Camptodactyly
Introduction
Camptodactyly is a congenital condition characterized by the permanent flexion of one or more fingers, most commonly the little finger. It results from abnormalities in tendons, ligaments, or muscles and may vary in severity. The condition can be hereditary or occur sporadically. Treatment options include stretching, splinting, and, in severe cases, surgery.
Camptodactyly is a condition in which the middle joint of a finger bends abnormally. Although it can occur in other fingers, it is most frequently found in the little finger.
Camptodactyly: what is it?
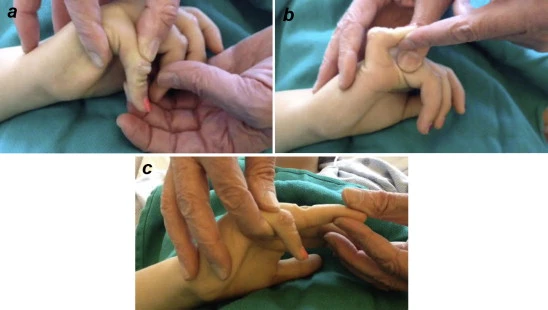
If your child has camptodactyly, it indicates that their finger is bent and cannot be fully straightened. At a joint known as the proximal interphalangeal (PIP) joint, the finger normally bends in the middle.
Some children can straighten their fingers (passive motion) with help from a physical therapist. Even with assistance, the joint could be too tight to straighten for others. About 1% of children have some degree of camptodactyly. Girls are more affected than boys.
Types
Type I: Infantile camptodactyly
- Equally impacts boys and girls.
- Adapts well to splinting and stretching
Type II: Adolescent camptodactyly
- More often affects girls than boys.
- Surgery might be necessary.
Type III: Syndromic camptodactyly
- Impacts many fingers
- Linked to several syndromes
- Severe and frequently present from birth
Symptoms
Your child might not exhibit any symptoms if they have moderate camptodactyly. Although their finger—likely the small one—will be somewhat bent, it won’t interfere with how they use their hand. Your child’s hand function may be slightly affected if their case is more severe.
The primary symptom of camptodactyly is a slightly flexed posture of the middle joint, which prevents the finger from fully straightening. It is most common in the little finger, but it can also affect other fingers. Over time, the condition may get worse, and it frequently gets worse during increases in growth. In most cases, camptodactyly does not cause pain or significantly impair hand function.
Your child has camptodactyly if their finger is bent and unable to straighten entirely.
It could begin in adolescence or be present from birth, and it could get worse as the child gets older.
Your child won’t have any symptoms if the condition is mild. The little curvature of the finger, most likely the little one, will not have any effect on hand function. Your child’s hand function may be slightly affected if their case is more severe.
- At least one finger is bent all the time.
- The proximal interphalangeal (PIP) joint is where the finger bends in the center.
- In extreme situations, even with assistance, the joint is too tight to straighten.
Causes
Your child’s finger may have abnormal structures that lead to camptodactyly. These could consist of: The majority of the time, the cause of this is unknown. However, some kids with camptodactyly have a family history of similar issues with their fingers.
- Tight skin
- Contracted tendons and ligaments
- Abnormal muscles
- Irregularly shaped bones
- Abnormal muscles in the hand.
- Differences in bone shape
- Camptodactyly might be caused by problems with the skin, tendons, ligaments, muscles or bones of the finger.
- Camptodactyly could be a hereditary disorder (inherited in families).
Additionally, camptodactyly may be a symptom of a more widespread illness or sickness that impacts numerous body parts.
Risk factor
Risk factors for camptodactyly include abnormal structures in the fingers, genetic conditions, and syndromes.
- Abnormal structures
- Tight skin
- Contracted tendons and ligaments
- Abnormal muscles
- Irregularly shaped bones
- Abnormal lumbrical insertion
- Abnormal flexor digitorum superficialis insertion
- Abnormal extensor tendon anatomy
Genetic conditions
- Camptodactyly can be inherited as an autosomal dominant trait.
- Mutations in the connexin-43 gene (GJA1) may cause misassembly of channels or alter channel conduction properties.
Diagnosis
The first step in identifying camptodactyly at Children’s Hospital of Philadelphia (CHOP) is usually a physical examination of your child’s hand and fingers. To confirm the diagnosis, doctors may occasionally suggest an X-ray. X-rays assist physicians in determining the hand’s underlying structure by creating images of the bones.

