Extensor Carpi Ulnaris Muscle
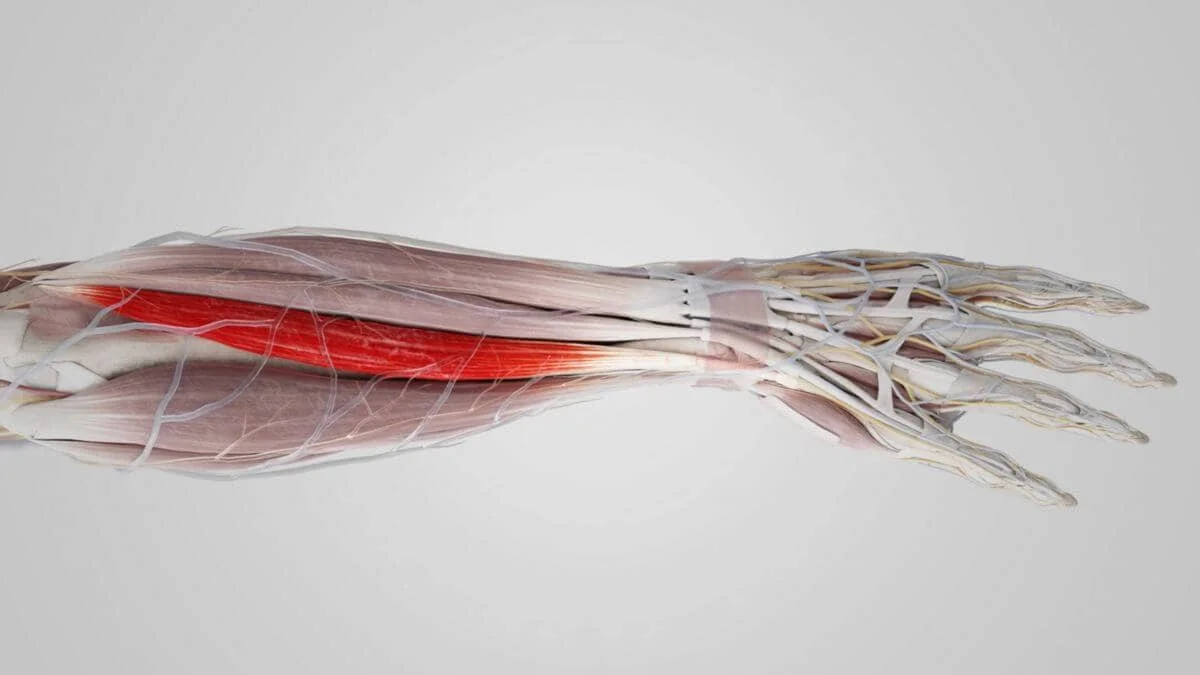
The extensor carpi ulnaris muscle is a prominent anatomical structure located in the forearm, essential for various t is situated on the ulnar side of the forearm, running along the posterior aspect. The posterior edge of the ulna and the lateral epicondyle of the humerus are the origins of this muscle. It extends distally, inserting into the base of the fifth metacarpal bone.
What is the Extensor Carpi Ulnaris Muscle?
The primary purpose of the elongated fusiform muscle known as the extensor carpi ulnaris, which is situated in the posterior compartment of the forearm, is to extend and adduct the wrist. It reaches the elbow from the base of the little finger.
Along with the brachioradialis, anconeus, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, and extensor digiti minimi, the extensor carpi ulnaris muscle is a member of the superficial group of forearm extensors.
The posterior part of the ulna and the lateral epicondyle of the distal humerus are its points of origin. It travels via the sixth compartment of the extensor retinaculum before attaching to the dorsal base of the fifth metacarpal. It is supplied with blood by the ulnar artery and innervated by the posterior interosseous nerve.
