The atlanto-occipital joint is the articulation between the atlas (C1 vertebra) and the occipital bone of the skull. It is a synovial joint that allows for nodding movements of the head, such as flexion (“yes” motion) and slight lateral tilting.
This joint is stabilized by ligaments, including the anterior and posterior atlanto-occipital membranes, and plays a crucial role in supporting and facilitating head movements while maintaining stability.
Introduction
A paired, symmetrical articulation between the base of the skull and the cervical spine is called the atlantooccipital joint (also called the C0-C1 joint).The craniovertebral joints are a collection of joints that includes the atlantoaxial joint.
At the atlantooccipital joint, flexion-extension is the primary movement. This motion allows the head to nod, as is done when expressing acceptance (the “yes” motion). From a functional standpoint, these two ellipsoid (condyloid) joints can be regarded as a single joint because they operate concurrently.
Although stability is sacrificed, the upper cervical spine region is made to provide a great deal of motion. For this reason, the fibrous capsules, ligaments, articular surfaces, and surrounding muscles are primarily responsible for maintaining joint stability in the craniocervical region.
Anatomy
Articulations
Each joint is made up of two concave articular surfaces on the superior aspect of the lateral mass of atlas, which articulate with a convex surface on the occipital condyle.The joint is strengthened by fibrous capsules that support each joint.The atlanta facets are inclined medially.
Capsule
The atlantooccipital articulation capsules surround and connect the occipital bone’s condyles to the atlas’ articular processes; they are thin and loose.
Attachments
Attachment-of-Atlanto-Occipital-Joint
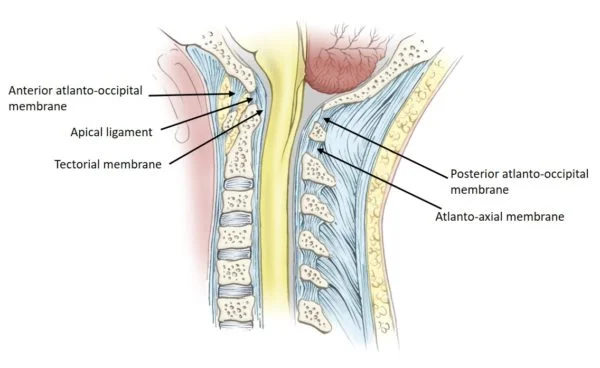
The anterior atlanto-occipital membrane is a large, dense fibrous structure that connects the top border of the anterior arch of the atlas (C1) to the anterior inferior margin of the foramen magnum. It is a continuation of the anterior longitudinal ligament and helps to prevent excessive neck extension. Laterally, it integrates with the joint capsule, while medially it is reinforced by a strong, rounded cord that joins the basilar occipital bone to the anterior atlantal tubercle.
The posterior atlanto-occipital membrane is a large but thin fibrous membrane that connects the upper border of the anterior side of the atlas’ posterior arch (C1) to the posterior margin of the foramen magnum. It connects with the posterior atlantoaxial membrane inferiorly (part of the ligamentum flavum) and the ligamentum nuchae posteriorly, and it is located directly posterior to the spinal dura. Suboccipital muscles are located posteriorly. The atlantic (V3) section of the vertebral artery travels anteriorly, piercing the membrane and dura before becoming the dural (V4) portion.
Tectorial membrane: the posterior longitudinal ligament extends from the dens to the anterior portion of the foramen magnum.
Articular surfaces
The synovial articulation between the occipital bone and the first cervical vertebra (atlas) is known as the atlantooccipital joint. The occipital bone’s convex surfaces articulate with the concave articular facets of the C1 vertebra, which have an oval (elliptical) form and are reciprocally concave-convex. No intervertebral disc separates the occiput from C1. There is hyaline cartilage lining every articular surface. In the first cervical vertebra, the inferior articular facets are located.
These facets can be seen on the superior portion of the lateral mass of the vertebra. They are concave, oval in form, and somewhat slanted medially. In the anteromedial direction, each facet’s two long axes run obliquely, meeting at the midline immediately in front of the atlas. On the inferior part of the occipital bone, near the occipital condyles, are the superior articular facets. Elliptical in shape, these two rounded protuberances are extended and convex on both their long and short axes. The occipital condyles are orientated anteromedially, and are placed immediately lateral to the anterior part of the foramen magnum.
Ligaments & Joint Capsule
The articular capsule that surrounds each atlantooccipital joint is thin and flexible. The synovial membrane lines this fibrous tissue-based capsule. It adheres to the articular facets’ edges. Both the lateral and posterior portions of the capsule exhibit thickenings.
A number of ligaments span the atlantooccipital joint and contribute to its stability. They are the lateral atlantooccipital ligament, anterior atlantooccipital membrane and ligament, posterior atlantooccipital membrane, tectorial membrane, alar ligament, apical ligament, and ligamentum nuchae.Two of these are thought to be the main ligaments of the atlantooccipital joint because they link the occipital bone with the atlas. The following are the:
Anterior atlantooccipital ligament (and membrane)
Posterior atlantooccipital membrane
The dense band of fibrous tissue known as the anterior atlantooccipital ligament extends from the top border of the anterior arch of the atlas to the anterior border of the foramen magnum.The anterior longitudinal ligament, which serves as the anterior atlantooccipital membrane, strengthens it medially, and laterally it merges with the atlantooccipital joint capsule.
The posterior part of the atlantooccipital joint is covered by a thin membrane known as the posterior atlantooccipital membrane. It extends inferiorly from the top border of the posterior arch of Atlas to the superior posterior boundary of the foramen magnum. Its lateral edges run the length of the posteromedial joint capsule. It is a significant clinical hallmark that the posterior atlantooccipital membrane is close to the vertebral artery and C1 nerve.
Innervation
The anterior rami of spinal nerve C1 innervate the atlantooccipital joint.
Arterial supply
The deep cervical, occipital, and vertebral arteries anastomose.
Blood supply
An anastomosis between the deep cervical, occipital, and vertebral arteries supplies blood to the atlantooccipital joint.
Function
The following movements are permitted in this joint:
Flexion and extension around the mediolateral axis, resulting in the typical forward and backward nodding of the head.
Minor lateral motion, lateroflexion, to one or both sides of the anteroposterior axis.
Flexion is primarily caused by the activity of the longi capitis and recti capitis anteriores, whereas extension is caused by the recti capitis posteriores major and minor, the obliquus capitis superior, the semispinalis capitis, splenius capitis, sternocleidomastoideus, and upper trapezius fibers.
The recti laterales are involved in lateral movement, with the trapezius, splenius capitis, semispinalis capitis, and sternocleidomastoideus on the same side all working together.
Movements
The atlantooccipital joint has two degrees of freedom of motion since it is an ellipsoid joint. Flexion-extension and lateral flexion are two examples. However, flexion and extension are the main movements possible at the atlantooccipital joint. This is due to the atlantal sockets’ form, which is deep enough to keep the occipital condyles from translating too much and enable the atlantooccipital joint to give the head some stability while it balances on the cervical spine.
In the anteroposterior plane, flexion and extension movements take place around a transverse axis. Over the concave facets of the atlas, the convex occipital condyles slide posteriorly and roll forwards concurrently during flexion. Consequently, the occipital bone is moved away from the atlas’s posterior arch. This enables a forward tilting, or downward nod, of the head, like the “yes” movement used to express acceptance. The fibrous structures that surround the joint (joint capsules, posterior atlantooccipital membrane, ligamentum nuchae) and the posterior suboccipital muscles restrict flexion to roughly 5°–10°.
The opposite motions take place in extension. The gap between the occipital bone and the atlas’s posterior arch is closed by the occipital condyles, which roll backward and slide anteriorly on the atlantal facets. The extension range of motion is limited to roughly 10° by the occipital bone, the atlas, and the axis.
The range of motion at the atlantooccipital joint is not significantly affected by lateral flexion.The lateral flexion of the upper cervical spine is actually limited to about 5-8° on each side in cadaveric studies. Additionally, the lateral flexion of the upper cervical spine is a double-joint and linked movement. When lateral flexion and a slight degree of contralateral rotation happen simultaneously, this is referred to as coupled movement. When multiple joints move simultaneously, it’s referred to as double-joint movement.
The combined movements to accomplish lateral flexion of the upper cervical spine are thus as follows: a small quantity of contralateral glide at the occipital condyles (lateral flexion); concurrently, one occipital condyle moves somewhat anteriorly while the other moves posteriorly (rotation); and in addition to these movements, the second vertebra rotates (relatively) against the third cervical vertebra, resulting in an overall range of motion for lateral flexion of the upper cervical spine that is between 5 and 8°.
Muscles acting on the atlantooccipital joint
The cervical spine is made more mobile by the action of the postvertebral and anterior neck muscles on the atlantooccipital joint.
Flexion from a standing posture
Trapezius, splenius capitis, longissimus capitis, semispinalis capitis, rectus capitis posterior major, rectus capitis posterior minor, obliquus capitis superior
From the supine posture, flexion
Sternocleidomastoid, longus capitis, rectus capitis anterior muscles
Extending from the standing position
Sternocleidomastoid, longus capitis, rectus capitis anterior muscles
Extending from the prone posture
Rectus capitis posterior major, rectus capitis posterior minor, obliquus capitis superior, semispinalis capitis, splenius capitis muscles, cervical part of trapezius
Lateral flexion
The splenius capitis, semispinalis capitis, trapezius, rectus capitis lateralis, and sternocleidomastoid
Muscles acting on the atlantooccipital joint
The rectus capitis anterior and longus capitis muscles are the primary flexors of the head on the neck. The obliquus superior capitis, semispinalis capitis, splenius capitis, trapezius, rectus capitis posterior major, and rectus capitis posterior minor are the primary extensor muscles. Nevertheless, the precise muscles used in these motions may vary based on the head’s starting posture.
Strong motion is required to raise the head and flex it forward on the neck while in a supine position. The muscles of the anterior neck are the primary movers in this situation. These muscles include the rectus capitis anterior, longus capitis, and sternocleidomastoid.
Since the weight of the head can cause it to bend when it is upright, the same strength is not needed. The forward bend movement in this situation is controlled by the posterior muscles of the neck and back. The short suboccipital muscles, the splenius capitis, the longissimus capitis, the semispinalis capitis, and the trapezius are among them.
Similar to this, the anterior neck muscles (such as the sternocleidomastoid and longus capitis) regulate the head’s ability to extend from an upright position by acting against the head’s weight. To raise the head into extension while in the prone position, primary movers are required. These muscles include the cervical portion of the trapezius, the obliquus capitis superior, the semispinalis capitis, the splenius capitis, and the rectus capitis posterior major and minor.
The anterior and posterior neck muscles work together to cause the head to flex laterally. Among these are the muscles of the rectus capitis lateralis, trapezius, splenius capitis, semispinalis capitis, sternocleidomastoid, obliquus capitis superior, and rectus capitis posterior minor. Sternocleidomastoid, rectus capitis posterior minor, obliquus capitis superior, and splenius capitis support the linked movement of rotation.
Clinical significance
Dislocation
The atlanto-occipital joint can be dislocated, particularly in traumatic events like traffic crashes.This can be diagnosed with CT scans or magnetic resonance imaging of the head and neck. Surgery could be utilized to repair the joint and any related bone fractures. Neck movement may be limited for a long time following this injury. Such injuries may also cause hypermobility, which can be identified via radiography. This is especially true if traction is applied during treatment.
Three forms of AOD are distinguished by the occipital dislocation recommendation:
Anterior displacement
Posterior displacement
Longitudinal distraction.
Damage to the related ligaments occurs along with dislocation. The degree of dislocation is the primary determinant of the injury’s severity. Stages I and II show no or very little displacement and sufficient ligament preservation. Stage III is characterized by significant dislocation and extremely unstable damage. Damage to the spinal cord’s cervical area may be linked to stage III.This might be lethal.The neurological abnormalities that survivors of this kind of damage may experience include unilateral or bilateral muscular deficiencies, lower cranial nerve deficits, or even quadriplegia, or paralysis of all four limbs.
FAQs
Is the atlanto-occipital joint an ellipsoid one?
The atlantooccipital joint, which is an ellipsoid, has two degrees of freedom of movement.These include flexion-extension and lateral flexion. However, the primary mobility allowed at the atlantooccipital joint is flexion-extension.
Is the atlanto-occipital joint a pivotal joint?
The atlanto-occipital joint (O-C1) serves as a pivot for the cranium’s flexion/extension motion, with 13 degrees average flexion/extension and 8 degrees lateral bending, enabling just a few degrees of axial rotation.
How stable is the atlanto-occipital joint?
The tectorial membrane and alar ligaments supply the majority of the support for the atlanto-occipital joint, and damage to these ligaments causes instability due to low inherent osseous stability.
What kind of lever is the atlanto-occipital joint?
The Atlanto-Occipital Joint is a First Class Lever. A first-class lever in the human body is the head and neck during neck extension.The fulcrum (atlanto-occipital joint) connects the load (front of the skull) with the effort (neck extensor muscles).
Is the atlanto-occipital region synovial?
The atlanto-occipital articulation (also called the C0-C1 joint or articulation) is made up of two condyloid synovial joints that connect the occipital bone (C0) to the first cervical vertebra (atlas).
What makes up the atlanto-occipital joint?
The atlanto-occipital joint connects the atlas bone to the occipital bone. It is composed of two condyloid joints. It is a synovial joint.
What are the biomechanical properties of the atlanto-occipital joint?
Atlanto-occipital joint biomechanics. Although the atlanto-occipital joint is capable of flexion, extension, rotation, and lateral bending, cadaveric studies reveal that flexion and extension are its main motions. Bony components are the primary constraint on this motion (Wolfla, 2006).
Which feature of the atlantooccipital joint is the most distinctive?
This bone’s most distinctive feature is its robust dens, an odontoid process.To put it simply, the atlantooccipital joint is made up of two condyloid joints. The atlantooccipital joints are synovial socket joints, which have shallow sockets when a baby is born and deeper sockets as people age.
References
Atlantooccipital joint. (2023, August 3). Kenhub. https://www.kenhub.com/en/library/anatomy/atlanto-occipital-joint
Wikipedia contributors. (2024c, August 24). Atlanto-occipital joint. Wikipedia. https://en.wikipedia.org/wiki/Atlanto-occipital_joint
Bell, D., & Jarvis, M. (2015). Atlanto-occipital articulation. Radiopaedia.org. https://doi.org/10.53347/rid-35478
Rupapara, H. (2023, March 29). Atlanto-occipital joint – Anatomy, Ligament, Muscles, Movement. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/atlanto-occipital-joint/
The term metabolism refers to a variety of chemical reactions that occur within our bodies. These functions help with breathing, food digestion, and cell repair, to mention a few.