Along with X-rays and a physical examination, your child might also have:
- Tests of range of motion to see if the illness is impairing agility and flexibility
- Tests for nerve evaluation to see whether any nerves have been harmed or compressed
- A precise diagnosis aids us in choosing the best treatment plan for your child.
Treatment
Since mild camptodactyly rarely results in pain or functional issues, surgery is typically not advised. The doctor will likely advise your child to wear a splint and undertake physical therapy if their disease is moderate.
If your child’s finger curve is more severe, and it is becoming worse, surgery might be necessary. Your child’s finger may still have some bend, even though surgery can help it work better. Following surgery, splinting and physical therapy are required to avoid joint stiffness.
The majority of camptodactyly patients don’t need surgery. Nonoperative treatment will be advised if your child has minor camptodactyly, which is defined as less than a 30-degree bend in their finger that does not impair hand function.
Physical therapy treatment
Goals
- Correction of palmar tissue shortening and reduction of fixed flexion contracture at the PIPJ
- Prevention of contracture development or recurrence
- Maintenance of flexion range
Treatment options that don’t involve surgery include:
Massage
Before stretching the finger(s), massage your muscles and tissues to loosen them. Although older kids might be able to do this on their own, a parent or other adult should help.
Please check below for advice on how to massage the affected fingers.
- Apply a moisturizer or massage oil to the affected fingers and hands. (Ensure your child is not allergic to any substances in the cream or oil used.)
- Apply strong pressure to the region. (Massage should not cause discomfort or damage to the skin.)
- Use the other hand’s fingers to support the back of the injured finger.
- With your thumb, rub the front as well as sides of the affected finger.
Splinting

Physical therapy splinting is quite effective, and the best outcomes come from early intervention. The first treatment location, with follow-up sessions possibly taking place at a local hospital. The degree of bending and the amount of pressure required to straighten the finger will determine the course of treatment.
Throughout the treatment, the splints will be observed and modified. Splints are usually only needed to be worn while you sleep, but occasionally you may need to wear them for eight to twenty hours per day.
- Splinting: With the help of an physical therapist, the initial line of treatment consists of a program of finger stretching and splinting.
- Stretches for the affected finger or fingers to increase range of motion
- To keep the bent finger straight, use a splint.
- Dynamic finger orthosis (capener orthosis) indicated for adolescents with contractures of 45 degrees or less, who are very proactive during the day and unlikely to comply with stretching and active extension strengthening regimens, gain the most from this orthosis.
A camptodactyly splint is a device that supports and straightens a bent finger. It’s frequently composed of mouldable plastic.
When do you use a splint?
- A doctor may prescribe occupational therapy and a splint for mild camptodactyly.
- To treat camptodactyly in children, a therapist may propose a splint to keep the affected finger straight.
- A camptodactyly splint is a device that supports and straightens a bent pinky finger. It is used to treat mild cases of camptodactyly, which causes a finger to bend.
How it functions.
- The hand-based splint lengthens the palmar skin and extends the PIPJ.
- It is attached with tape or Velcro at the distal end of the proximal phalanx.
- The splint should be comfortable and not involve unaffected fingers, thumbs, or wrists.
Therapeutic play

- Taking hold of blocks and bigger objects, like balls
- Playdoh/putty games
- Musical instruments: piano, hand drums
- Weight bearing exercises and Activity
Surgical treatment
Your child’s doctor might suggest surgery if your child’s finger curvature increases quickly or if it gets to the point where it affects hand function. Surgery is dependent on the finger’s deformity. After surgery, bending the finger may become difficult, and success rates are frequently low. For children, no one surgical technique is advised.
If your child’s camptodactyly is severe, worsening over time, or impairing their hand function, surgery may be recommended. Surgery is most beneficial when performed while your child is still young and the bones have not fully developed.
Children with hand issues benefit from several surgeries performed by board-certified orthopedic and plastic surgeons at CHOP.
Two commonly used procedures are:
- Dividing the tendon that causes the muscle to shorten.
- Transferring a tendon and/or muscle to restore balance in the hand.
- In rare situations, if a child’s camptodactyly is caused by abnormal bones or bone structure, surgeons may need to undertake surgery to repair, remove, or fuse a bone to improve hand function.
During this procedure, the joint’s range of motion may be lost. Following surgery, your child’s finger, hand, or arm may be immobilized in a cast, splint, or sling while it heals.
Complication
- Stiffness: Residual stiffness in the finger after surgery
- Hand function: More severe cases can affect hand function
- Difficulty holding objects: People with severe camptodactyly may have trouble holding objects
- Progression of deformities: In non-operative cases, the condition may progress
- Other features of camptodactyly: Tight skin, contracted tendons and ligaments, Abnormal muscles, and irregularly shaped bones.