Structure of Extensor Carpi Ulnaris Muscle
There are two heads to the extensor carpi ulnaris muscle: the ulnar and humeral heads. The humeral head is linked to the lateral epicondyle of the humerus, which originates from the common extensor tendon. The same aponeurosis, which is connected to the ulna’s posterior border, is the origin of the ulnar head.
The flexor carpi ulnaris, flexor digitorum profundus, and deep fascia of the forearm all share the same extensor tendon. Within the tendinous sheath of the extensor carpi ulnaris, the extensor carpi ulnaris tendon runs beneath the extensor retinaculum in a groove between the posterior surface of the head and the styloid process of the ulna, forming a distinct compartment of the extensor retinaculum, distally, just proximal to the wrist.
Relations of Extensor Carpi Ulnaris Muscle
The most medial muscle in the forearm’s extensor compartment is the extensor carpi ulnaris. However, the superior fibers of this muscle are only medially positioned by the tiny, triangular-shaped anconeus muscle.
The extensor digiti minimi and extensor digitorum muscles are connected laterally to the extensor carpi ulnaris. The ulnar artery’s cutaneous branch emerges from the space created by the flexor and extensor carpi ulnaris tendons. This branch runs distally.
Functions of Extensor Carpi Ulnaris Muscle
There are two purposes for the extensor carpi ulnaris. It extends the hand at the wrist joint by working along the extensor carpi radialis longus and extensor carpi radialis brevis. The extensor carpi ulnaris adducts the hand at the wrist in addition to the flexor carpi ulnaris.
When clenching the fist (tight flexion of the medial four digits), the extensor carpi radialis longus, extensor carpi radialis brevis, and extensor carpi ulnaris work in tandem to provide medial support to the wrist.
The extensor carpi ulnaris (ECU), which provides vital medial stability and aids in both wrist extension and adduction, is a key component in wrist and forearm function.
Adduction and Extension
Medial Stability: The wrist’s medial stability, which helps to prevent excessive lateral deviation, is greatly influenced by the ECU in addition to its control over movement.
Fiber Origin: The ECU has a unique fiber origin that comes from the proximal ulna and the distal humerus, one of the bone origin of the common extensor tendon.
For physiotherapists to create successful rehabilitation plans for patients with wrist and forearm injuries, they must have a thorough awareness of the ECU’s role, including how it affects wrist movement and stability.
Origin
The posterior portion of the ulna and the lateral epicondyle of the distal humerus are the origin of the extensor carpi ulnaris muscle.
Insertion
After going through the sixth compartment of the extensor retinaculum, it attaches itself to the dorsal base of the fifth metacarpal.
Nerve
The posterior interosseous nerve (C7–C8), a motor branch of the radial nerve, supplies nerve fibers to the muscle. The posterior interosseous nerve is formed when the radial nerve descends posteriorly via the heads of the supinator muscle in the antecubital fossa.
Together with the other muscles in the posterior compartment of the forearm, it innervates the extensor carpi ulnaris muscle. The posterior cord, which receives input from the spinal nerve roots of C5 to T1, leads to the radial nerve’s emergence from the brachial plexus.
Action
The extensor carpi ulnaris, when used alone, extends the wrist and rotates the hand to the ulnar side. When used repeatedly, however, it extends the elbow joint.
The muscle is a minor extensor of the carpus in carnivores, but it has changed to a flexor in ungulates. It would be referred to as the ulnar lateralis in this instance.
Blood Supply
The ulnar artery, which splits off the brachial artery close to the antecubital fossa and serves the medial side of the forearm, is the main origin of blood flow for the extensor carpi ulnaris. The muscle also receives from the posterior interosseous artery, a posterior branch of the radial artery that supplies both the superficial and deep extensor muscle groups.
Lymphatics
The lymphatic drainage system of the upper limb consists of both superficial and deep lymphatic vessels. Along with superficial veins like the basilic vein, the superficial lymphatic vessels of the hand and forearm ascend the arm and enter the cubital lymph nodes close to the medial epicondyle of the humerus.