Our body’s basal metabolic rate (BMR) is the amount of energy it requires to carry out those chemical activities. A higher BMR is associated with a faster metabolism, whereas a lower BMR is associated with a slower metabolism.
Numerous factors, including age, body size, gender, and—most importantly—genetics, can influence how quickly or slowly our metabolism speeds up.
One of the main components of metabolism is the thermic effect, which may be simply explained as a process of heat generation. This can be achieved by eating alone or doing activities. As a result of this process, more fat is burned and more calories are burned.
The maintenance of muscles requires more energy than that of fat cells, hence individuals with greater muscular mass also often have quicker metabolisms. This is one of the causes of our slower metabolism as we age, as our muscle mass declines with age.
The 33 foods that are thought to help burn fat or increase metabolism are listed below. Not only might incorporating a handful of these products into your diet potentially aid in weight reduction, but many of them also include a variety of essential vitamins and minerals.
What Are Fat Burning Foods?
Though certain foods are more successful than others at promoting the speed and efficiency of metabolism, fat-burning foods are thought to be those that stimulate the metabolic process.
Consuming any food causes the metabolism to begin, but many foods have additional components that accelerate the process. As we shall discuss in more depth shortly, components like proteins and carbohydrates are particularly crucial when it comes to the thermic impact.
A dietary item that stimulates a chemical response is generally referred to as a “fat-burning food”; this reaction has a direct impact on other processes that might improve weight reduction.
The sensation of fullness, a reduction in the number of calories absorbed, and a reduction in the amount of food taken are a few instances of these processes.
Everything will become a bit more apparent when we discuss each item separately and how it influences your ability to burn fat.
24 Fat-burning or metabolism-boosting foods
Chili Peppers
Coffee
Tea
Pulses
Ginger
Chocolate
Apple Cider Vinegar
Coconut Oil
Water – Ice
Avocado
Whole Grains
Eggs
Asparagus
Greek Yoghurt
Spinach
Cottage Cheese
Broccoli
Citrus Fruits
Oats
Poultry
Cinnamon
Bananas
Sweet potatoes and yams
Chili Peppers:
A fantastic dietary item to consider when considering ways to increase your metabolism and burn fat is chili peppers.
In chili peppers, capsaicinoids are the active ingredient that gives them their spiciness. Moreover, this fat-burning meal has anti-inflammatory and antioxidant qualities.
Capsaicinoids have been shown in studies to help suppress appetite, which can result in a natural reduction in body weight by reducing food intake.
Additionally, the thermic effect and the browning of adipose tissue, which is a result of increased energy expenditure, activate the prevention of diet-induced obesity. The quantity of calories burned is enhanced as a result of this process encouraging energy expenditure. Because they can promote the induction of browning in white cells, capsaicinoids are therefore the important actors.
Coffee:
Although coffee is not strictly a food and is usually drunk for its energizing and energizing properties, it has been included on our list of foods that increase metabolism and burn fat for the following reasons.
Eventually, caffeine increases the amount of a chemical element called epinephrine, sometimes known as adrenaline, which speeds up our metabolism. As it passes through the circulation, it instructs the fat cells to release and break down.
Although caffeine, the primary stimulant that keeps us up and energized, can influence metabolism, all of the stimulants included in coffee can have an impact. Adenosine is an inhibitory transmitter, which means that caffeine also inhibits this neurotransmitter.
Tea:
Although it is not a meal, tea—more especially, green tea—can be included in this list of superfoods for weight reduction that burn fat like a furnace! There are a lot of teas that promise to help us battle belly fat and drop a few pounds, so it’s reasonable to be cautious.
Our bodies create norepinephrine, a neurotransmitter, and when green tea catechins raise the amounts of this transmitter, our fat breaks down more quickly.
Another enzyme that prevents the synthesis of norepinephrine is monoamine oxidase. In addition, the ECG in green tea can block monoamine oxidase, which makes norepinephrine more efficient in burning fat.
It has been demonstrated that consuming green tea before exercise enhances its benefits; in fact, green tea extract is a common ingredient in pre-workout supplements. Green tea has been demonstrated to increase your metabolism even at rest, however it is improved during activity.
Though they are still in the early phases of the study, it has been shown that the catechins in tea, such as ECG, can especially assist in reducing visceral fat in our bodies. Therefore, additional research is required.
Pulses:
While pulses are a general name for a variety of food products, legumes, and pulses are both foods that raise metabolism and burn fat. Furthermore, it goes without saying that their high protein content is the primary cause of their capacity to increase metabolism.
When compared to macronutrients like fats and carbs, high-protein meals need our systems to expend more energy and calories to break down. As a result, the previously described thermic action causes a quicker metabolism and higher calorie burn when more energy is used to digest certain meals.
High-protein meals also tend to make us feel filled for longer periods, which naturally helps us lose weight by consuming less food overall.
Amino acids like methionine, which is abundant in beans and pulses, are important components of diets that aid in weight reduction and are very good at increasing metabolism. This is because methionine promotes fat burning by combining it with sulfur and B vitamins.
Complex carbs may be found in legumes and pulses. In order to longer satiate our hunger and provide us with a consistent supply of energy throughout the day, our body breaks down these foods more slowly.
In addition to burning fat, they are a terrific addition to any diet since they are packed with several nutrients, such as potassium, zinc, and B vitamins.
Ginger:
For fat-burning foods that are simple to include in a regular diet, ginger is a fantastic choice. Gingerol is the primary active ingredient in ginger, and it is this substance that stimulates a variety of bodily biological processes.
More precisely, gingerol is recognized for its ability to stabilize blood sugar levels and for its antioxidant properties, which help the body avoid oxidative stress (an imbalance between antioxidants and radicals).
Numerous studies have demonstrated that gingerol may help us digest our meals more quickly, which translates into a quicker metabolism and maybe an anti-obesity impact.
Ginger is one of the foods that burn fat because it contains the chemicals zingerone and shogaols, which are both good for burning fat.
They include additional nutrients like calcium, iron, and magnesium in addition to the fat-burning elements, all of which are essential for a balanced diet.
Chocolate:
This may come as a welcome surprise, but chocolate is one of the most highly praised meals for burning belly fat! Its primary component is cacao.
Cacao helps with blood circulation, blood sugar regulation, digestive enzyme support, and hunger suppression.
The high magnesium profile of this meal, which is linked to reduced blood levels of insulin and glucose, makes it one of the fat-burning foods. What makes this important? When we overproduce insulin, it is stored as fat in our bodies. Insulin production increases with the amount of sugar we eat.
By lowering insulin levels, magnesium can help reduce the amount of fat that is stored in our bodies. It also helps ATP (adenosine triphosphate) turn food into energy, which is crucial for intense exercise.
Foods that burn fat fast are especially abundant in dark chocolate. Selecting chocolate that has 70% or more cacao is a fantastic way to get your fill of cacao; it will have less sugar and dairy and more antioxidants, which can help avoid chronic diseases.
Apple Cider Vinegar:
The detoxifying effects of apple cider vinegar are widely recognized, and this is usually the primary reason why individuals choose to use it. Nevertheless, it has also drawn more and more attention as a meal that burns fat as you sleep.
Acetic acid, which is included in apple cider vinegar, helps to increase the body’s metabolism while also preventing fat from being deposited in the body. Additionally, it may slow down our digestion and decrease our appetite, which would keep us feeling fuller for longer. Naturally, weight loss will benefit from feeling fuller for longer because, in principle, this leads to consuming fewer calories.
Because vinegar slows down the pace at which glucose enters our blood, it immediately lowers blood sugar levels. For those who already have diabetes or are trying to prevent the disease from developing, this is very crucial.
A decrease in abdominal fat has been discovered to be facilitated by an increase in AMPK, which may be achieved by consuming apple cider vinegar.
According to research, subjects who drank one tablespoon of apple cider vinegar every day exhibited improvements in their waist circumference, blood triglycerides, and body fat percentage. Triglycerides, a kind of blood fat, are important because, after food is ingested, any wasted calories are transformed into triglycerides, which are subsequently stored as fat.
Coconut Oil:
As a vegetarian cooking oil that burns belly fat, coconut oil is a terrific, nutritious substitute for sunflower oil or other cooking fats.
Coconut oil can help burn fat when combined with a nutritious diet, but it cannot directly affect weight reduction.
Compared to long-chain triglycerides, which are commonly found in meat and animal products, medium-chain triglycerides (MCTs), which are present in coconut oil, are generally less likely to be stored as fat.
Including fat-burning items like coconut oil in our diets may also make us feel fuller longer, which promotes weight reduction naturally.
Additionally, the good cholesterol that circulates throughout the circulation and helps the body get rid of bad cholesterol, HDL cholesterol, can be raised by coconut oil.
Coconut oil may be used in cooking or poured over salads to enhance taste, making it a helpful addition to the list of foods that aid in fat burning. Naturally, this makes it an excellent alternative to animal fats for vegetarians and vegans.
Water – Ice:
Given its accessibility and significance, water has earned a spot on this list of meals that burn fat. One thing to keep in mind is that our bodies frequently confuse hunger with thirst. Try drinking a glass of water the next time you feel hungry and see how it affects your mood.
Remarkably, consuming cold water instead of room temperature water can encourage the body to burn more fat. For what reason is this? The reason is that in order to prepare the water for digestion, the body must expend additional energy. Notably, a brief rise in metabolism following cold water consumption might eventually show to be a useful weight reduction tool.
Along with other items that aid in weight reduction, drinking water also helps to keep you from being dehydrated. Our total muscle mass may decrease as a result of muscles breaking down protein. Regretfully, this may make exercise more difficult and less efficient.
Our bodies utilize water for practically all of their functions, and being hydrated allows our blood vessels to relax, which lowers blood pressure.
Since our bodies require water to burn fat in the first place, dehydration can significantly decrease the efficiency of foods that burn fat. Because our brains are already dehydrating when they detect thirst, it is advised to drink water throughout the day rather than just when you feel thirsty.
Avocado:
The fitness industry has helped to increase the appeal of the superfood avocado, which is a renowned competitor among meals that burn body fat. Nowadays, avocados are served in practically all UK cafes.
The avocado may have qualities that aid in fat burning and metabolic enhancement in addition to its high nutritional content.
Healthy fats are abundant in avocados. We need both monounsaturated and polyunsaturated fats in our diet to absorb fat-soluble vitamins, but increased monounsaturated fat intake—found in avocados—is linked to decreased cholesterol.
Avocados have been shown to have appetite-suppressive properties, which is one of the main reasons they are regarded as one of the foods that burn belly fat quickly. As previously said, this is a natural weight reduction solution since it establishes the basis for consuming fewer calories.
Additionally, avocados’ protein composition contributes to its reputation as one of the morning foods that aid in fat burning. Protein has a major role in increasing metabolism because of its thermic impact, which is linked to an increase in energy expenditure.
Avocados include monounsaturated fats, which burn more quickly than saturated fats and may also help people stop nibbling after meals. In addition to being high in fat, they are also a great source of fiber, which is a nutrient that is vital for our digestive systems and helps us feel fuller for longer.
Avocados are one of the foods that raise metabolism and burn fat, but because of their fat content, they should only be eaten in moderation. There are other methods to incorporate it into our diets, though. They may be added to salads, smoothies, or even eaten on toast for breakfast.
Whole Grains:
Whole grains are used in many different goods and are among the numerous foods that burn fat and are simple to include in your diet. Generally speaking, any unprocessed grain is referred to as whole grains. Buckwheat, quinoa, whole wheat couscous, and whole wheat bread are a few examples.
Oddly, 8-week research examining the impact of whole grains on metabolism and weight control discovered that subjects shed more weight when they ate a diet rich in whole grain items.
Additionally, they had a greater resting metabolic rate than those who were following the same diet but were consuming processed grains instead of whole grains.
Eggs:
The high protein content of eggs improves metabolism and satiety, making them one of the meals that burn belly fat and speed up metabolism. Additionally, depending on how they are cooked, eggs often have little calories, which lowers the total number of calories consumed.
Not only are eggs one of the best breakfast options for burning belly fat, but they also provide all of the amino acids our bodies need for metabolism and overall upkeep.
In addition to lowering the hunger hormone ghrelin, eggs are known to stabilize insulin and glucose responses. This is merely another proof that eggs encourage a natural way to cut calories. Additionally, the chemical choline, which is included in eggs, works to increase metabolism and promote children’s brain growth.
Rich in essential minerals like iodine and selenium, which may both accelerate metabolism, eggs are a low-calorie fat-burning meal.
The thyroid is also affected by iodine and selenium. The thyroid is the organ that controls our metabolism, thus this is relevant. To do this, it collaborates with the crucial iodine, removing it from the blood, absorbing it, and incorporating it into the thyroid hormone. Therefore, our metabolic rate will be decreased if our thyroid gland is unable to function normally.
Asparagus:
Among the numerous nutritious foods that burn fat, asparagus is one that you should absolutely include on your shopping list. This green vegetable contains a number of nutrients, including potassium, fiber, and antioxidants, in a single meal.
One substance found in asparagus is called asparagine, and it directly affects fat burning. Additionally, asparagus has a low calorie and fat content. Well, how does this operate?
Asparagine is an amino acid that can assist our body store energy in muscle instead of fat and improve insulin sensitivity. Additionally, asparagus is one of the fat-burning foods on our list that may help decrease post-workout weariness while also aiding in the removal of waste from the body.
The indirect effects of asparagus’s fiber content make it an excellent choice for fat-burning meals that aid in weight reduction. This is because fiber is a crucial component that helps us feel satisfied for longer, which results in fewer snacks and fewer calories in total.
One of the best foods for burning fat is asparagus, which can be prepared and used in a variety of pasta meals or salads, or it can be eaten on its own as a side dish to a major meal. Remember to get some the next time you’re at the grocery store.
Greek Yogurt:
Nutritionists like Greek yogurt over regular yogurt because it’s naturally lower in sugar and richer in protein, especially when eaten plain, according to Mikus.
Additionally, it is a fantastic source of protein, which helps counterbalance the carbs it contains. “Avoid purchasing 0% Greek yogurt because 1% and 2% contain fat that will help you feel fuller for longer,” she continues.