FAQs
Why does camptodactyly occur?
Why does camptodactyly occur? Issues with the skin, tendons, ligaments, muscles, or finger bones may be the cause of camptodactyly. Camptodactyly may be a genetic disorder that runs in families. A syndrome is a collection of symptoms, and camptodactyly may be one of them.
Is camptodactyly a congenital condition?
A rare, genetic, non-syndromic, congenital limb malformation known as camptodactyly of the fingers is characterized by a permanent, often bilateral, flexion contracture at the proximal interphalangeal joint of a postaxial finger that is painless, non-traumatic, and non-neurogenic. This causes the affected digit to be permanently volarly inclined.
How does camptodactyly get treated?
Since camptodactyly rarely causes pain and typically has little effect on hand function, symptoms are commonly overlooked in a child’s early years. Depending on how severe the disease is, treatment options may include surgery, splinting, and stretching.
How can a small finger that is bent be straightened?
One of the most effective strategies for restoring extension to a bent finger is to use a well-designed splint or orthosis to apply a modest, continuous corrective force over time.
What is type 3 camptodactyly?
Hand camptodactyly is linked to facial dysmorphism (flat face, hypertelorism, telecanthus, symblepharon, simplified ears, retrognathia) and neck abnormalities (short neck with striking pterygia, muscle sclerosis) in Camptodactyly syndrome, Guadalajara type 3, a rare genetic bone development disorder.
My baby’s finger is bent; why?
A child with clinodactyly has a finger that curls to one side. Although it can affect other fingers, it often affects the little (pinky) finger. Usually, it is caused by abnormal finger bone growth and development.
Does camptodactyly tend to progress?
The proximal interphalangeal joint (PIPJ) of the fifth finger is most frequently affected by camptodactyly, a nontraumatic and progressive flexion deformity that may or may not affect the other fingers. The first finger is always spared.
Will my bent finger straighten out?
If mallet finger injuries are treated promptly, the majority of fingers recover. You should be able to straighten your fingertip once again following hand therapy and splinting. It occasionally stays slightly bent or has a bump on the underside of the joint, but it still works as it should.
Where may one see camptodactyly?
In the general population, 1 in 300 people have camptodactyly, or flexion contracture of the proximal interphalangeal joint (PIP), a solitary deformity that can be inherited as an autosomal dominant trait with different manifestations. It usually manifests as a tiny finger malformation, which might be bilateral.
What is the camptodactyly surgery?
A wide range of surgical techniques, including capsular release, lumbrical excision, tendon transfer, flexor digitorum superficialis (FDS) lengthening, osteotomy, and arthrodesis, are used to address the underlying structural abnormalities.
Reference
- Camptodactyly | Boston Children’s Hospital. (n.d.). https://www.childrenshospital.org/conditions/camptodactyly
- Camptodactyly – Alder Hey Children’s Hospital Trust. (2024, March 19). Alder Hey Children’s Hospital Trust. https://www.alderhey.nhs.uk/conditions/patient-information-leaflets/camptodactyly/
- Camptodactyly in Children | Children’s Hospital Colorado. (n.d.). https://www.childrenscolorado.org/conditions-and-advice/conditions-and-symptoms/conditions/camptodactyly
- Glick, Y., & Weerakkody, Y. (2011). Camptodactyly. Radiopaedia.org. https://doi.org/10.53347/rid-13487
- Wikipedia contributors. (2024, November 18). Camptodactyly. Wikipedia. https://en.wikipedia.org/wiki/Camptodactyly
- Kate. (2022, June 28). Camptodactyly – GC Hand Therapy. GC Hand Therapy. https://gchandtherapy.com/camptodactyly/
- St George’s University Hospitals NHS Foundation Trust, H. T. D. (2023). Hand therapy treatment for children with camptodactyly. https://www.uhs.nhs.uk/Media/UHS-website-2019/Patientinformation/Childhealth/Hand-therapy-treatment-for-children-with-camptodactyly-3474-PIL.pdf
- Philadelphia, C. H. O. (n.d.). Camptodactyly. Children’s Hospital of Philadelphia. https://www.chop.edu/conditions-diseases/camptodactyly
- Occupational Therapy Department. (2014). Congenital hand anomalies: camptodactyly. In The Royal Children’s Hospital. https://www.rch.org.au/uploadedFiles/Main/Content/hand-therapy/congenital_hand_anomalies-camptodactyly.pdf