The apical axillary lymph nodes are the primary drainage location for superficial lymphatic veins that pass more proximally to the cephalic vein, however, the deltopectoral lymph nodes are another possible drainage site. The forearm and arm’s deep lymphatic vessels follow the deep veins until they reach the humeral axillary lymph nodes and, ultimately, the subclavian lymphatic trunk.
Embryology
The forearm muscles originate from dorsolateral somite cells that migrate to the limb during the fourth week of development and eventually mature into muscles. The muscles start to split into distinct functional groups, such as the flexors and extensors, as the limb buds lengthen. A sonic hedgehog protein released from the zone of polarizing activity determines the anterior and posterior pattern of the limb.
Muscles
One of the forearm’s extensor muscles, the extensor carpi ulnaris, is situated in the superficial layer of the posterior compartment. The brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, and extensor digiti minimi are the other muscles that occupy this compartment. Many of these muscles have a single origin on the lateral epicondyle through the same extensor tendon. The extensor retinaculum holds each of these muscles in place as they approach their distal insertion sites.
Anatomical Variation
Some people have extensor carpi ulnaris accessory tendinous slips, which may make them more vulnerable to injury. It may also raise the risk of tendinopathy and muscle dislocation, functionally limit the wrist and fifth digit, and prolong the symptoms of extensor carpi ulnaris syndrome.
The accessory slip comes in three varieties: kinds A, B, and C. The most often recognized type, type A, inserts into the base of the fifth metacarpal. Type B attaches to the fifth metacarpal’s midshaft, while Type C attaches to the metacarpal head. The extensor carpi ulnaris gives birth to a functioning auxiliary digiti minimi.
Surgical Considerations
In many orthopedic treatments, such as those involving the distal humerus, elbow joint, forearm, and wrist, the anatomic position of the extensor carpi ulnaris is crucial. For example, after open reduction and internal fixation of the olecranon and proximal ulnar fractures, the extensor carpi ulnaris is recognized by its original fibers on the lateral epicondyle and dorsal aspect of the end of the ulna. It may be necessary to manipulate this muscle to locate the fracture’s components.
The subluxation of the extensor carpi ulnaris is one injury that may necessitate surgery. It is more common in athletes who do frequent, forceful wrist rotations than in the general population. In sports, tennis, golf, and water polo are the most common causes of this injury. The tendon’s fibro-osseous subsheath is ruptured, causing the dislocation when the forearm is supinated. The sixth compartment of the extensor retinaculum, which is attached to the distal ulna, includes a component of this covering.
According to the research, three types of retinal tears could be the origin of this illness. Sheath ruptures of type A are obvious and leave the sheath only slightly above the tendon. Type B refers to a sheath rupture that occurs radially and occurs in the bone’s ulnar groove. Last but not least, type C happens when the fibro-osseous sheath separates from the ulna’s periosteum, creating a fake pouch for the tendon.
Individuals who suffer from this injury frequently report experiencing a sharp ache in the wrist’s dorsal-ulnar aspect. Regarding how to manage this injury, there is some discussion. On the other hand, fibro-osseous sheath surgery works well. Direct suturing of the sheath over the tendon is an excellent treatment for individuals with radial rupture of the fibro-osseous sheath securing the tendon.
Patients who experience an ulnar rupture of the sheath have rebuilt using their natural extensor retinaculum. Patients can resume their prior level of functioning in their respective sports without discomfort or recurring dislocation after this procedure is properly completed.
Clinical Significance
The extensor carpi ulnaris is a crucial muscle involved in wrist and forearm movements, supporting medial stability as well as wrist extension and adduction. The majority of injuries occur in sportsmen who use strong wrist motions.
Tenosynovitis can result from repeated wrist flexion and extension because these movements irritate the tendon and its sheath. Additionally, overuse can result in tendinopathy, a condition in which the tendon thickens and becomes painfully stiff while sustaining little structural damage. Extended periods of high strain on the tendon may result in structural deterioration and a partial tear.