Spinach: This leafy green is a great addition to your meals since it is high in folate, a vital B vitamin, and is full of fiber. Mikus notes that spinach has a high water content, which lowers its total calorie count while providing a high nutritional value. It may be added to smoothies, sautéed with lemon, garlic, and olive oil, or eaten raw in salads, she says.
Cottage Cheese:
Cottage cheese is on our list of foods that burn belly fat because it contains a lot of calcium, which is believed to speed up fat burning by promoting fat metabolism.
Compounds called conjugated linoleic acid (CLA) are found in cottage cheese. The body needs CLA because it reduces insulin resistance, increases metabolism, and aids in the body’s utilization of stored fat.
With 11g of protein in 100g of cottage cheese, this is just one of several items you may include in your diet to help you lose weight.
Broccoli:
Broccoli is a vegetable that is high in calcium, iron, and fiber and is a popular weight-loss product. In addition, broccoli is one of the five essential foods to eat each day and is high in nutrients.
Given its high protein content, this delicious green vegetable is an excellent choice for vegans and vegetarians who have trouble finding protein in other parts of their diet.
Glucoraphanin, a compound found in broccoli, is particularly useful in controlling our metabolism. Sulforaphane, glucoraphanin’s precursor, has the ability to reduce body weight on its own. This is done by assisting us in generating more ATP from the food we consume, which causes us to consume more calories for energy.
Citrus Fruits:
The most well-known benefits of citrus fruits are their high vitamin C content and their popularity as meals for weight loss. The main source of vitamin C, or ascorbic acid as it is known in science, is citrus fruits like oranges and lemons.
In addition to its beneficial effects on the immune system, it has been demonstrated to increase metabolism.
Research has supported the idea that vitamin C plays a significant role in meals that aid in weight reduction. According to the study’s findings, those who consume more vitamin C in their diet are probably going to burn more fat when exercising than people who consume less of it.
Ascorbic acid may be needed for the metabolic transportation of fatty acids inside cells and their mobilization for use as an energy source. According to this, ascorbic acid may naturally and indirectly promote fat burning.
Numerous antioxidants included in citrus fruits can lessen our chance of developing chronic illnesses and help manage insulin resistance, which in turn lowers blood sugar levels.
Fruits in the citrus family are adaptable. You may use them to add flavor to a variety of recipes, or you might add lemon and lime to your water to make it taste better. For additional vitamin consumption, they are also excellent additions to smoothies or salads.
Oats:
Oats are one type of whole grain that has several health benefits. In addition to being a food that burns fat fast, oats are high in fiber, which helps prolong feelings of fullness. Additionally, many oats include additional vitamins; when choosing which oats to buy, check the label for this information.
Since porridge is the most popular way to consume oats, adding them to milk helps us get more calcium. As previously mentioned, calcium has been shown to be crucial in supporting a healthy metabolism, so this is a fantastic go-to meal for a superfood combo that speeds up metabolism and burns fat.
In addition to being present in oats, selenium helps maintain a healthy thyroid, which supports a balanced metabolism.
They also include manganese, which is present in the majority of oat brands, and B vitamins, which aid in the metabolism of energy from meals. For instance, this mineral directly affects our metabolism by triggering the enzymes that break down food.
Poultry:
Chicken is one of the fat-burning meals you frequently hear about while trying to lose weight or switch to a healthier lifestyle. Chicken’s high protein and low-fat content make it a staple food for bodybuilders and gym patrons.
Although it has been shown that calcium can help with weight reduction, it has been discovered to work best for those who are overweight, so this is helpful to remember!
Additionally, chicken has a lot of B vitamins, which are necessary for the metabolism of proteins, lipids, and carbs.
This meat is unique among weight loss meals since it can be added to nearly any meal and has a wide range of taste characteristics. Turkey and chicken are examples of poultry products that consume more because of the high protein content, food breaks down more quickly, burning more calories as it passes through the digestive system.
Additionally, meals high in protein, such as chicken, help people lose weight by promoting muscle growth, which can indirectly increase metabolism because people with more muscle have quicker metabolisms by nature.
Cinnamon: Cinnamon may alter how sugar and carbs are metabolized by imitating the actions of insulin, according to studies. Because it requires more energy to metabolize, having cinnamon in your body speeds up your metabolism and increases your calorie burn, Dr. Petre says.
Bananas: Do you think bananas are healthy? You bet! A banana is a satisfying snack that has just 120 calories and 3 grams of fiber, especially when combined with nut butter. A bonus? Mikus claims that they are an excellent source of magnesium and potassium.
Sweet potatoes and yams: The antioxidant beta-carotene is abundant in sweet potatoes and yams, along with fiber and vitamin C. “This adaptable root vegetable is a fantastic addition to a well-balanced meal and can even be enjoyed as a snack,” Mikus notes. According to a 2019 study, individuals’ satiety was enhanced by sweet potatoes.
Summary
All things considered, the foods on the above list are excellent providers of fat-burning and metabolism-boosting nutrients. Including them in your diet will also supply a variety of other nutrients that are necessary for a healthy lifestyle.
FAQ’s
Which foods increase metabolism and burn fat?
12 Foods That Increase Metabolism to Help Lose Weight Fish & Shellfish: Fish (salmon, tuna, sardines, and mackerel) are high in protein and omega-3 fatty acids…. Low-Fat Milk…. Broccoli…. Lentils…. Oatmeal…. Berries.
Does green tea actually boost metabolism?
A 2021 review indicated that green tea extract may increase resting metabolic rate (RMR), which raises overall energy expenditure and may help you burn more calories while at rest. Having said that, the authors point out that not every study had favorable findings.
References:
Groth, L. (2024, February 22). 25 Fat-burning foods to help boost metabolism and overall health. Prevention. https://www.prevention.com/weight-loss/g24805401/fat-burning-foods
Foods that Boost Metabolism and Burns Fat – HealthXchange. (n.d.). https://www.healthxchange.sg/syndication/Pages/foods-boost-metabolism-burn-fat.aspx
Mitchell, K. (2024, July 8). 33 foods that help burn fat or help speed up our metabolism. OriGym Centre of Excellence. https://www.origym.co.uk/blog/fat-burning-foods/embed/#awb-open-oc__777
Have you ever questioned why some individuals eat everything they want and never seem to gain weight, while others find it difficult to eat every meal? Often, metabolism is the key.
Your body uses metabolism to turn the food and liquids you consume into energy. Your body needs energy to do things like breathe, circulate blood, and repair cells, even when you’re not moving. Losing weight may be facilitated by your body burning calories more effectively if your metabolism is greater.
What Role Does Metabolism Play in Weight Loss?
We lose weight when we consume less calories than we require. There are, however, additional aspects that are involved. For instance, each person has a different metabolism. Weight management can be easier for some people because they naturally have quicker metabolisms, but it can be quite difficult for others.
Comprehending your body’s metabolism facilitates weight loss through informed decision-making.
The following variables affect metabolism and weight loss:
Age: As we age, our metabolism slows down. One explanation for why weight loss may become more challenging as we age.
Sex: Generally speaking, men have a faster metabolism than women. Men just have larger muscular mass than women; there is no evolutionary bias.
Muscle mass: Even while at rest, muscle burns more calories than fat. Your metabolism will be higher if you have more muscle.
Exercise level: Your metabolism is influenced by physical exercise.
Genetics: Some people are predisposed to have a quicker metabolism from birth. God bless you! They could burn calories naturally more effectively and discover that it’s simpler to keep a healthy weight.
Strategies to Increase Metabolism and Reduce Weight
Eat plenty of protein at every meal
Do a high-intensity workout
Lift heavy things
Stand up more
Drink green tea or oolong tea
Eat spicy foods
Get a good night’s sleep
Drink coffee
Drink enough water
Eat plenty of protein at every meal: For a few hours, eating can cause your metabolism to rise.
We refer to this as the thermic effect of food (TEF). The additional calories needed to break down, absorb, and assimilate the nutrients in your food are the reason.
TEF rises more when protein is present. As opposed to 5–10% for carbohydrates and 0-3% for fats, 20–30% of dietary protein’s useable energy must be used for metabolism.
Increasing protein intake can help lessen the metabolic decline that is frequently linked to fat loss. This is because a common consequence of dieting is muscle loss, which protein helps to avoid.
You can indirectly increase your metabolism by engaging in this kind of workout if it’s safe for you. In order to burn fat and gain muscle, your muscle cells will use energy when they are at rest.
For HIIT, this effect is thought to be stronger than for other forms of exercise.
Lift heavy things: Compared to fat, muscle has a higher metabolic activity. Gaining muscle can help you burn more calories every day, even when you’re not moving.
Additionally, lifting weights can help you maintain your muscle mass and prevent the metabolism from dropping while you lose weight.
Stand up more: Long periods of sitting can increase weight gain and reduce calorie expenditure, which are two reasons why excessive sitting can be harmful to your health.
Standing or stepping at work was linked to decreased cardiometabolic risk (CMR) scores, weight, body fat, waist circumference, systolic and diastolic blood pressure, fasting triglycerides, total/HDL cholesterol, and insulin, according to a 2018 review.
Nevertheless, stepping led to more significant reductions in systolic blood pressure and insulin resistance than standing.
To break up the amount of time you spend sitting down if you work a desk job, try getting up and moving around for little periods of time. Another option is to purchase a standing desk or go for walks during the day. In a 2020 study, scientists discovered that doing this led to lower blood sugar and insulin levels.
Drink green tea or oolong tea: Combining green and oolong teas with exercise may indirectly enhance fat burning by converting some of the body’s stored fat into free fatty acids.
It is believed that the teas’ effects on your gut microbiota, which enhances how your body breaks down fats for energy and turns extra energy into fat for later use, may help prevent a weight loss plateau in an indirect way.
But according to several earlier studies, these teas have little effect on metabolism. They may therefore have a minor impact or just affect a select few.
Eat spicy foods: Capsaicin, which is found in peppers, is a substance that can increase metabolism.
But a lot of folks can’t handle these spices at the levels needed to make a big difference.
One review from 2016 examined the effects of capsaicin at reasonable dosages, for example. It was estimated that consuming peppers will increase caloric expenditure by about 10 calories each meal. This might explain 1 pound (lb) or 0.5 kilogrammes (kg) of weight loss over 6.5 years for a male of average weight.
Get a good night’s sleep: Obesity risk is significantly increased when sleep deprivation occurs.
Leptin, a hormone that regulates fullness (satiety), and ghrelin, the hunger hormone, have also been demonstrated to be impacted.
This could be the cause of the frequent hunger pangs and weight loss or increase experienced by many sleep-deprived people.
In a 2019 study, researchers also discovered that sleep deprivation lasting four nights or more may marginally impair the body’s ability to metabolise fat. This rise is minor, though, and can be readily reversed with a restful night’s sleep.
Drink coffee: According to research, coffee can cause the body to produce neurotransmitters like epinephrine, which assist control how your body breaks down fat.
However, a number of variables may cause this effect to change. Caffeine, for example, was found to be more effective than skilled athletes at increasing fat burning during exercise in people who lead less active (sedentary) lifestyles.
Drink enough water: Water is essential for a healthy metabolism and can aid in weight loss.
Summary
Although altering one’s metabolic rate is not always feasible, food and exercise modifications may be beneficial.
Having a greater metabolic rate could aid in controlling weight. But it’s better to concentrate on eating a diversified diet full of nutritious foods and getting regular exercise if you’re trying to reduce weight. Spices and other foods may help increase rates in the short term, but they are not a permanent fix.
In 2016, 13 individuals who drank 250 or 500 millilitres (mL) of water had their metabolic rates measured. After 500 mL when at rest, they discovered evidence of increased fat oxidation, leading them to infer that drinking water may have an impact on metabolism. They did not discover, though, that it raised metabolic rate.
FAQ’s
What is metabolic rate?
The rate at which the body burns calories and consumes energy is referred to as the metabolic rate. The term resting metabolic rate (RMR), commonly referred to as resting energy expenditure (REE), describes how much energy the body uses when it is at rest, such as when sleeping or sitting. This is how the majority of the body’s energy is used.
What is a high metabolic rate?
Individual differences in metabolic rates make it impossible to define a high or normal metabolic rate. But the higher the rate, the faster an individual will burn the energy they consume from food, potentially lowering the chance of gaining weight.
Which foods speed up your metabolism?
Protein-rich foods like meat, dairy, and legumes are usually foods that increase your metabolism. Although a few other particular meals may also be helpful, your total dietary plan and calorie requirements are more important. The top 12 foods that increase your metabolism are discussed in further detail. Nuts, turkey, or fish are examples of protein-rich snacks that can increase fat burning if you eat them right before bed. Learn more about these and other pre-bedtime snacks.
What can increase metabolic rate?
Eating the right amount of calories, choosing protein over fat and carbs, getting enough sleep, and engaging in strength training and other forms of exercise are all factors that can raise a person’s metabolic rate.
References:
Rd, H. W. (2024, January 11). 8 ways that may speed up your metabolism. Healthline. https://www.healthline.com/nutrition/10-ways-to-boost-metabolism#eat-protein
Crna, R. N. M. (2024, May 15). How to increase your metabolism. https://www.medicalnewstoday.com/articles/323328
How to increase metabolism for weight loss | Aashirvaad. (n.d.). https://aashirvaad.com/blogs/understanding-metabolism-and-its-role-in-weight-loss-how-to-increase-metabolism.html
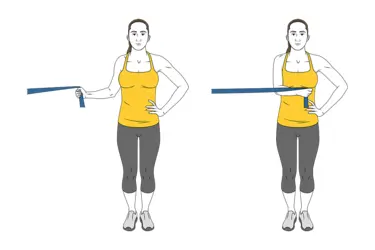
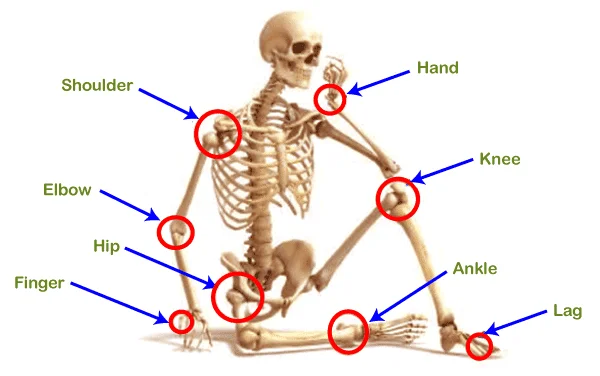
Arm muscle pain is characterized as discomfort and pain felt anywhere along the arm, sometimes extending to the wrist, elbow, and shoulder joints. There are several reasons why this pain arises, but the most frequent ones are pain or overuse.
