
Brachioradialis Muscle
The brachioradialis muscle is a forearm muscle that plays a significant role in both the flexion and extension of the forearm. It is located on the lateral side of the forearm, running from the distal end of the humerus (upper arm bone) down to the radius (one of the two bones of the forearm).
Additionally, depending on the posture of the forearm, it can pronate or supinate. It is attached to the lateral supracondylar line of the humerus through the brachioradialis tendon and is linked to the distal styloid process of the radius.
What Is The Brachioradialis Muscle?
Despite having flexor activity, the brachioradialis is classified as a posterior or extensor-compartment muscle. One of the two forearm extensor-compartment muscles that do not cross the wrist is this particular muscle; the other is the supinator. Though innervated by the radial nerve, the brachioradialis flexes pronates, and supinates the forearm. Thus, a radial nerve palsy/lesion rather than a median or ulnar nerve lesion may be indicated by the decreasing of this muscle or its tendon reflex during neurologic testing.
The two most common causes of brachioradialis dysfunction are trauma and prolonged overuse. The brachioradialis is essential in surgery for carpal tunnel release, forearm tendon transplants, and hand deformity reconstruction. Comprehending the physical importance of the medicine for these muscles is essential for properly diagnosing and managing many musculoskeletal disorders.
The brachioradialis is the muscle on the radial side of the forearm that sits closest to the skin. Its thin belly ends at the mid-forearm, from which a long, flat tendon radiates to the radius. Supinator longus is another term for it.
Structure of the Brachioradialis Muscle
It is possible to palpate the brachioradialis muscle in the anterolateral forearm. The muscle is fusiform in shape, getting larger at the muscle belly and becoming thinner farther out to places through a thin tendon at the attachment point.
The base of the lateral radial styloid process is where the brachioradialis places distally after originating proximally from the proximal two-thirds of the lateral humeral supracondylar ridge. The muscle only crosses the elbow joint because of these attachments. The brachioradialis affects the muscle tissue that covers the anterolateral forearm.
In association with the wrist extensors, the brachioradialis muscle forms the lateral cubital fossa boundary. The brachial artery, median nerve, and biceps tendon all pass through this vital area on the flexor surface of the elbow.
The volar superficial, volar deep, dorsal superficial, dorsal deep, and movable band the five forearm divisions. The brachioradialis muscle, along with the extensor carpi radialis longus and extensor carpi radialis brevis, is situated in the mobile wad compartment.
From the lateral side of the forearm lies a superficial, fusiform muscle called the brachioradialis. It begins proximally on the humerus’s lateral supracondylar ridge. It inserts near the base of the styloid process, distally on the radius. It demonstrates the elbow pit’s lateral boundary close to the elbow, it is called the cubital fossa.
Function of the Brachioradialis Muscle
The forearm is bent at the elbow by the brachioradialis. The brachioradialis tends to supinate when it flexes when the forearm is pronated. Its tendency when it flexes in a supinated position is to pronate.
When the forearm is positioned almost between supination and pronation at the radioulnar joint, For the flexion of the elbow, the brachioradialis muscle has more strength.
When rapid motion is necessary or while lifting weight during gradual forearm flexion, the brachioradialis flexes the forearm at the elbow. When in a midposition, like when hammering, the muscle must function to stabilize the elbow during rapid flexion and extension.
Elbow flexion is the main function of the brachioradialis muscle. however whether the forearm is pronated, neutral, or supinated, the muscle contracts when the elbow flexes. The elbow flexion, the brachioradialis supports the forearm. When the forearm is supinated, the muscle works as a supinator; when the forearm is pronated, the muscle acts as a pronator.
Origin
The anterior aspect of the arm’s lateral intermuscular septum and the upper two-thirds of the lateral supracondylar ridge of the humerus are the sources of the brachioradialis muscle. It enters the anterolateral cubital area by moving across the lateral surface of the elbow joint.
Insertion
The muscle fibers form a thick tendon around the middle of the forearm as they run inferiorly along the radial portion of the anterior forearm. After that, the tendon runs the length of the forearm and is placed close to the wrist, directly in front of the styloid process of the radius.