The Extensor Carpi Ulnaris Muscle’s Performance
To assess the instability or function of the extensor carpi ulnaris muscle, ask the patient to stretch their fingers and pronate their forearm. To create resistance against the motion, place your hand along the hand’s medial border. After that, the extended wrist is adducted against the opposition. If the muscle is working normally, the tendon can be palpated around the head of the ulna. The muscle is located in the proximal region of the forearm.
In other circumstances, the patient might be able to replicate the problem shortly and the value might not even result in any symptoms. The tenderness that is precisely localized to the fifth metacarpal can be found by palpating the whole length of the ECU tendon, beginning distally at its insertion to guarantee palpation of the proper structure.
The pathognomonic sign of an ECU problem is pain upon resisted active extension with ulnar deviation. Pain is commonly linked to weakness. It is conceivable that a complete rupture of the ECU tendon is represented by painless weakening.
Assessment of Extensor Carpi Ulnaris Muscle
To diagnose ECU tendon diseases, a precise clinical history and evaluation are necessary.
The distinction between acute and chronic causes is made by the timing of symptom onset. In this illness, mechanical symptoms at the outset are also common characteristics. Words like “snap,” “pop,” or “tear” are used by patients to describe an acute sheath disruption.
Tendon subluxation events can occasionally be very painful.
However, in certain cases, the subluxation may be completely asymptomatic and easily recreated by the affected individual.
Accurate identification of soreness can be achieved by palpating the whole length of the extensor carpi ulnaris tendon, starting with its distal insertion into the base of the fifth metacarpal.
The ECU tendon is likely to have completely ruptured if there is no pain.
Other Issues
Acute tendon ruptures are rare and usually happen as a result of a puncturing wound.
Treatment
Strategies for ECU Treatment Tendinopathy and Tendinosis seek to treat ECU tendinopathy and tendinosis at different phases, offering a thorough method to control symptoms and encourage healing.
Acute Tendinosis
Non-operative treatments for acute tendinopathy of the ECU usually have good results:
Rest: To aid in healing, allow the injured wrist to rest.
Modifying activities to lessen the strain on the ECU tendon is known as activity modification.
Splintage: Three weeks or so of immobilization in a short-arm plaster cast with the wrists extended at a 30° angle and the ulna twisted.
Rehabilitation for Early Reactive Phase
For tendinopathy’s early reactive phase:
Load management involves carefully planned exercises that gradually reintroduce load.
Exercises involving contracting muscles without moving joints are called isometric exercises, which can help control pain over five to ten days.
Support from Pharmacology: Ibuprofen’s anti-inflammatory properties make it a possible complement at this stage.
Chronic Tendinopathy
When chronic tendinopathy patients do not experience a rapid increase in pain:
Load management is the continual distribution and control of load.
Tendon strength and resilience can be enhanced using eccentric-focused exercises.
Strength and Isometric Exercises: Supplementary Rehabilitation targeted at improving strength and function.
Steroid Injection: If non-surgical methods fail to alleviate the symptoms, a steroid injection into the fibro-osseous sheath could be taken into consideration. This therapy aims to lessen pain and inflammation, especially when more conventional, conservative methods have not worked.
Exercise of Extensor Carpi Ulnaris Muscle
Strechinng Exercise Of Extensor Carpi Ulnaris Muscle
Wrist extensor stretch

- With the palm facing down, extend your arm in front of you.
- One arm should be bowed with the palm facing the earth.
- Bend the wrist even more downward using the opposing hand.
- The person would stretch the upper part of their forearm.
- For 10 seconds, hold the stretch; repeat as necessary
Strengthening Exercise of Extensor Carpi Ulnaris Muscle
Wrist Extension Exercise
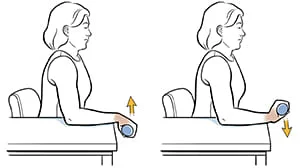
- For this method, a person requires a level surface, like a desk or tabletop.