Depending on the cause of the arm, the pain may begin suddenly, subside, or worsen over time. The RICE principle and physical therapy treatment can relieve this pain.
Causes of arm muscle pain?
Overuse:
When an arm is overexerted, moved repeatedly, and used for extended periods of time.
Numerous pain result from overusing this muscle.
Pinched nerves:
These disorders arise when a nerve exerts excessive pressure on the arm’s surrounding muscles, tendons, cartilage, and bones.
Sprains:
Sprains are caused by the ligaments and tendons stretching or rupturing.
It’s a typical pain.
Sprains are classified as mild, moderate, or severe based on their severity.
Tendonitis:
Tendon inflammation is the cause of this disease.
The wrist, elbow, and shoulder joints are affected by this tendonitis.
Mild to severe tendinitis can occur.
Rotator cuff pain:
People that execute overhead motions in their daily tasks, such baseball players and painters, are more likely to sustain this pain.
Broken bones:
When bones are damaged or fractured, the arm experiences excruciating pain.
Rheumatoid arthritis is a long-term inflammatory condition that mostly affects the joints.
Angina:
Chest pain caused by insufficient oxygen delivery to the heart.
It causes pressure in your chest, neck, or back, as well as pain in your arm and shoulder.
Symptoms of the arm muscle pain?
The cause will determine your symptoms:
You experience too much dull, stinging pain.
You are shown to have arm soreness, edema, and redness.
You experience arm muscle weakness and stiffness.
Additionally, there are trigger points and a sensitivity sensation in the painful location.
You may experience tingling and numbness in the vicinity of the pain.
Additionally, you notice a reduction in arm range of motion.
You have trouble moving your arms as well.
You may also have shortness of breath and dizziness at times.
Additionally, experiencing shooting or radiating pain when experiencing arm ache.
Diagnose of arm muscle pain?
Initially, the physician is attempting to identify the source of the pain.
Thus, the doctor is questioned about the patient’s medical history and physical examination first.
Inquire about your activities, possible pain, and symptoms as well.
The ROM is then requested to be examined by the physician.
Blood tests assist your doctor in identifying certain illnesses, such as diabetes and joint inflammation, that are caused by arm pain.
A doctor can diagnose fractured or broken bones with the use of X-rays.
Your doctor is also suggested to perform certain tests when determining whether your arm pain is related to any possible cardiac issues.
Doctors can identify issues with joints, ligaments, and tendons with the use of ultrasounds.
In order to obtain a more complete image of the soft tissues and bones for a more thorough diagnosis, your doctor may occasionally recommend MRIs and CT scans.
Nerve Conduction Study: When a tiny quantity of electrical current is given, this technique helps measure nerve impulses to identify pain nerves.
Electromyography (EMG): In order to assess electrical activity and identify damage to the nerves that supply muscles, a needle electrode is inserted into the muscles.
When is it necessary to call a doctor in an emergency?
In most cases, arm pain does not require medical attention.
While home remedies can be used to alleviate arm pain in many circumstances, there are some conditions that require emergency care.
If you experience any of the following symptoms, you need to dial 911 right away:
when you get pressure and pain in your chest.
when the upper body, neck, and back start to feel this ache.
the sensation of lightheadedness and vertigo.
when you experience dyspnea and nausea.
if the pain is too sharp or intense for you.
When you have obvious physical abnormalities, such as an angled arm or wrist joint
if you have trouble bending or turning your hands, fingers, or arms.
Which condition causes by pain in the arm muscles?
Carpal tunnel syndrome:
is a frequent ailment caused by repetitive motions of the fingers, wrists, or hands.
This causes your arms, palms, and fingers to become tingly, numb, and weak.
The tennis elbow:
is another name for lateral epicondylitis, a condition that is primarily caused by repetitive motions in the arms, elbows, and wrists. It causes pain and weakness in the elbow or forearm, as well as tenderness and trigger points on the outside of the elbow joint.
Adults between the ages of 40 and 60 are typically affected by this less prevalent ailment.
Pain and restricted range of motion (ROM) are symptoms of this illness.
This disorder is caused by thickening and inflammation of the connective tissue surrounding the shoulder joint.
Deep vein thrombosis of the upper extremity:
It happens when a blood clot forms in an arm’s deep vein, causing arm tiredness, severe pain, and swelling.
Risk factor for arm muscle pain?
Carpal tunnel syndrome is more likely to occur in women.
Carpal tunnel syndrome is more likely to occur when you have thyroid issues.
Nerve damage is another consequence of diabetes.
Being obese increases the pressure on nerves and raises the possibility of compression.
Being pregnant
Overuse of any activity
Always loosen your grip, which indicates that you should not clutch a pen, handle, or anything else more forcefully than is necessary to complete the work at hand.
Take breaks: To prevent pain, always take a little respite from repetitive activity.
Making sure your hand reaches the mouse at a comfortable angle is the first step in optimizing your computer mouse.
Treatment for arm muscle pain?
RICE principle:
A doctor is recommended to use the RICE concept as a main treatment or at-home remedy when you experience arm muscle soreness.
R-rest is reducing forearm activity, which aids in the recovery of pain tendon, ligament, muscle, bone, and nerve. You should do this sporadically rather to staying inactive for extended periods of time.
Avoid the activity until the pain has completely gone away if the person has forearm pain from sports.
I – ice To help reduce inflammation and pain, I applied ice to the affected area for 20 minutes. You can also use an ice pack and frozen peas to relieve the pain.
C-compression.
E-elevation.
Pain medication:
Your doctor may occasionally prescribe painkillers, such as anti-inflammatory drugs, if the pain does not go away.
The doctor prescribes anti-inflammatory drugs like corticosteroids to treat inflammation, which helps you lessen the underlying cause and the resulting pain.
These anti-inflammatory drugs can be taken orally, intravenously, or as injections.
Applying pain-relieving gel and spray, such as volini gel and spray, to the area of muscle soreness and swelling is another option.
Physical Therapy Treatment for arm muscle pain?
The doctor has recommended physical therapy to reduce forearm pain if the muscular soreness does not go away after home remedies and painkillers.
Massage, electrotherapy, and exercise therapy are all part of the physical therapy treatment.
Massage:
The therapist is suggested to use massage therapy to relieve muscle pain when trigger and tender points are present in the affected area.
When you are unable to relieve your muscular pain after two to three days of using the RICE method, you should have a massage.
Electrotherapy treatment:
If the RICE principle, pain medicine, and massage do not alleviate the muscle pain, electrotherapy is employed to release the pain.
Therapists are encouraged to use US (ultrasound treatment) to relieve muscle pain when trigger and tender points are present.
A pain reduction therapist applies TENS (transcutaneous electrical nerve stimulation), IFC (interferential current therapy), and SWD (short wave diathermy) to the affected muscle.
SWD, or short wave diathermy, is a type of hot therapy used to relieve muscle pain.
Gel and electrodes are used to apply TENS (transcutaneous electrical nerve stimulation) and IFT (interferential therapy) to the affected muscle area.
The area of muscle pain is treated with this therapy for ten minutes.
Exercise therapy for arm muscle pain:
The physical therapist suggests exercise treatment to alleviate muscular weakness and tightness after you feel comfortable and relieved of your muscle pain.
Stretching and strengthening exercises are part of the exercise therapy for muscle pain.
Both strengthening exercises and stretching exercises can help you release muscle weakness and tension.
Stretching exercise:
The physical therapist is instructed to stretch to relieve muscle tightness after electrotherapy has been used for two to three days to relieve muscle pain. When you feel comfortable and your pain has subsided, you apply this stretching.
Shoulder stretch
Neck release
Triceps stretching
Across-the-chest stretch
Doorway shoulder stretch
Towel stretch
The Reverse Shoulder Stretch
Shoulder stretch:
You’re standing right now.
Make an effort to elevate your shoulder joint.
For ten seconds, hold this exercise.
Next, squeeze your shoulder joints together and back.
For ten seconds, hold this exercise.
Pull your shoulder blades down as much as you can.
For ten seconds, hold this exercise.
Unwind and perform this exercise ten times.
Neck release:
You may gently relieve stress in your shoulder and neck joints with this workout.
You can do this stretching while standing or sitting.
The nape of your neck feels stretched.
To stretch your right shoulder joint, try tilting your head slightly to the left.
Repeat on the other side after holding this stretching stance for up to 30 seconds.
Stretch each side three to five times.
Triceps stretching:
You are either standing or seated.
Try raising one arm above your head and bending it such that it reaches behind your head and toward your back.
Gently press back on the bent elbow with the other hand.
Feel the tricep muscle stretch after 30 seconds of holding this exercise.
Stretch each side three to five times.
Across-the-chest stretc
Across-the-chest stretch:
You can either stand or sit as you do this stretching exercise.
Start by crossing your right arm across your chest.
Next, position the arm in the elbow joint’s crease.
Your arm is being supported by your hand.
Repeat on the other side after 30 seconds of holding this stretching stance.
Stretch each side three to five times.
Raise your arm to shoulder joint height to increase the stretch’s depth.
Doorway shoulder stretch:
Your arms and elbow joint are at a 90-degree angle as you stand close to a doorway.
Start by pressing your palms against the door frame’s sides and stepping forward with your right foot.
Make an effort to lean forward and use your core muscles.
Then put your left foot forward and repeat the stretching.
Perform this stretching exercise two or three times on each side.
Towel stretch
Towel stretch:
To begin, grasp one end of a three-foot-long towel behind your back and use your other hand to grasp the other end.
The towel is being held horizontally by you.
To stretch the affected arm, you must pull it upward with your good arm.
With your towel placed over your good shoulder joint, you are also doing a more complex variation of this exercise.
Next, use the affected arm to grasp the towel’s underside.
Using the unaffected arm, try to draw the arm toward the lower back.
Following two to three days of electrotherapy and massage to relieve muscle pain, the physical therapist recommends strengthening activities for weak muscles.
All of these strengthening exercises help with muscle soreness and weakness.
Chest expansion
Eagle arms spinal rolls
Shoulder circles
Pendulum exercise
Wand exercise
Lateral raises
External shoulder rotation
Internal shoulder rotation
Scapula Setting
Scapular Retraction/Protraction movement
Pully exercise
Finger ladder Exercises
Shoulder Roll
Chest expansion:
Chest-expansion-workout
This exercise is performed while standing.
Next, use both hands to grasp an exercise band, strap, and towel behind your back.
As you move your shoulder joints toward one another, try to widen your chest.
Next, raise your chin and gaze at the ceiling.
Hold for a maximum of 30 seconds.
Do this three to five times.
Place your hands, the towel, and the strap closer together to intensify the exercise.
Eagle arms spinal rolls:
Stretch your arms out to the sides while you are seated.
With your right arm on top, try to cross your elbow joint in front of your body.
Place the backs of your hands or forearms together and bend your elbow joint.
Next, bring your hands together by extending your right hand around.
For fifteen seconds, maintain this workout position.
As you draw your elbow joint in toward your chest during an exhale, roll your spine.
As you inhale, raise your arms and open your chest.
After a minute, repeat same exercise motion on the other side.
Do this three to five times.
Shoulder circles:
With your left hand on the back of a chair, you are standing.
Let your right hand dangle down after that.
Using your right hand, try to draw a circle five times in each direction.
On the other side, repeat this exercise.
Perform this workout three times a day.
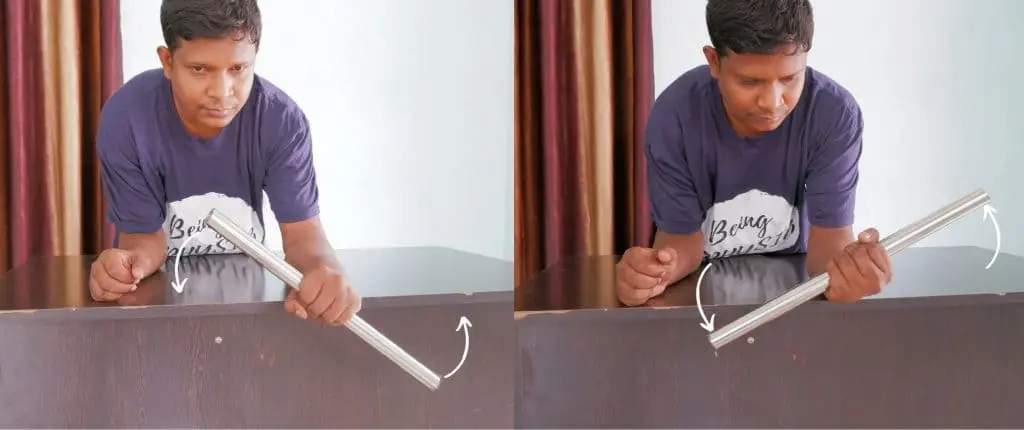
Pendulum exercise:
Pendulum Exercise
The patient is standing next to a table, with their feet somewhat wider than shoulder-width apart and their unaffected shoulder’s hand resting on the table.
Allow the affected arm to droop toward the floor while bending the hip joint to around 75 to 90 degrees.
Try shifting the weight from one side to the other while allowing your arms to swing freely.
Next, Allow the arms to swing freely from front to back while shifting the weight forward and backward.
Move the body until the arm swings in a circle after they are at ease with these motions.
Surely Don’t make the circle larger than 8 inches.
Keep going for 30 seconds.
Increase the duration to three to five minutes each day.
Wand exercise:
You can increase your range of motion with this workout.
Using both hands, you are holding the wand.
Make an effort to move your elbow and shoulder joints.
Using the wand, do the following movements: elbow flexion, extension, external and internal rotation, shoulder flexion, abduction, and adduction.
Every workout is performed two to three times a day.