Nerve Supply
The radial nerve supplies stimulation to the brachioradialis muscle. Although the majority of the neuron input to the brachioradialis comes from spinal roots C5 and C6, this nerve receives contributions from spinal roots C5 to C7.
The distal part of the radial nerve is situated anteriorly between the brachioradialis muscles. The radial nerve divides into superficial and deep branches distal to the elbow joint. The radial nerve’s superficial branch extends with the brachioradialis in the forearm and laterally to the radial artery.
The brachioradialis and extensor carpi radialis longus tendons are where the superficial radial nerve comes superficially in the distal direction. The brachioradialis is one of the earliest muscles to heal after radial nerve damage.
Blood Supply
The radial recurrent artery, a branch of the radial artery that serves the forearm and adds to the anastomotic network of the elbow joint, supports the brachioradialis muscle.
The primary superficial veins of the upper limb climb the lateral and medial forearms, respectively, and are called the cephalic and basilic veins. The cephalic vein, which emerges from the median cubital vein in most individuals, traverses the antecubital fossa before merging proximally with the basilic vein.
However, many differences exist in the superficial venous drainage of the elbow and forearm. In the meantime, the arm and forearm’s designated arteries are covered by paired vessels made of deep veins.
Lymphatics Drainage
There are both superficial and deep lymphatic vessels in the brachioradialis lymphatic drainage, which is a component of the upper limb lymphatic system. The superficial venous vasculature is closely followed by the superficial lymphatic vessels.
A portion of the superficial lymphatic system drains into the cubital lymph nodes by following the basilic vein. The axillary lymph nodes receive the lymphatic veins that surround the cephalic vein. Along with the deep veins, the brachioradialis fluid is drained by the deep lymphatic arteries, which ultimately discharge into the axillary lymph nodes.
Related Muscles
From the lateral humeral supracondylar ridge, the brachioradialis muscle develops together with the extensor carpi radialis longus muscle. One of the seven muscles in the superficial layer of the forearm that attaches to the lateral epicondyle and supracondylar ridge of the humerus is the brachioradialis.
The extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, extensor carpi ulnaris, and anconeus are the other six muscles that originate from these locations.
Embryology
The lateral plate of the layer and the somatic layer are the source of the upper limb, which develops into a limb bud after around 26 days. While the lateral plate also gives rise to the tendon and other connective tissue, the somatic mesoderm creates the muscle. By the seventh week, superficial muscles, such as the brachioradialis, are different from deeper muscles.
The newly created connective tissue separates the limb muscles into extensor and flexor components as the limb buds lengthen. Sonic hedgehog protein is secreted by the zone of polarizing activity, which is situated at the posterior boundary of the upper limb bud and it regulates anterior-posterior patterning.
Anatomical Variation
Different anatomic variants of the brachioradialis have been documented in research. One variation includes two brachioradialis muscle stomachs and two superficial radial nerves with a similar base and attachment location.
The two muscular belly layers are called superficial and surface layers. Because it passes between the muscular bellies, one of the superficial radial nerves is more likely to become taken. A divided brachioradialis is present in another variation, where the superficial branch of the radial nerve passes through both muscle movements. These variations can lead to the development of Wartenberg’s syndrome, a disorder resulting from entrapment of the superficial branch of the radial nerve.
It has also been seen that muscle fibers from a more proximal origin fuse with the brachioradialis. In one variation, the humeral midshaft, close to the distal deltoid insertion, is the source of the proximal muscle fibers. It has been claimed that the acromial level is where the accessory muscle fibers might develop, and this variety can improve the muscle’s supinating ability. Compression of the radial nerve that causes symptoms is also more likely in accessory brachioradialis muscles.
It has also been established that the brachioradialis is placed into the third metacarpal. With this variation, the wrist joint can be moved by the muscle.
Surgical Considerations
A significant phase in radial surgery using the volar method, also known as the Henry approach, is the radialis arm muscles. This method optimizes the exposure of radial bone during volar plating along the distal radius. The approach divides the operative site into proximal and distal interneuron lines. Between the flexor carpi radialis and the brachioradialis is the distal internervous plane. The space between the pronator teres and brachioradialis is accepted as the proximal internervous plane.
