.
Can someone with plantar fasciitis lead a normal life?
You frequently feel pain after working out, but rarely while doing it. In order to prevent hip or knee issues from developing as a result of changing your stride due to pain, it is imperative that you get treatment for plantar fasciitis.
Does plantar fasciitis last a lifetime?
Although it normally goes away on its own, plantar fasciitis may be excruciating. In most cases, it might take up to two years to settle. A tiny percentage of individuals with really severe plantar fasciitis may experience the ailment for years at a time.
Why did I develop plantar fasciitis so quickly?
People between the ages of 40 and 60 are most likely to suffer from plantar fasciitis. specific forms of physical activity. Plantar fasciitis can develop as a result of activities that put a lot of strain on your heel and surrounding tissue, such as aerobic dancing, ballet dancing, and long-distance jogging.
How can plantar fasciitis be verified?
In order to diagnose plantar fasciitis, the clinical history and physical examination are crucial. Morning stiffness and increased pain while bending the foot upward (dorsiflexion), which happens during activities like standing on your toes or climbing stairs, are the most significant aspects of the clinical history.
How can plantar fasciitis be healed the quickest?
In order to cure plantar fasciitis on your own, you should stretch your plantar fascia many times a day, ice your foot, take NSAIDs, rest your foot, use orthotics to support your arch and heel, and limit the amount of time you spend doing painful activities like jogging or walking.
Can plantar fasciitis be alleviated by drinking water?
Plantar fasciitis. The inflammation of the band of tissue that connects the heel bone to the toes is known as plantar fasciitis. Water consumption can help control the pain and inflammation associated with plantar fasciitis. pain in the nerves.
Does plantar fasciitis benefit from heat?
Since heat doesn’t reduce pain and can exacerbate swelling, it is generally not advised to utilize heat therapy alone to treat plantar fasciitis. It can, however, be used in conjunction with cold and ice treatments; this is known as contrast therapy.
What is frequently confused with plantar fasciitis?
Summary: Compression of the posterior tibial nerve during its passage through the tarsal tunnel, which is situated close to the inner ankle, results in tarsal tunnel syndrome. This disorder can cause heel and arch pain and sensory abnormalities, which frequently resemble plantar fasciitis.
Who is most affected by plantar fasciitis?
About 10% of runner-related injuries and 11% to 15% of all foot complaints that call for expert medical attention are caused by this ailment. Approximately 10% of the general population suffers from plantar fasciitis, and 83% of those affected are active, working people between the ages of 25 and 65.
References
Plantar fasciitis – Symptoms and causes. (n.d.). Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/plantar-fasciitis/symptoms-causes/syc-20354846
Plantar Fasciitis. (2024, September 9). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/14709-plantar-fasciitis
Dhameliya, N. (2022d, August 5). Plantar Fasciitis – Cause, Symptoms, Treatment, Exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/plantar-fasciitis/