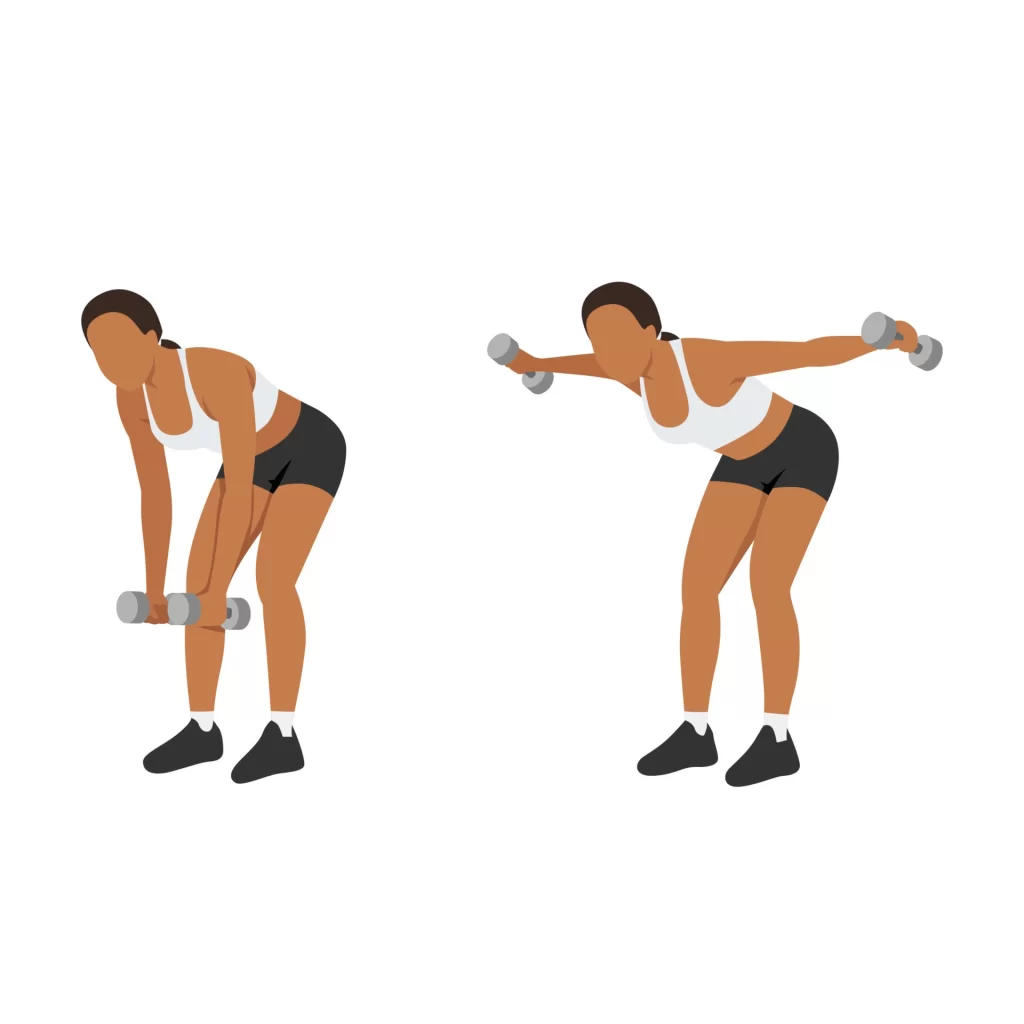
Lateral raises:
Lateral raises
For this workout, you are first holding a pair of light dumbbells.
You are standing with your feet a little wider apart than the distance between your hips.
Aim to elevate the weights to shoulder level by moving them to the sides.
It’s important to keep in mind to contract your core muscles and gradually reduce the weights to the sides.
Do this exercise three to four times a week for two sets, with each set consisting of 12 to 15 repetitions.
External shoulder rotation:
The light resistance band is first held in both hands.
Both arms must be bent at the elbow joint and kept at the sides of the body.
Next, while keeping the elbow joint bent at a 90-degree angle, rotate the opposite arm away from the body while keeping the first arm still.
After five seconds of holding this workout stance, carefully bring the arm back toward the body.
Do this exercise three to four times a week for two sets, with each set consisting of 12 to 15 repetitions.
Internal shoulder rotation:
Shoulder Internal Rotation With Resistance Band
You start by fastening a big elastic band and a resistance band to a doorknob.
One hand is used to hold the other end of this band.
Pull the forearm toward the body and attempt to bend the arm at the elbow joint.
After five seconds of holding this workout stance, carefully bring the arm back toward the body.
Do this exercise three to four times a week for two sets, with each set consisting of 12 to 15 repetitions.
Scapula Setting:
With your arms by your sides, you are in a prone position, meaning you are laying on your stomach.
For comfort, you start by placing a pillow beneath your forehead.
As much as you can, try to gently pull your shoulder joints together and down your back.
Hold this exercise for 10 seconds after easing it halfway off from this position.
Repeat this exercise ten times while relaxing in the exercise position.
Scapular Retraction/Protraction movement:
Your damaged arm is dangling over the side of a table and bed as you lie on your stomach in a prone position.
You must lift the weight gradually and maintain a straight elbow joint.
Squeeze your shoulder joint as much as you can in the opposite direction.
After then, carefully go back to where you were before and repeat the practice.
Pully exercise:
Pully exercise
You start by holding a rope pully in both hands, and then you move your shoulder.
Abduction, flexion, and internal and exterior rotation.
This workout is done three times a day and ten times in a single session.
Finger ladder Exercises:
You are facing a ladder that is suspended over a wall while you are standing.
Position the affected hands at a low position on the ladder.
Try starting the finger ladder gently, working your way up to the top, and then carefully descending back to the beginning.
This workout is done three times a day and ten times in a single session.
Shoulder Roll:
You are standing with your feet apart and your back straight.
Put your arms by your sides first.
Breathe deeply, then raise your shoulder joint to rotate it slowly.
When lifting something, try to shift your shoulder joint back so that the muscles in your shoulder joint are squeezed together.
Lower your shoulders when you exhale.
You feel a stretch around the rear of your shoulder joint when you move it forward.
What are the complications of Arm Pain?
It becomes extremely difficult to type, write, talk on the phone, and carry out your everyday tasks when you have aches and pains in your arm, shoulder, or wrist joint.
Other forms of inflammation and pain that go unnoticed and untreated might cause severe tissue damage that necessitates surgery.
How to prevent arm pain?
Always attempt to adhere to these preventative guidelines as many occurrences of arm pain can be avoided:
Always stretch your muscles, especially before working out.
Always perform the exercises with the right form, which also helps to avoid pain.
When participating in sports, make an effort to use protective gear.
Carefully and correctly lift the objects.
Conclusion
If left untreated, arm pain can worsen and lead to several consequences. Using the R.I.C.E. approach or taking anti-inflammatory drugs at home will assist a normal or minor arm pain return to normal. However, whether it may be disregarded or requires emergency medical attention depends greatly on its severity and duration.
FAQs
What is the primary line of treatment for sore arm muscles?
For the first few days following the pain, apply an ice pack or ice and water slush bath for 15 to 20 minutes at a time, repeating every two to three hours while you’re awake. compression. Apply an elastic bandage to the affected area and squeeze it until the swelling subsides.
Does a massage help with arm pain?
An arm massage stimulates the lymphatic system, improves blood circulation, and reduces swelling in order to alleviate delayed onset muscular soreness. An increase in capillarization and vasodilation during an arm massage improves blood circulation.
How can I get rid of arm pain?
Apply a cold pack or ice to your arm for ten to twenty minutes at a time. During the next three days, if you sit or lie down, support the aching arm with a pillow. Aim to maintain it higher than your heart.
Why does nighttime make arm ache worse?
Tendons and muscles may glide easily across boney surfaces thanks to bursas, which are fluid-filled sacs. The elbow and shoulder contain many bursae that are susceptible to irritation or inflammation. The pressure on the bursae may increase while you sleep on your side, which could cause throbbing arm pain at night.
Which medication works well for arm pain?
Using over-the-counter medicine is another method of treating arm pain. This does not imply that you should take it without first seeing a doctor, but after seeing you and evaluating your condition, they will probably give you some form of acetaminophen or ibuprofen to relieve your pain.
How can someone with arm pain sleep?
Put a pillow underneath the entire affected arm, including the shoulder, to avoid this. By doing this, the shoulder is raised, avoiding pain from gravity pressing on the joint. If you are a side sleeper, you must sleep on the side that is unaffected in order to prevent shoulder pain.
What vitamin helps with arm pain?
If your doctor recommends it, you might think about taking supplements if your diet isn’t providing enough niacin. Pain and stiffness caused by diseases like arthritis can be reduced when your body has the proper amount of niacin. One strategy to positively maintain your health is to include vitamins for pain in your diet.
Is pain in the arm muscles normal?
A common symptom with numerous potential explanations is arm pain. It can be a minor ache that subsides with massage and painkillers. Or it can be severe enough to interfere with your ability to carry out your daily tasks.
What is the greatest exercise for pain in the arms?
Arm workouts: Stretch, Press, and Triceps. Discover how to use this triceps press stretch to lengthen the shoulders and back of the arms. March…. Resistance Band Reverse Fly…. Resistance Band Row…. Resistance Band Triceps Extension…. Resistance Band Shadow Boxing.
Which pain reliever works best for arm pain?
Conservative treatments like acetaminophen, ibuprofen, or over-the-counter aspirin may be used as the first line of treatment. Following the directions on these over-the-counter drugs can help relieve some types of arm pain. To lessen muscle cramps, you might also think about at-home care practices like drinking lots of water.
How can arm muscle pain be relieved?
Self-care Get some rest. Take a vacation from what you usually do. Ice. Three times a day, apply an ice pack or bag of frozen peas to the aching spot for 15 to 20 minutes. compression. To reduce swelling and offer support, wrap the region with a stretchable bandage. elevation.
Does arm pain respond well to physical therapy?
Shoulder pain can be effectively relieved with physical therapy exercises. These exercises increase flexibility and range of motion in addition to easing pain. It’s crucial to collaborate with a licensed physical therapist who can create an exercise regimen tailored to your requirements and health.
Are there any forms of therapy that I can do at home?
As instructed by your doctor or therapist, you can carry out a number of therapies at home, including stretching, mild mobilizations, and elevating the affected area.
What if there is an underlying cause for my arm pain?
If this is the case, our skilled medical professionals will identify it and request that you have the necessary tests and examinations to aid in the diagnosis.
Will I receive the right care from the doctor?
Depending on the severity and underlying cause of your pain, the doctor will assess your physical condition, diagnose it, prescribe medicine, and provide appropriate treatment. In order to assist you return to your regular self, the doctor will also assign you simple physical tasks to complete.
What’s causing the ache in my arm?
There are numerous reasons for arm pain, including acute pain and underlying medical conditions like arthritis. Finding the underlying cause is crucial, and your doctor will assist you in doing so.
References
Ladva, V. (2024e, December 11). Arm muscle pain cause, symptoms, treatment, exercise | Samarpan. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/arm-muscle-pain/
Hospitals, A., & Askapollo. (2024, October 15). Arm pain. Apollo Hospitals Blog. https://www.apollohospitals.com/health-library/arm-pain/
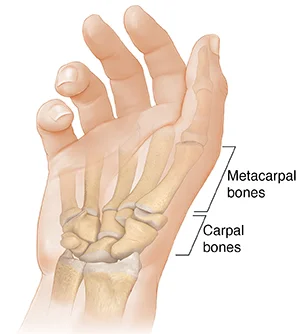
The carpometacarpal (CMC) joints are the articulations that connect the hand’s carpal (carpals) and metacarpal (metacarpals) bones. Five carpometacarpal joints are known to exist, with the thumb’s carpometacarpal joint—also referred to as the trapeziometacarpal joint—being the most specialized and flexible.
Introduction
The proximal bases of the five metacarpal bones and the distal row of carpal bones are joined by the carpometacarpal (CMC) joints, which are five wrist joints. Another name for the thumb’s CMC joint is the trapeziometacarpal (TMC) joint.
The carpal (carpo-) and metacarpal (-metacarpal) bones of the hand are joined by the carpometacarpal (CMC) joints. The thumb’s carpometacarpal joint, also known as the trapeziometacarpal joint, is the most specialized and adaptable of the five CMC joints.
Metacarpals 2, 3, 4, and 5 on the medial side and the distal row of carpal bones (trapezium, trapezoid, capitate, and hamate) on the distal side are connected by the four functional plane synovial joints that make up the remaining CMC joints. The three most medial CMC joints combine to form the common carpometacarpal joint.
The ranges of motion of the four CMC joints increase with medial movement; metacarpals 2 and 3 are nearly stationary, metacarpal 4 glides to a limited degree, and metacarpal 5 glides to the point where it produces flexion and rotation. The medial four CMC joints are exceptionally robust due to these properties, which enable a firm hold between the wrist and hand while also allowing for flexibility to support opposing movements such as palm cupping and thumb object grasping.
The CMC joints’ mobility increases from the radial to the ulnar sides of the hand as their articular surfaces grow increasingly curved.CMC joints total five in number. From the trapezium to the first metacarpal base is the first CMC joint. The second metacarpal base and the trapezoid are separated by the second CMC joint.
First Carpometacarpal Joint
The thumb (pollex) carpometacarpal joint, also referred to as the trapeziometacarpal joint (TMC), is the first carpometacarpal joint. It is necessary for the thumb’s proper function and serves as a link between the trapezium and the first metacarpal bone.
The prevalence of TMC osteoarthritis, a severely incapacitating condition, is up to 20 times higher in older women than in the overall population. The TMC is the most essential joint connecting the wrist to the metacarpus.
The pronation-supination of the first metacarpal is particularly crucial for opposition action. The capsulo-ligamentous complex surrounding the joint, the form of the joint, and the balance of the participating muscles limit the first CMC’s range of motion. First CMC joint subluxation (slight displacement) towards the radius is common if the first metacarpal does not sit correctly “on the saddle,” as in the case of hypoplasia.
Although the capsule reinforces ligaments and tendons to give joint stability, it is sufficiently slack to permit a wide range of motion and a 3 mm distraction. On the dorsal side compared to the ventral side, it is marginally thicker. Most postmenopausal women have osteoarthritis of the first carpometacarpal joint.
Type
Concavoconvex articular surfaces give rise to saddle type of synovial joints.
Articular Surfaces
The trapezium’s distal surfaces
first metacarpal bone’s proximal portion.
Concave in the sagittal plane and convex in the frontal plane are the articulating surfaces of trapeziums.
The articular surfaces’ concavoconvexity permits a broad range of motion.
Ligaments
There are significant differences in the anatomical literature on the number and nomenclature of the first CMC’s ligaments. The thumb is stabilized primarily by three intracapsular and two extracapsular ligaments.