- Also required is a lightweight dumbbell—between one and two pounds.
- Begin by placing the dumbbell on the tabletop with the working hand and wrist hanging off the edge. Then, stand or sit with your feet shoulder-width apart. with the palm pointing downward.
- When the individual is prepared, raise the dumbbell by bending the wrist and reaching as far as you can.
Eccentric wrist extensions
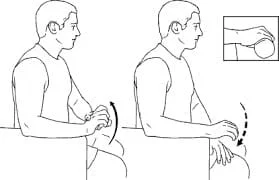
- Giving the muscle stimulus without overdoing exercise, which could potentially worsen the injury, is the key to both rehabilitation and strengthening.
- Hold a light dumbbell in your hands, and then rest your forearm with your hand dangling off the edge of a weight bench, table, or desk.
- Next, bend your wrist to lower the dumbbell to the floor gently.
- Lower the dumbbell until the person’s forearms are comfortably stretched. Then, using mostly the other hand, raise the
- dumbbell back up to the starting position by pressing the “dumbbell hand” upward.
Wrist curls

- Take a position where your hands rest easily over your legs or a bench, and your forearms are flat.
- The side where your palms are pointing up.
- You can also hold a barbell in both hands or grip a dumbbell in each hand.
- Curl the weight back up so that your palms are facing you after allowing your wrists to extend back.
- Lower gradually, then do so again.
- After finishing a set, turn the weights and your forearms so the palms face the other direction and repeat.
Zottman Curls
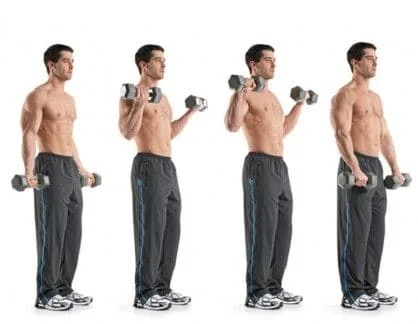
- Take a tall stance with your hands facing up and a set of dumbbells at your sides.
- Curl both dumbbells upward till your pinky fingers are close to your shoulders while maintaining a modest amount of movement and your upper arms close to your torso.
- Squeeze at this spot, rotate your wrists, and descend the dumbbells while keeping your palms facing the other direction.
- Repeat by rotating your wrists back at the bottom.
Kettlebell Swings

- Hinge at the hips and swing the kettlebell rearward, high between your thighs, while keeping it between your legs.
- To blow it up to eye level explosively, drive your hips forward.
- Allow yourself to be propelled back into the hinge position, then proceed directly to the second rep.
- Maintain a flat body and flexible knees throughout.
Reverse Grip Barbell Curl

- With your hands shoulder-width apart and your palms facing down, take a tall stance with a barbell hanging at your waist.
- As you curl the bar upward toward your chin, maintain your body still and your upper arms pinned to your sides.
- Hold, then controllably and gradually lower the bar till your arms are straight.
Weighted Pull-Ups and Hangs
- Use an overhand or neutral grip to grab a pull-up bar, and strap a weight plate or dumbbell to yourself.
- Raise your feet off the ground and dangle unrestricted.
- Flexing your elbows and bringing your shoulder blades down and back will help you stand up.
- Consider pushing your elbows all the way down into your pockets.
- Once your chin clears the bar, take a moment and then gradually return to the beginning position.
- Aim to refrain from swinging too much.
Conclusion
The Extensor Carpi Ulnaris muscle is essential for wrist adduction and extension. Injuries or dysfunction of this muscle can cause pain, weakness, and restricted wrist and forearm range of motion. A comprehensive physical examination, imaging investigations, and maybe electromyography (EMG) testing are usually required for the diagnosis.