The brachioradialis or palmar cutaneous branch of the median nerve is situated deep within the wrist region, served by the superficial radial nerve. The median nerve’s palmar cutaneous branch is located medial to the flexor carpi radalis tendon. Careful planning retraction or dissection in this region helps prevent damage to the median and distal radial nerves.
Before volar plating, the brachioradialis can be loosened to aid with reduction since it serves as a shaping force on the distal radius. Research indicates that there is no discernible clinically significant reduction in elbow flexion or wrist function when the brachioradialis is released during the healing of a distal radial fracture.
Compression of the superficial radial nerve may be the cause of Wartenberg syndrome, which causes discomfort in the dorsoradial wrist and hand. Surgical decompression is used to treat the problem. This is achieved by releasing the fascia that lies between the extensor carpi radialis longus and the brachioradialis.
Clinical Significance
Wartenberg syndrome is caused by compression of the superficial radial nerve in the subcutaneous plane by the brachioradialis and extensor carpi radialis longus tendons or fascial band. The symptoms, which are typically paresthesia and scorching pain over the wrist, thumb, index, and middle fingers, are brought on by forearm pronation.
The patient may have had handcuffs, tight wrist bands, or casts in the past, or they may have had forearm fractures. Only sensory problems are brought on by this kind of radial neuropathy. Wrist flexion with ulnar deviation and the Tinel and Finkelstein tests are two physical exam techniques that might cause Wartenberg syndrome. A surgical decompression procedure can improve the situation.
In clinical settings, the C6 spinal nerve is tested via the brachioradialis tendon. Elbow flexion with either supination or pronation of the forearm results from striking the brachioradialis tendon.
Spiraling around the humeral groove, the radial nerve is susceptible to injury from a humeral midshaft fracture. The first muscle that the radial nerve innervates distal to the fracture is the brachioradialis. Therefore, observing brachioradialis function aids in tracking this nerve’s recovery.
After radial nerve damage at the humeral midshaft level, the brachioradialis and extensor carpi radialis longus are the first two muscles to regain motor strength. The rate at which a lesioned radial nerve regains function is roughly 1 mm.
Even with conservative treatment, reinnervation of the brachioradialis usually occurs in 3 or 4 months. If, after six months, the brachioradialis has not strengthened, surgical arm exploration may be performed.
Associated conditions
Brachioradialis strain
A sudden force applied to the wrist or forearm can overstretch the brachioradialis muscle, leading to a minor or severe tear.
This can cause the forearm to enlarge and ache, making it difficult to move the arm normally.
Brachioradialis tendinitis
A sudden force applied to the wrist or forearm can overstretch the brachioradialis muscle, leading to a minor or severe tear.
This can cause the forearm to enlarge and ache, making it difficult to move the arm normally.
Forearm weakness from cervical radiculopathy
Forearm weakness and pain may be the result of a pinched nerve in the neck.
This may have an impact on the brachioradialis muscle, which may make wrist and arm movement challenging.
Avulsion fracture of the brachioradialis tendon
A strong force applied to the forearm may split the brachioradialis tendon from the radius bone, resulting in a tendon tear.
An avulsion fracture occurs when a portion of bone is also ripped from the tendon.
Forearm discomfort, bruising, and swelling are possible consequences of this fracture.
Additionally, nerve injury could occur, causing tingling and numbness in the hand and arm.
It is important to consult a physician if one thinks they may have a brachioradialis muscle ailment.
They may assist someone in brachioradialis rehabilitation in addition to providing an accurate diagnosis of the ailment.
Rehabilitation
Heat and Ice
The hand and brachioradialis should be treated with an icepack to assist reduce localized pain, inflammation, and edema.
Applying ice should last for five to ten minutes.
Heat therapy may be applied a few days after the injury has healed to encourage blood flow and enhance tissue suppleness.
You can apply heat for ten to fifteen minutes on many occasions a day.
Avoiding heat-related burns or ice-related frost burns requires caution.
Massage
The brachioradialis muscle contains an excessive number of trigger points, therefore massage therapy in this area can be beneficial.
Increased blood flow, increased tissue mobility, and pain reduction are all benefits of massage.
Kinesiology Tape
The brachioradialis muscle may benefit from kinesiology taping, according to the physical therapist.