Anterior oblique ligament (AOL)
A robust, thick intracapsular ligament that begins on the palmar tubercle of the trapezium and terminates on the palmar tubercle of the first metacarpal. According to certain reports, it has a significant retention function and is either absent or extended in CMC joint arthritis. Abduction, extension, and pronation all exhibit rigidity.
Ulnar collateral ligament (UCL)
An extracapsular ligament that extends nearly to the AOL is called the UCL. It is placed on the ulnopalmar tubercle of the first metacarpal after starting on the flexor retinaculum. It is often extended when CMC joint arthritis is present and is taut in abduction, extension, and pronation. Researchers differ widely about the UCL’s significance.
First intermetacarpal ligament(IML)
This ligament attaches to the ulnopalmar tubercle of the first metacarpal, where its fibers converge with those of the UCL, and joins the bases of the second and first metacarpals. It is taut during opposition, abduction, and supination.
It was the primary restraining structure of the original CMC joint, according to several researchers. Although some people think it isn’t strong enough to maintain the joint by itself, when paired with the UCL, it serves as a crucial restraining component.
Posterior oblique ligament (POL)
An intracapsular ligament called the posterior oblique ligament (POL) connects the dorsal side of the trapezium to the ulnar-palmar tubercle of the first metacarpal. Although it tightens during forceful adduction and radial abduction, it is not a crucial ligament for the first CMC joint.
Dorsoradial ligament (DRL)
Similar to the previous ligament, the DRL has no bearing on the initial CMC. The trapezium’s dorsal and first metacarpal sides have a connection it.
Relations
Anteriorly: The joint is protected by the thenar eminence muscles.
Posterior: The long and short extensors of the thumb are situated
Medially: the radial artery and the first dorsal interosseous muscles
The thumb pulp moves over the palm to get closer to the digit pulps. When the thumb is simultaneously abducted, flexed, and pronated, opposition is created.
Retroposition
In both ulnar adduction and extension, the thumb pulp is raised. extensor pollicis longus
Circumduction
Circumduction is the result of extension, abduction, flexion, and abduction occurring one after the other (or the opposite).
Circumduction, opposition, abduction, and adduction in a plane perpendicular to the palm, and flexion and extension in the palm’s plane are all allowed. The movement of opposition causes the thumb’s tip to make contact with the volar surfaces of the slightly bent fingers. A modest sloping facet on the anterior lip of the saddle-shaped articular surface of the greater multangular allows for this mobility. The Adductor muscles carry out the opposite movement, while the Flexor muscles pull the matching portion of the metacarpal bone’s articular surface onto this facet.
With help from the Opponens pollicis and Adductor pollicis, the Flexores pollicis longus and brevis bring this joint into flexion. The extension is mostly accomplished by the abductor pollicis longus, with support from the extensor pollicis longus and brevis. The Adductor is responsible for adduction, while the Abductores pollicis longus and brevis, with the help of the Extensors, are principally responsible for abduction.
Joint Capsule
There is a distinct synovial membrane surrounding the fibrous joint capsule.
Arterial supply
The anterior interosseous artery and the posterior carpal branches of the radial and ulnar arteries supply blood to the carpal joints.
The radial artery’s dorsal metacarpal branch.
Innervation
Lateral antebrachial cutaneous nerve Palmar cutaneous branch of the median nerve. Superficial radial nerve
Second to fifth carpometacarpal joints
Articular surfaces
The CMC joints connect the surfaces of the metacarpal bases of the medial four metacarpal bones to the distal surfaces of the four distal carpal bones.
The second metacarpal bone, trapezium, trapezoid, and capitate appoint to form the second CMC joint. A flat, quadrilateral bony protrusion (facet) that links to another quadrilateral facet on the base of the second metacarpal is directed medially by the distal part of the trapezium. The trapezoid’s distal surface is triangular and concave coronally, ‘cupping’ a concave groove on the base of the second metacarpal. It is convex in the transverse plane. The concave, anterolateral corner of the capitate bone is articulated with a deep ridge situated medially to this groove. The second CMC joint is unique in these features since it is the only one in which the articulation is formed by three carpal bones.
The third metacarpal bone and the capitate make up the third CMC joint. The triangular and primarily concave distal aspect of the capitate articulates with a convex facet on the metacarpal base.
Together with the hamate and fourth metacarpal bones, the capitate bone contributes to the formation of the fourth CMC joint. This capitate’s anteromedial corner develops an articulating facet in the direction of a sizable, oval dorsal facet on the base of the fourth metacarpal. On the distal aspect of the hamate bone, a tiny, anterolateral facet meets the somewhat convex and concave quadrangular proximal surface of the metacarpal base.
The fifth CMC joint is formed in part by the fifth metacarpal bone and the adjacent bigger, anteromedial facet on the same distal surface of the hamate. This metacarpal base gets attached to the hamate by a laterobasal surface that is coronally convex and transversely concave. This transition from concave to convex is not sharp; rather, it slopes almost smoothly downward. The articular surface of the hamate bone has a beveled edge that allows the fifth CMC joint to move more freely than the other CMC joints.
The four CMC joints are flat (non-planar) based on the specifications given above. Certain surfaces can be concave, convex, or both, but some are nearly flat. Certain surfaces can be concave, convex, or both, but some are nearly flat. They therefore resemble sophisticated saddle synovial joints or ellipsoid joints physically. The CMC joints are functionally classified as plane synovial joints because of their tiny curvatures, which are typically ignored.
Ligaments
The dorsal carpometacarpal ligaments, palmar carpometacarpal ligaments, and interosseous ligaments are the three types of ligaments that connect the CMC joints. The fibrous joint capsule that envelops the CMC joints thickens to form these soft tissue formations.
Dorsal carpometacarpal ligaments
The CMC joints are largely supported by the strongest ligaments, the dorsal carpometacarpal ligaments, which are situated on the dorsal side of the hand. They consist of four medial metacarpal bases and seven ligamentous bands that extend obliquely between the dorsal surfaces of the distal row of carpal bones.
Both metacarpals 2, 3, and 4 are given two bands: the capitate and hamate for metacarpal 4, the trapezium and trapezoid for metacarpal 2, and the trapezoid and capitate for metacarpal 3.The fifth metacarpal is unique in that the hamate bone only gives it one ligamentous band. The equivalent palmar carpometacarpal ligament is connected to this band to produce an incomplete capsule.
Palmar carpometacarpal ligaments
Palmar carpometacarpal ligaments are found on the palmar portion of the hand and resemble their dorsal counterparts in many ways. With three ligamentous bands—one medial from the hamate, one intermediate from the capitate, and one lateral from the trapezium/trapezoid—the third metacarpal base is the only exception.
Interosseous ligaments
The CMC joints’ smallest stabilizers are the interosseous ligaments. These structures separate the third and fourth metacarpal bases and the inferior portion of the capitate and hamate bones’ distal edges by two thick, fibrous bands.
These bands may be joined proximally or entirely. The capitate and the third metacarpal base are connected by the lateral band and the fourth metacarpal base by the medial band, respectively, if they are separated. The CMC joint space can also occasionally be separated into medial and lateral compartments by the medial interosseous ligament, which forms a distinct synovial cavity between the hamate and the fourth and fifth metacarpal bones.
Movement
The four CMC joints are all synovial based on their structural composition. Their functional classification, degrees of freedom, ranges of motion (ROM), and articular surfaces, however, separate them into two groups. The latter gradually rises as one moves medially over the four CMC joints.
The range of motion of the second to fifth carpometacarpal joints increases from the radial to the ulnar side. Small gliding motions are produced at these joints by the contraction of the long flexor and extensor digitorum muscles. The opponens digiti minimi can contract to induce flexion and lateral rotation at the fifth carpometacarpal joint, which makes it possible to do palm “cupping.”
Muscles acting
There is no direct muscle activity required to move the four medial CMC joints. The muscles that affect joint translational movements, however, are the flexor digitorum profundus and extensor digitorum. The fourth and fifth CMC joints experience flexion and extension, respectively, as a result of the indirect gliding action of these antagonistic muscles on the phalanges.
The isolated exception is the opponent’s digit minimise direct participation in the fifth CMC joint’s rotating movement. The muscle brings the fifth finger to the palm when it is in an agonistic position, externally rotating it and hollowing the palm. Adductor pollicis, opponens pollicis, flexor pollicis brevis, and abductor pollicis brevis are the muscles that oppose and smoothly govern the opponens digiti minimi. Together, the flexor digiti minimi, abductor digiti minimi, and palmaris brevis support the joint when moving.
Several soft tissue structures are connected to the four medial CMC joints. The flexor digitorum superficialis, flexor digitorum profundus, flexor carpi radialis (lateral), and flexor carpi ulnaris (medially) are among the muscles whose tendons cover the CMC joints on the palmar aspect of the hand. Additionally, the hypothenar muscles cover the medial CMC joints superficially.
On the dorsal side of the hand, near the tendons of the extensor forearm muscles, are the CMC joints. Extensor carpi ulnaris, extensor pollicis longus, extensor digitorum, extensor digiti minimi, extensor carpi radialis longus, and extensor carpi radialis brevis are a few examples.
Joint capsule
A shared fibrous capsule envelops and stabilizes the four CMC joints. A synovial membrane that lines this fibrous capsule secretes viscous synovial fluid, which serves as a lubricant. The synovial membrane is normally continuous with the lining of the intercarpal joints.
The midcarpal and intermetacarpal joint spaces are connected to the proximal and distal extensions of the joint cavity of the CMC joints, respectively. CMC joints are lined with hyaline cartilage on their articular surfaces.
Arterial supply
Posterior carpal branch of the radial artery
Posterior carpal branch of the ulnar artery
Anterior interosseous artery
Innervation
Dorsal ulnar nerve
Anterior interosseous nerve
Superficial radial nerve
Blood supply of carpometacarpal joints
The palmar and dorsal carpal anastomotic arches give blood to the CMC joints. These are created when the radial artery’s palmar and dorsal carpal branches unite.
Synovial membranesof carpometacarpal joints
The intercarpal joints’ membrane continues onto the synovial membrane. There are instances where the hamate and the fourth and fifth metacarpal bones form a joint with a distinct synovial membrane.
There are five synovial membranes in the wrist and carpus, as may be seen:
The lower end of the ulnar muscle connects to the ulnar notch of the radius muscle, and it runs along the upper surface of the articular disk.
The second connects the first row of bones below to the articular disk and the lower end of the radius above.
The third, and longest, connects the contiguous margins of the two rows of carpal bones. If an interosseous ligament is missing, it can also connect the second row’s bones to the carpal extremities of the second, third, fourth, and fifth metacarpal bones.
Starting from the edge of the larger multangular, the fourth one reaches the thumb’s metacarpal bone.
The fifth connects the pisiform and triangle bones’ neighboring edges.
Occasionally, there is a distinct synovial membrane at the fourth and fifth carpometacarpal joints.
For the wrist and carpal joints to operate smoothly and to be lubricated, these synovial membranes are essential.
Clinical significance
The degeneration of both the joint cartilage and the underlying bone is a defining feature of osteoarthritis of the carpometacarpal joints. In particular, it is called trapeziometacarpal osteoarthritis when it involves the thumb.
The development of a tiny, fixed projection over the joint is known as carpometacarpal bossing. The formation of an immovable prominence in the carpometacarpal area is referred to by this word.
The affected joints may experience pain, stiffness, and decreased mobility as a result of these diseases, which frequently influence daily activities and hand function.
Summary
The distal row of carpal bones and the proximal bases of five metacarpal bones are joined by the carpometacarpal (CMC) joints, which are five wrist joints. The trapeziometacarpal (TMC) joint, the first CMC joint, is more common in older women and is necessary for appropriate thumb function.
The first dorsal interosseous muscles, the radial artery, the long and short extensors of the thumb, the thenar eminence, and two extracapsular ligaments are all covered by the first CMC joint. Three types of carpometacarpal ligaments—dorsal, palmar, and interosseous—maintain the stability of the CMC joints.
Despite having synovial motion, the CMC joints are classified into two categories based on their articular surfaces, degrees of freedom, and ranges of motion. The flexor digitorum profundus and extensor digitorum muscles have an indirect effect on the four medial CMC joints. On the dorsal part of the hand, near the tendons of the extensor forearm muscles, are the CMC joints.
FAQs
The most movable carpometacarpal joint is which one?
The thumb’s carpometacarpal joint (pollex), also known as the first carpometacarpal joint or the trapeziometacarpal joint (TMC), is an essential component of the thumb’s normal function because it connects the trapezium to the first metacarpal bone.
At what types of movements does the carpometacarpal joint move?
The CMC joint can move in all directions, including flexion, extension, adduction, and abduction. When combined, these motions enable intricate thumb actions like adduction, palmar and radial abduction, opposition, and retropulsion.
Where is joint discomfort associated with CMC?
The base of the thumb hurts as a result of the wear and tear on that CMC joint in particular.
What is the CMC’s weakness?
A frequent degenerative illness that significantly impairs function and causes morbidity is osteoarthritis of the thumb carpometacarpal (CMC) joint. Hand weakness is common in patients with early-stage CMC OA when they pinch, grab, or twist objects.
How big is the carpometacarpal joint?
Due to its small stature, the carpometacarpal joint is suitable for code 20600, Arthrocentesis, aspiration, and/or injection, small joint or bursa (e.g., fingers, toes); without ultrasound guidance.
Is the carpometacarpal a saddle joint?
A wide range of motion (ROM) is made possible by the thumb’s carpometacarpal (CMC), a saddle joint that is primarily responsible for the typical agility of human comprehension. Throughout life, this joint, which is found at the very base of the thumb, is consistently under a lot of physical strain.
References:
Vaghela, D. (2023, December 13). Carpometacarpal Joint – Anatomy, Structure, Function. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/carpometacarpal-joint/
January 21, 2024: Goswami, K. Carpometacarpal joints (CMC joints): All the Information You Need. Physiotherapy Clinic of Samarpan. CMC joints: https://samarpanphysioclinic.com/carpometacarpal-joints/
Carpometacarpal (CMC) joints. (2023, July 5). Kenhub. https://www.kenhub.com/en/library/anatomy/carpometacarpal-cmc-joints
Wikipedia contributors. (2024a, May 22). Carpometacarpal joint. Wikipedia. https://en.wikipedia.org/wiki/Carpometacarpal_joint
Gracilis muscle pain refers to discomfort or soreness in the long, slender muscle located in the inner thigh. This pain is often caused by overuse, strain, or injury from activities involving repetitive leg movements, such as running or cycling.