In extreme situations, surgical intervention may be necessary in addition to rest, immobilization, physical therapy, anti-inflammatory drugs, and corticosteroid injections. The degree of the injury and the effectiveness of the treatment determine the chance of a full recovery; many patients gain a great deal from skilled care.
FAQ
What is the purpose of the carpi ulnaris extensor?
The primary purpose of the elongated fusiform muscle known as the extensor carpi ulnaris, which is situated in the posterior compartment of the forearm, is to extend and adduct the wrist. It reaches the elbow from the base of the little finger.
What nerve is extensor carpi ulnaris?
The posterior interosseous nerve (C7, C8), a branch of the radial nerve’s deep division, innervates the extensor carpi ulnaris. The posterior chord of the brachial plexus is where the radial nerve originates.
How do you strengthen extensor carpi ulnaris?
Raise your arm straight in front of you, bend your wrist back, and rotate it inward so that your elbow crease faces the floor. Maintain this posture to produce a stretch. Tennis elbow and other repetitive strain ailments can be alleviated with this exercise, which stretches the forearm extensor muscles.
What level of the spine is the extensor carpi ulnaris?
The posterior interosseous nerve, a branch of the radial nerve, innervates the extensor carpi ulnaris. Nerve fibers that emerge from the spinal cord at the seventh and eighth cervical vertebrae (C7–C8) are part of the posterior interosseous nerve.
What is the insertion of extensor carpi ulnaris?
The sixth extensor compartment at the wrist is where the tendon of the extensor carpi ulnaris passes. Attachments: connects to the base of the fifth metacarpal after emerging from the lateral epicondyle of the humerus.
What is the extensor carpi ulnaris special test?
The examiner palpates the ECU tendon with one hand while holding the patient’s thumb and long finger in the other. Next, the patient is directed to the radial deviation of their thumb against resistance. A favorable outcome is characterized as a recovery of the discomfort experienced at the dorsal ulnar aspect of the wrist.
What are the symptoms of extensor carpi ulnaris?
discomfort on the wrist’s top little finger side.
There are occasions when tendon swelling happens.
Wrist pain during resistance stretching, especially if the wrist is also bowed toward the little finger (ulnar deviation).
When pressed, the tendon could be sensitive.
How do you test extensor carpi ulnaris?
To stop the hand from moving, place your hand at its medial border. Adduction of the extended wrist occurs against resistance. If the muscle is functioning normally, its tendon can be palpated close to the head of the ulna. The muscle can be felt and visualized in the proximal region of the forearm.
What does the extensor carpi ulnaris attach to?
The sixth extensor compartment at the wrist is where the tendon of the extensor carpi ulnaris passes. Attachments: Connects to the base of the fifth metacarpal after emerging from the lateral epicondyle of the humerus. Wrist adduction and extension are the actions. Radial nerve innervation (deep branch).
How do you treat extensor carpi pain?
It is crucial to take breaks from activities that can be taxing or uncomfortable for your wrist extensor muscles so that they have time to recuperate. Ice: Using ice on the injured region might help lessen pain and inflammation.Cold for 15 to 20 minutes at numerous times a day.
Reference
- Sawyer, E., Sajjad, H., & Tadi, P. (2023, August 28). Anatomy, Shoulder and Upper Limb, Forearm Extensor Carpi Ulnaris Muscle. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK539760/#:~:text=The%20extensor%20carpi%20ulnaris%20muscle,base%20of%20the%20little%20finger.
- Extensor Carpi Ulnaris. (n.d.). Physiopedia. https://www.physio-pedia.com/Extensor_Carpi_Ulnaris
- Extensor carpi ulnaris muscle. (2024, May 4). In Wikipedia. https://en.wikipedia.org/wiki/Extensor_carpi_ulnaris_muscle
- Extensor carpi ulnaris muscle. (2023, November 3). Kenhub. https://www.kenhub.com/en/library/anatomy/extensor-carpi-ulnaris-muscle


3 Comments