The tape can be used to lessen discomfort, improve muscular function, or lessen post-injury muscle spasms.
Kinesiology taping is a relatively new technique in the rehab industry, hence research on it is limited.
Assessment Of Brachioradialis Muscle
Palpation
The anterolateral surface of the forearm will be palpated.
Muscle Test
We will ask the patient to bend their forearm in a mid position, which entails bending their elbow against resistance, to concentrate on the brachioradialis.
For the three primary elbow flexors—the biceps, brachialis, and brachioradialis—this is how the MMT is usually executed.
It should be noted that during the test, the wrist flexor muscles should be relaxed since tight wrist flexor contractions may facilitate elbow flexion.
Exercises of Brachioradialis Muscle
Stretching Exercise for Brachioradialis Muscle
Standing brachioradialis stretch

- With your elbows firmly locked out, extend your arms in front of you.
- After placing one hand over the other, interlock your fingers.
- Bend your lower hand’s wrist.
- When you feel a significant brachioradialis stretch, rotate your wrist to the left. Hold it for ten to thirty seconds, then rotate your hands to the right and repeat with the opposite arm.
Arms down brachioradialis stretch

- Interlock your fingers and cross your wrists over one another.
- Next, rotate your upper wrist away from your body while maintaining a locked-out elbow position.
- Try to hold each stretch for ten to thirty seconds as you repeat the same movement with your other arm.
Arms back brachioradialis stretch

- stand up tall and with a proper posture.
- With your palms pointing back, pronate your hands by your sides.
- Now, extend your arms behind your body (as if you’re rowing with straight arms) without bending your waist or shifting your hips until you feel the deep brachioradialis stretch I described earlier.
- Hold it for ten to thirty seconds, then do one or two more sets of it.
Strengthening Exercise for Brachioradialis Muscle
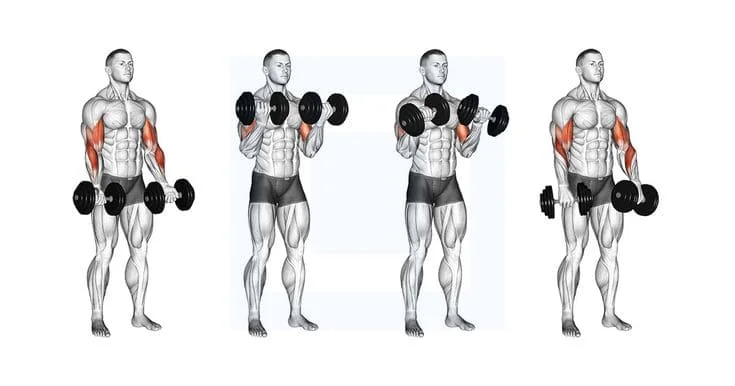
Dumbbell Hammer Curls

- Each hand should hold a dumbbell in a neutral grip.
- Maintain a straight back and a taut core when standing.
- Curl the dumbbells steadily upward until your bicep is in contact with your brachioradialis.
- To slowly lower the dumbbell, tense your biceps.
- Repeat this exercise for 2-4 sets of ten to fifteen repetitions
Reverse Grip EZ Bar Curls
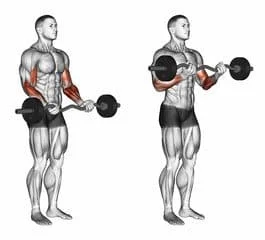
- Assume a standing position and foot placement akin to the Cable Hammer Curl.
- Take hold of the EZ-curl bar that is attached to the bottom of the cable by facing down on the angled portion of the bar.
- The same as you would with a standard bicep curl workout, curl the bar up and down.
- Maintain your elbow and shoulder postures tightly in place while you perform the cable hammer curl.
- For 2-4 sets of 10–20 repetitions, repeat.
Dumbbell Forearm Twist

- Hold a dumbbell in each hand that is relatively heavy and maintain a neutral hand position.
- While you rotate your wrists (first in a pronated position, then a supinated position), keep your posture constant.
- Aim for muscle failure after 20–30 repetitions for one or two sets.
Bent Arm Hang

- Using your hands shoulder-width apart, grasp the bar or the rings.