It may result in inner thigh stiffness, soreness, and difficulty with leg motion, requiring proper diagnosis and management for effective relief.
What is the Gracilis muscle pain?
Pain where the inside of the upper thigh and the belly meet is known as gracilis muscle pain.
However, there are other reasons of groin pain besides muscle pain, and the way that gracilis pain is experienced can differ. The symptoms and underlying cause of the pain, as well as whether the pain is experienced by a child or an adult, male or female, will determine the diagnosis and course of treatment.
Anatomy of the Gracilis muscle.
Origin: inferior ischiopubic ramus
Insertion: The gracilis muscle attaches to the medial tibia at the pes anserinus after descending nearly vertically down the leg.
Nerve supply: obturator nerve (L2-L4)
Blood supply: medial circumflex femoral artery
Gracilis’ action
Adduction around the hip joint and weak thigh flexion only serve to support the other, stronger thigh adductors.
Common causes of Gracilis muscle pain
It’s likely that an pain to a muscle or the cartilage connecting the bones in your hip joints is the cause of your Gracilis muscle pain, especially if it gets worse when you walk.
Conditions affecting the organs and tissues in the belly and groin may also be the cause of gracilis muscle pain that gets worse when you walk.
Following an accident, groin pain may start right away or develop gradually over the course of weeks or even months. Continued use of the damaged area may exacerbate groin pain.
Despite the fact that groin and testicular pain are distinct, a testicle issue can occasionally result in pain that radiates to the groin region.
The following are some direct and indirect causes of gracilis pain:
Bone tissue loss from avascular necrosis or osteonecrosis caused by insufficient blood supply:
Avulsion fracture:
inflammation of the bursitis joint:
Labral tear in the hip:
While some people may not experience any pain or discomfort, others may have the following:
hip and groin pain that worsens with walking or prolonged sitting or standing.
Epididymitis:
One or both testicles may become inflamed as a result of epididymitis.
Hip impingement
Hip impingement is a painful ailment that can arise when the ball and socket in the hip joint do not fit and move together smoothly. A different name for it is femoroacetabular impingement.
When the ball bends over, it may jam in the hip socket if it is malformed.
An improperly formed hip socket or one with an additional bone may also be the cause of this condition. This may make it more difficult for the femur’s ball to glide smoothly inside the hip socket.
Problems with hip impingement can result in groin pain and stiffness, particularly when walking or bending forward at the hip. Osteoarthritis may also result from it.
Hydrocele
Inguinal hernia
Groin pain from an inguinal hernia may get worse as you move, bend, raise, or cough. Additional symptoms include a protrusion in the groin area that enlarges when you cough or stand up.
Pain or redness around the bulge
Scrotal swelling, fever, nausea, and vomiting.
Kidney stones:
Hard, crystal-like stones that are generated from mineral deposits make up kidney stones. Until they reach the point where the kidney and ureter meet and beyond, these stones frequently don’t produce any symptoms. One side of the abdomen or low back may experience pain, which can be quite severe. The groin may experience further radiating pain.
Mumps
Gracilis strain
During preparation and competition, these sports necessitate an eccentric contraction of the gracilismus culature. A muscle or tendon strain at the point where the Gracilis muscle tendon attaches to the bone is typically the underlying ailment.
Gracilis strain symptoms also include:
bruises close to the affected muscle edema, decreased strength in the upper leg.
Orchitis (inflamed testicle)
Osteoarthritis
Over time, osteoarthritis may result from the cartilage in the hip and other joints wearing down due to wear and tear. The ends of the bones in a joint no longer move smoothly when the cartilage has been severely eroded.
When they stand, move, or climb stairs, it may feel worse. If you are sleeping, the pain could feel pleasant.
When you move, you might also experience a clicking or grinding sound in your hip. On the same side of the body as the affected hip, you could also experience referred pain over the lower leg and knee.
Pinched nerve
Piriformis syndrome
Tendinitis
Any tendon may experience it, and the pain typically begins as a dull ache surrounding the affected area.
If you frequently do the same motions when exercising, playing sports, or doing your job, you run a higher danger.
Pain from hip tendonitis typically develops gradually. Walking or other physical exertion tends to make it worse, while resting helps it feel better.
Urinary tract infection (UTI):
In women, it is more widespread. A change in the frequency or urgency of urination, as well as pain or burning when peeing, are possible symptoms in addition to groin pain.
Strained round ligament:
It extends to make room for the growing uterus during pregnancy, and walking can cause strain and pain.
They are usually painless, but if the cyst gets bigger, symptoms may show up. Abdominal bloating, uncomfortable bowel movements, and groin or lower back pain are some of the symptoms.
Testicular cancer:
This cancer frequently results in a painless bump on the testicle. But it hurts sometimes. This type of cancer is uncommon. It is nearly usually treated and cured if detected early.
Prostatitis:
The prostate gland is swollen or infected. You can get pain and difficulty urinating.
Consult your physician. Sometimes prostatitis resolves on its own. However, you might need to take medicines if it’s an infection.
Gracilis muscle of this pain:
Grade 1: neither strength nor function is lost. On US and MRI imaging, muscle tears may seem normal or may show a small portion of localized disruption (less than 5% of the muscle volume), with hematoma and perifascial fluid appearing relatively universal.
Grade 2: severe, somewhat feeble. If the athlete tries to continue the activity after suffering an acute grade 1 or 2 strain of the adductor muscle, they will experience severe groin pain that feels like a sharp knife stab. A few days following the pain, a hemorrhage and swelling are typically seen. Localized pain, trouble contracting the hip abductors, and a typical trauma history.
Grade 3: severe loss of function and full muscular breakdown. The distal musculotendinous junction, which is situated at the femur’s insertion, is where complete muscle rips or grade 3 strains are most frequently discovered.
Symptoms of gracilis muscle pain?
People who have gracilis muscle pain typically feel pain in the top 1/3 of the gracilis muscle region, high in the groin. However, the painful area may become less localized to the original injury or pain site if the pain has persisted for a long time. It may spread into the lower abdomen and across the pubic area. On occasion, it may also spread to the opposite leg’s gracilis area.
Walking
On one leg
Standing on the damaged leg and turning or changing direction
Sneezing or coughing
Enhanced pain when touched
Usually, there is little to no pain when at rest or when engaging in everyday low-level tasks if the pain is less severe or has been present for a long time. Typically, pain occurs with more demanding or dynamic tasks like:
Particularly when accelerating or decelerating, running
Kicking
Bounding and Hopping
Side lunges or deep split lunges
After the acute pain subsides, athletes with gracilis pain can frequently resume their sport, although they may find it difficult to perform at their best because of pain or diminished strength.
Which disease requires you to call a doctor?
if the leg is immfobile.
if the leg is unable to support the weight.
Diagnose of gracilis muscle pain?
Medical intervention is not necessary for the majority of gracilis muscle pain situations. However, if you have significant, ongoing pain along with fever or swelling, you may want to consult a doctor.
Your healthcare professional may diagnose gracilis muscle pain in a variety of methods due to the wide range of potential reasons.
In addition to assessing the symptoms, the doctor will inquire about any recent physical activity. After that, they will examine the groin area physically and run more tests if needed.
Your doctor will inquire about your medical history and additional information regarding your gracilis pain, including:
When it started:
Whether you were hurt
What exacerbates and alleviates the pain
If you experience any further symptoms
Usually, a physical examination is required. Imaging studies can also be necessary to confirm the diagnosis.
Physical Examination
During the physical examination, the physician will:
An examination of the abdomen
If he were male at birth, a testicular examination
A neurological examination
A hip-focused musculoskeletal examination
People who have hip joint issues also experience pain when they bend and rotate their hip joints. Sitting with your ankle resting on your thigh is an example of this kind of motion.
Hernia test
Your doctor will ask you to cough after sticking one finger into the scrotum, which is the sac that houses the testicles. Coughing forces the intestines into the hernia opening and increases abdominal pressure.
The physical examination is sufficient to detect a gracilis muscle strain. However, imaging is typically required for other causes of groin pain.
X-ray: The doctor can use X-rays to determine whether the gracilis pain is due to a bone fracture. Gracilis pain is frequently diagnosed with X-rays. This imaging exam takes pictures of the body’s interior structures. In this instance, the hip joint’s bone structure and anatomy may be seen on the X-ray.
The best technique to view the cartilage pain area is with X-rays. They may also exhibit joint space narrowing and bone spurs, which are further symptoms of hip osteoarthritis.
The doctor could prescribe an ultrasound if your groin pain seems to be caused by an inguinal hernia or the testicles. Sound waves are used in ultrasounds to produce an image of the interior organs.
A computed tomography (CT) scan may be used by the medical professional if a kidney stone is suspected. A CT creates a three-dimensional image by combining many X-rays.
Intestinal issues or other disorders of the abdomen and pelvis can also be diagnosed by ultrasound and CT scans.
The soft tissue surrounding the hip joint is also examined using a magnetic resonance imaging (MRI) test.
Contrast is occasionally used during an MRI. You will receive an injection of a particular kind of dye throughout this process. This makes minor damage to the labrum and cartilage inside the joint appear more clearly on the scan.
An MRI is frequently used to check for nerve issues. For instance, a pinched nerve in the back may occasionally indicate groin pain. This implies that even though the pain is elsewhere, the pain may seem to be emanating from the groin.
An MRI can assist in determining the actual cause of the pain in a situation like this.
Differential Diagnosis
Gracilis pain has always been regarded as complicated, with several definitions and terminologies and no established diagnostic standards. The complexity of groin strain in athletes is increased by the fact that over 30 different diagnostic terms were used to characterize gracilis pain in a systematic review on the treatment of groin pain in sports.
During the Doha accord meeting, a classification scheme for groin pain was explained in three primary subheadings:
The RICE principle is applied in the initial stages of pain management.
R-rest = keep away of actions that could exacerbate pain and pain when it occurs. Therefore, either take a short break or limit activities that involve the adductor longus muscle, such as jogging and walking.
I-ice = 20 minutes of ice applied to the painful location, followed by its release to reduce pain and swelling. Additionally, you can use frozen peas and ice packs.
C-compression: Used on compression bandages to relieve spasms and edema.
E-elevation: To reduce edema, the patient is raised to the affected leg using a pillow.
In most cases, non-operative therapy works and should be pursued for several months. Surgery may be recommended, though, if symptoms and a notable performance limitation continue following a suitable conservative treatment plan. One method that has been proposed to alleviate symptoms is adductor tenotomy.
Athletes who underwent surgery had a quicker return to play (RTP) time, according to a new systematic study that contrasted conservative and surgical treatments. However, the meta-analysis’s lack of high-quality randomized control trials (RCTs) and the variety of surgical procedures make it impracticable to suggest surgery.
Medical treatment:
Patients can utilize painkillers like NSAIDs (nonsteroidal anti-inflammatory medicines), which include ibuprofen and naproxen, when they experience muscle pain.
In order to lessen the pain in the affected area, the patient can also apply pain reliever gel or patches, such as volini gel or diclofenac gel.
Heating therapy:
When the swelling has subsided after two to three days of muscle soreness, apply heat using a heating pad and a warm water bottle until the patient’s groin area feels comfortable.
Grcilis strain treatment:
Treatment for Gracilis strains varies by grade.
Acetaminophen and non-steroidal anti-inflammatory drugs are typically used to treat groin strain pain in the initial stages.
The RICE principle can also be applied to pain management.
From mild to more severe strains, recovery takes longer and requires rest for three to six weeks.
A full tear indicates three degrees of strain, necessitating surgery and a recuperation period of up to three months.
When there is an emergency with gracilis pain:
abrupt onset and excruciating pain
nausea, vomiting, fever, or chills caused by the pain
Surgery: Surgery can treat more serious bone fractures and muscle rips as well as other issues like a hernia that can be causing the pain.
Physical Therapy Treatment for gracilis muscle pain?
Electrotherapy, stretching, and exercise are all part of the physical therapy treatment to relieve muscle pain.
Electrotherapy for the gracilis muscle pain:
SWD, TENS, IFT, and the US machine—which reduces pain and swelling—are all part of this electrotherapy treatment.
Ultrasound therapy: To lessen edema, a US machine is used to the trigger and tender points.
To alleviate muscle pain, short wave diathermy, or SWD, is applied to the affected area.
To relieve pain and edema in the affected area, TENS and IFT machines are utilized.
After their strength returns to normal, they move on to more demanding and strengthening exercises.
Gracilis muscle stretching exercise
The groin, or inner leg muscles, are involved in the gracilis. The group of muscles with a notably big muscle mass will be included in the Gracilis muscle stretch. In games like soccer, where the inside of the foot is used to kick a soccer ball, these muscles are more beneficial. Lastly, they are used for thigh flexion and extension when sprinting or against resistance.
Lunge Stretch
Standing Lateral Lunge gracilis Stretch
Butterfly Stretch
Half-kneeling adductor dips
Supine Wall Stretch
Standing Gracilis Stretch
Kneeling Gracilis stretch
Gracilis AIS Release
Frogger stretch
Lateral squat
Crossover stretch
Seated Gracilis Stretch
Reclining angle bound pose
Standing banded adduction
Hip Opener and Groin Stretch
Runner’s Lunge
Squatting Groin Stretch
Frog Squat With Arm Raise
Lunge Stretch
Lunge-Stretch
How to perform stretch:
Start by assuming a lunge position while kneeling on the ground.
For five to ten seconds, hold this adductor stretch, then let go.
Do ten to twelve repetitions.
Standing Lateral Lunge Gracilis Stretch
How to perform stretch:
Take a wide stance when standing.
while performing the stretch, keep your posterior pelvic tilt.
Holding time can be improved in progression.
Perform this adductor stretch four or five times.
Butterfly Stretch
Butterfly Stretch
How to perform stretch:
Grab your left foot by reaching forward.
To aid with the hand-foot joint, you can bend your knee.
Pull your left foot slowly up toward your groin, bending it until the sole is toward your right thigh and it feels comfortable.
Let your knees drop toward the floor while keeping your back upright.
By applying moderate pressure to the knees with the elbows, you can provide mild pressure to the inner thigh.
You may experience stiffness and tugging in your groin.
For twenty to thirty seconds, hold the butterfly pose.
Release and repeat two or three times.
Half-kneeling adductor dips
How to perform stretch:
Half-kneeling dips for the adductor
As much as possible, extend the left leg to the side.
It’s possible that your foot and knee are at right angles.