- Keep your chin above the bar for as long as possible, using only your hands for support.
- Rest and repeat for 1-2 sets lasting at least 30–60 seconds.
Zottman Curl
- Dumbbells should be held out to the sides.
- Curl the load up to the shoulders while maintaining the palms facing up.
- At the peak of the movement, stop.
- Turn the grip slightly so that the palms point down.
- Using an overhand hold, slowly lower the dumbbells back to the starting position.
- Return to the beginning posture and turn the hands once more until the dumbbells are nearly at the thighs.
Cable Hammer Curl

- Position yourself facing the machine and fasten a cable attachment to a low pulley.
- Using a neutral grip (palms in), grab hold of the rope.
- For the duration of the exercise, position your elbows sideways and remain there.
- Pull the arms till the forearms and biceps meet.
- Hold on for a moment.
- Start lowering the weight gradually to its starting position.
- Continue for the recommended amount of times.
Dumbbell Reverse Curl
Hold a dumbbell at your sides in each hand while seated or standing.
Thumbs should be pointing toward your legs, and palms should be facing backward.
Lift the weights to your shoulders while bending your elbows and tucking in your upper arms.
Never rotate your wrists.
Repeat after lowering the weights.
Reverse Cable Curl
Fasten a bar onto a machine with a low pulley.
Use a pronated (palms down) grip to hold the handle.
Place your feet approximately shoulder-width apart, your shoulders back and down, and your core taut.
Curl the handle up to your shoulders while bending your elbows and keeping your upper arms close to your sides.
Repeat with your arms extended.
Close-Grip Pull-Up
Pull-up bars are held in place with your thin overhand grasp.
Face forward and contract your lats.
Pull your upper chest towards the bar while squeezing your back muscles, bending your arms, and keeping your legs motionless.
As you lower yourself back down, feel your arms extend.
Execute one or two sets of six to twelve reps.
Summary
Most regularly documented compression disorders have anatomical sources in the forearm, while radial nerve compression is rarely found in the upper arm. Radial nerve compression locations above the elbow have been identified as the teres major, the triceps muscle, the intermuscular septum area, and the gap between the brachialis and brachioradialis muscles.
We report the case of a 38-year-old male patient who did not exhibit any neurological abnormality and complained of dorsolateral forearm discomfort and paraesthesias.
Radial nerve compression at the brachioradialis muscle’s humeral origin was discovered during the surgical investigation. Symptom relief was achieved by successfully releasing the nerve at this location.
FAQ
What type of muscle is the brachioradialis?
The lateral region of the posterior forearm contains the fusiform muscle known as the brachioradialis. It is part of the radial group of forearm muscles, which are a part of the superficial layer of posterior forearm muscles, together with the extensor carpi radialis brevis and extensor carpi radialis longus.
What are the two actions of the brachioradialis?
Along with the biceps brachii and brachialis, the brachioradialis largely produces elbow flexion, or the ability to bend the elbow. Additionally, the brachioradialis muscles rotate the forearms inward (pronation) and outward (supination).
Do bicep curls work brachioradialis?
The primary targeted muscles are the elbow flexors (biceps brachii, brachioradialis, and brachialis), the arm flexors (e.g., anterior deltoids), and wrist supination/pronation. A dynamic or mostly isometric arm flexion combined with an elbow flexion defines the biceps curl.
Why does my brachioradialis hurt?
Brachioradialis muscle soreness is usually the result of overexertion and impairs the ability to grip, twist, and lift objects, such as a corkscrew, screwdriver, or cup of tea. The elbow can be bent by using the brachioradialis muscle, which runs down the back of the forearm, in conjunction with the biceps.
What exercises are good for brachioradialis pain?
Exercises like elbow flexion and wrist curls, both in reverse, can fall under this category. As the muscle gains strength, start with lighter weights and progressively increase the resistance. Physical treatment: Rehabilitating the brachioradialis muscle and other forearm and elbow muscles can be aided by physical therapy.
How do you know if you have a brachioradialis injury?
Sharp, abrupt pain may be followed by continuous discomfort that is accompanied by soreness, stiffness, or edema. Additionally, playing sports like racquetball and tennis can lead to overuse of this muscle. The overuse of the brachioradialis is also common in those whose jobs require them to lift or carry large goods.
What is the origin of brachioradialis pain?
Typical reasons for brachioradialis discomfort include Repetitive Overuse: physical labor, some sports like weightlifting and racket sports, and even computer typing, which are instances of tasks involving the brachioradialis muscle being used repeatedly. The most frequent cause of brachioradialis pain is repetitive usage.
What are brachioradialis issues?
Overuse or overstretching of the muscle can result in injuries to the brachiordialis. Blunt trauma from falls blows, or lifting weighty objects can also injure the muscle. Sharp, abrupt pain may be followed by continuous discomfort that is accompanied by soreness, stiffness, or edema.
How to build brachioradialis?
The reverse barbell curl is the first exercise that works the brachioradialis. For this exercise, I recommend switching between an EZ bar and a straight bar. You can then aim for both the pronated and neutral positions. We move on to the Offset Dumbbell Reverse Curl exercise.
How to make brachioradialis?
Barbell Curl in reverse. This brachioradialis workout, also called the overhand curl, works your biceps and forearms directly.
Dumbbell Hammer Curl.
Rear Front Rotations.
1-Arm Kettlebell Reverse Curl.
Resistance Band Hammer Curl.
Reverse Dumbbell Zottman Curl.
1-Arm Kettlebell Hammer Curl.
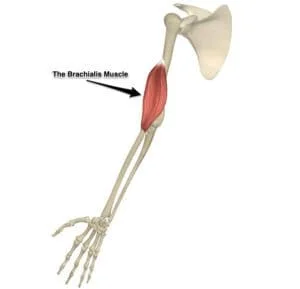
What is the difference between brachialis and brachioradialis?
The brachialis and brachioradialis are two muscles in the arm that are frequently neglected. The muscle that connects the upper arm to the forearm is called the brachioradialis, while the muscle between the bicep and the triceps is called the brachialis.
What is the brachialis muscle used for?
An essential forearm flexor muscle at the elbow is the brachialis. As a “pure flexor” of the forearm at the elbow, the brachialis allows for elbow flexion in all physiologic situations. It is deeper than the biceps brachialis muscle and is located in the anteroinferior region of the arm.
What nerve is brachioradialis?
The radial nerve (C5–C6), which passes next to the brachioradialis muscle, produces innervation for the muscle. In a similar vein, the radial recurrent artery, a branch of the radial artery, provides blood supplies.
How do you reduce brachioradialis?
Relax. As far as possible, avoid using during the 72 hours after the start of pain.
Ice. Every two hours, you should apply ice for 20 minutes to reduce swelling and irritation.
compression. Use a medical bandage to loosely wrap your forearm to reduce swelling.
A rise in altitude.
Is brachioradialis a bone?
On the lateral side of the forearm lies a superficial, fusiform muscle called the brachioradialis. It begins proximally on the humerus’s lateral supracondylar ridge. It inserts near the base of the styloid process, distally on the radius.
What exercises are good for brachioradialis pain?
Exercises like elbow flexion and wrist curls, both in reverse, can fall under this category. As the muscle gains strength, start with lighter weights and progressively increase the resistance. Physical treatment: Rehabilitating the brachioradialis muscle and other forearm and elbow muscles can be aided by physical therapy.
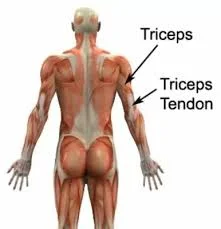
What causes loss of Brachioradialis reflex?
Depending on the anatomical location of damage to the nerve, a radial nerve injury may impact the brachioradialis reflex or the triceps reflex. A musculocutaneous nerve injury may impact the biceps reflex.
What is unique about the brachioradialis?
One of the two forearm extensor-compartment muscles that do not cross the wrist is this particular muscle; the other is the supinator. The radial nerve innervates the brachioradialis, which flexes, pronates, and supinates the forearm.
What nerve controls brachioradialis?
The radial nerve (C5–C6), which passes next to the brachioradialis muscle, produces innervation for the muscle. In a similar vein, the radial recurrent artery, a branch of the radial artery, provides blood supplies.



5 Comments