The inside thigh, particularly the right side, is where you may feel the strain.
Do this eight to ten times.
Supine Wall Stretch
Supine Wall Stretch
How to perform stretch:
having one leg propped up against a wall while lying supine in front of it.
As you go closer to the wall, keep your hamstrings at a comfortable length.
As they gradually split open, keep your leg straight until you feel the inside side of it expand.
Unwind and repeat three times.
Kneeling Gracilis stretch
How to perform stretch:
The left inner thigh is where you may feel the stretch.
After 8–10 seconds of pause, release the stretch and return to it.
Do this eight to ten times.
Gracilis AIS Release
How to perform stretch:
Put a resistance strap around one foot and start in a supine position.
The foot is then actively slid sideways.
Avoid raising the foot as this may cause the hip flexors to contract.
Instead, slip the foot.
Using the resistance strap, slowly pull the foot farther outward toward the end of the exercise.
You can feel your adductors getting stretched.
After five to ten seconds of holding the stretch, slide back.
Do 8–10 repetitions.
Frogger stretch
Frogger stretch
How to perform stretch:
Feel the strain on the inner thighs as you sit the butt back to the heels.
After ten to fifteen seconds of pause, release the stretch and return to it.
Do this eight to ten times.
Lateral squat
How to perform stretch:
While maintaining a straight right leg, lower yourself as much as you can.
Before going back to the starting position, take a breath and hold it for 15 to 20 seconds.
Crossover Stretch
Crossover Stretch
Since this motion is similar to the “grapevine” dance move, it may come readily to you if you enjoy dancing.
How to perform stretch:
Put both feet together.
Bring your left foot to join your right foot and take another step to the right with your right foot.
Repeat on the other side after both feet are together.
You can begin slowly and increase your pace as you become accustomed to the movement. Five to ten times.
Seated Gracilis Stretch
How to perform stretch:
Make a “V” shape with the legs straight out to the side.
Sitting like this is sufficient for many people to extend their inner thighs.
Lean your hips toward the floor while maintaining a straight back for greater flexibility.
Hold there for ten to fifteen seconds. Breathe normally.
Reclining angle bound pose
If you sit for the majority of the day, this is the ideal stretch.
How to perform stretch:
Draw your soles inward and bend both knees so that their borders meet.
To feel the groin muscles stretching, lower your knees toward the floor.
Do this three or four times. With each stretch, attempt to bring the feet closer to the buttocks.
Squatting Groin Stretch
Squatting Groin Stretch
How to perform stretch:
Squat down gradually until your knees are exactly over your ankles, then bend to a 90-degree angle.
The inner side of each leg will feel stretched.
Hip Opener and Groin Stretch
How to perform stretch:
Drop your right knee to the floor and start in a forward lunge position.
As seen in the illustration, place the left elbow on the inside of your left knee.
After holding the stretch for 20 to 30 seconds, let go and repeat with the right leg.
Runner’s Lunge
Runner’s Lunge
How to perform stretch:
With your right leg extended behind you and the knee resting or slightly raised, plant your fingertips gently into the floor.
Keep your head up.
With each inhalation and exhalation, push your hips farther into the floor.
Proceed to the opposite sides after that.
Squatting Groin Stretch
How to perform stretch:
Squat down gradually until your knees are exactly over your ankles, then bend to a 90-degree angle.
The inner side of each leg will feel stretched.
Frog Squat With Arm Raise
How to perform stretch:
As you stretch the left hand straight up to the roof, fingers pointing upward, keep pushing your inner thigh outward.
Reach as high as you can while twisting your upper body a little bit further with each breath.
You may notice a small lift in your right heel.
Next, flip the opposite sides.
Gracilis muscle Strengthening Exercises:
Multiple tiny muscles in the inner thigh that are in charge of bringing the thighs together, maintaining balance and support, and ensuring good hip alignment are used in gracilis muscle workouts. We are here to disrupt the mindset that most individuals should only think about practicing hip adductor exercises when they pass the gym’s hip adductor machine.
Strengthening the gracilis muscles is crucial for improving stability, preventing leg pains, and increasing mobility and flexibility. Strong abductors are essential for preventing pain as you age, preserving mobility, and doing well in sports. Because they can be challenging to train effectively, the adductors are often disregarded when it comes to strength training.
Standing Leg Circles
Side-Lying Hip Adduction
Squat Side Kick
Standing side Leg Raise
Sumo Squat
Cross Scissors
Dumbbell Side Lunge
Cossack Squat
Copenhagen Side Plank
Cable Hip Adductor
Seated Hip Adduction
Adductor machine
Wide stance squat
Standing banded adduction
Seated banded adduction
Standing Leg Circles
standing-leg-circles
How to do it?
This rapid warm-up exercise helps to increase blood flow to the upper leg and hip muscles.
Place your feet hip-width apart for the standing leg circular exercise.
Lift your left leg off the ground. Make a tiny circle with your left leg while maintaining your balance on your right leg.
Note: If you struggle with balance, position yourself near a prop that will allow you to support your body with a hand.
Side-Lying Hip Adduction
How to do it?
To lift your leg off the ground, simply concentrate on using your hip adductor muscles.
To perform this exercise, you must lie on your left side with your arms extended in front of you, supporting yourself with your forearm and elbows on the floor. With your heels against the bottom leg’s thigh, lift your right leg over your lower leg.
Keep your leg outstretched and lift it as high as you can.
Return to the starting position gradually.
Perform 10–25 left-side repetitions before switching to the right leg.
Note: If you struggle with balance, position yourself near a prop that will allow you to support your body with a hand.
Side-Lying Hip Adduction
Side-Lying Hip Adduction
How to do it?
To lift your leg off the ground, simply concentrate on using your hip adductor muscles.
To perform this exercise, you must lie on your left side with your arms extended in front of you, supporting yourself with your forearm and elbows on the floor. With your heels against the bottom leg’s thigh, lift your right leg over your lower leg.
Keep your leg outstretched and lift it as high as you can.
Return to the starting position gradually.
Perform 10–25 left-side repetitions before switching to the right leg.
Note: By strapping an ankle weight to the leg or utilizing a resistance band fastened to an anchor, you can add some provocation to your workout.
Squat Side Kick
How to do it?
The squat side kick bodyweight exercise is an excellent lower limb workout that works both the abductors and the adductors.
This exercise has two movements that allow for both stretching and muscular strengthening, which is crucial to lowering the likelihood of experiencing groin pain.
To perform the Squat Side Kick exercise, place your hands together in front of you and stand shoulder-width apart.
Return to the squatting position and do it again with a different leg.
Keep your back straight, chest up, and avoid letting your knees go past your toes when squatting. This will help your core muscles stay active throughout the exercise.
Standing side Leg Raise
How to do it?
Since you will be employing an isometric hold on your other leg to keep it in the air, this is the greatest bodyweight exercise for targeting the hip adductors of one leg while targeting the hip abductors of the other leg.
You must stand with your shoulders hip-width apart for this exercise. currently standing away from the body on the left leg.
Next, Raise your right leg as high as you can and stay there for four to six seconds.
Perform 2-3 sets of 10–18 repetitions.
Note: Attach ankle weights to both legs to increase the difficulty of this workout.
Sumo Squat
Sumo Squat
How to do it?
This squatting version will target the inner thighs as well as the lower limb muscular groups.
The sumo squat is nevertheless a useful exercise that may be included in regular exercises, despite having a lower range of motion than a standard squat. Drop your hips down and back.
Return to the starting position after pushing off through the ground.
Note: Hold a kettlebell in your hand to add some provocation to your workout.
Cross Scissors
How to do it?
The ideal exercise for concurrently working the hip adductor muscles and the core is this one.
Cross-cutting is difficult since you have to maintain a compressed posture during the motion.
All of your stabilizing muscles must be tensed in order to maintain this position, which involves crossing your legs in front of you.
With one leg crossed over the other, raise your leg off the ground in front of you at a 30–40 degree angle.
Throughout the exercise, your core muscle may be used to create a semi-V shape. Extend your legs to the sides and then bring them back together while crossing the other leg.
Continue doing this with a different leg until you have completed 10–20 reps on each side.
Note: Sitting in a “V” stance without using your arms to brace the upper limb will make cross-scissors more challenging.
Dumbbell Side Lunge
Dumbbell Side Lunge
How to do it?
Stretching and strengthening are two benefits of the side-to-side motion. You can use your hip abductors and hip adductors with the dumbbell side lunge exercise.
You must hold the dumbbells at chest level and stand with your shoulders hip-width apart for this workout.
With your foot firmly planted on the ground, take a big step to your side and lower your hip back and down until your thighs are parallel to the floor.
Bring yourself back to the starting posture by pushing through your flexed foot.
After ten to fifteen repetitions, proceed to the next leg.
Note: You can use bodyweight side lunges to make this workout easier. While attempting to avoid bending forward, you may have your chest up and your back in a neutral position.
Cossack Squat
How to do it?
The Cossack Squat exercise propels the body side to side in the frontal plane of motion.
Ankle, knee, and hip flexibility can be increased by working the lower limb at this position.
By learning this exercise, you will strengthen your hip adductors and obtain a decent stretch, which will boost your stability.
You must drop your hips back and downward while standing with your feet wide apart and your toes pointed outward for this exercise.
With your other leg extended out, heels on the floor, toes pointing up, squat down to that one side and redistribute your weight.
Bring your back to the beginning position after pushing through the ground with your flexed leg.
Repeat this exercise on the second leg by moving the weight & lowering it down into a squat position on the other side.
Note: Cossack Squat exercise involves a high degree of mobility thus if you can not get all the way down then go as far as you can while aiming to improve each workout. Throughout the workout, your back may be kept in a neutral position.
Copenhagen Side Plank
How to do it?
The most challenging type of plank exercise is the Copenhagen Side Plank, which develops the hip adductors in addition to the core muscles. Strengthening the muscles on the outside of the hip will be balanced with the Copenhagen Side Plank exercise.
You must lie on the floor perpendicular to the bench for this exercise, then support yourself using your elbows and forearms.
Place your top leg on the bench after flexing your knee.
Keep this position.
After two sets of 20–25 repetitions, switch to the opposite side.
Note: To make this exercise more challenging, try doing it with your legs outstretched and just your ankle resting on the bench.
Keep this position.
After two sets of 20–25 repetitions, switch to the opposite side.
Note: To make this exercise more challenging, try doing it with your legs outstretched and just your ankle resting on the bench.
Cable Hip Adductor
Cable Hip Adductor
How to do it?
At the gym, you might see ladies do this exercise while the guys ignore it.
Everyone may be using this exercise to strengthen their adductors and lower their risk of pain, thus it’s time to dispel the myth that cable hip adductions are not.
Then, try starting with a lighter weight and a higher number of repetitions until you feel comfortable enough to increase the weight.
Locate a strap attachment that you may fasten to the ankle nearest the pulley.
Adjust the pulley at about calf level. Place yourself beside the pulley.
Adjust the pulley at about calf level. Place yourself beside the pulley. In a secure location where your fingers won’t pinch, brace yourself by placing your hand against the machine.
Pull your leg toward the center of your body and away from the pulley.
Allow the leg to slowly return to its initial position. reached the target number of repetitions.
Note: By fastening a resistance band to a stationary anchor point, the same technique can be used for exercise.
Seated Hip Adduction
Seated Hip Adduction
How to do it?
When you are seated, the seated hip adduction will isolate the hip adductor muscles, requiring you to concentrate solely on bringing your thighs together.
At the end of your leg day, after you’ve finished the larger compound lifts like squats, add the Seated Hip Adduction exercise.
Place your back against the backrest while seated in the machine.
Adjust the knee pads’ breadth to a comfortable level that stretches the inner thighs without overstretching the adductor muscles.
To avoid going overboard, set up a lightweight for the first time.
As you exhale, squeeze your thighs together until your knees meet in the middle of your body.
Return to the starting position gradually.
Perform as many repetitions as possible.
Adductor machine
How to do it?
When most people think of isolation, they might picture the traditional adductor machine used at gyms all over the world.
Even though this machine is the most effective at training the adductor, there are other movements that can have positive outcomes.
This workout is excellent for beginners because you can adjust the weight and pad width. Starting out really light is the greatest way to gain a feel for the workout and prevent pain.
You must first sit on the machine with the pads as wide apart between your legs as comfortable, then choose the resistance level that best suits your ability.
Tighten your thighs together gently until the pads make contact while you can feel your muscles flex.
Return your thighs to the starting position by slowly reversing the motion. Do as many sets and repetitions of this exercise as possible.
Try two or three sets of ten reps if you’re just starting.
Wide stance squat
How to do it?
One of the best leg workouts that will work your entire leg is the squat.
There are other squat varieties, but in this article we’ll talk about the wide stance squat, often known as the sumo squat, which works the muscles in the inner thighs.
This exercise can be performed with body weight alone or with a variety of weighted equipment, such as a barbell, kettlebell, dumbbell, or sandbag.
You must stand slightly wider than shoulder-width apart and turn your toes out for the wide stance squat exercise.
Lower your hips gradually until your thighs are parallel to the floor by shifting your weight backward.
Your inner thigh muscles are then tensed as you push through the ground to return to the beginning position.
Perform 2-3 sets of 10–15 repetitions.
Standing banded adduction
Standing banded adduction
How to do it?
A resistance band is required for this exercise, and it should be wrapped around a sturdy anchor. You must face the resistance band and the anchor point while standing on each side of your body.
By opposing the movement, let the resistance band pull the leg to the side.
You must stand erect and move a banded leg toward your body’s midline to begin this workout. You should feel a nice contraction in your inner thighs.
Release your leg slowly and controllably back to the side.
Do three to four sets of 10 to 20 repetitions on each leg after switching legs.
Seated banded adduction
How to do it?
A resistance band is required for the Seated Banded Adduction exercise. It should be wrapped around a sturdy anchor.
You must face the resistance band and the anchor point while seated on the bench on each side of your torso.
The resistance band is placed right below the knee joint; insert the internal foot through it. Permit the leg to be drawn toward the anchor point by the resistance band.
Contracting the adductor muscle will move your leg toward the middle of your body.
Do this again for each leg.
Lateral Lunge
Lateral Lunge
How to do it?
You must place your feet hip-width apart in order to perform the Lateral Lunge exercise. Start by flexing your left knee while stepping out of your left leg and sending your hip back.
Your knee should be in line between your second and third toes during the descent, and it shouldn’t go more than two inches past them.
The toe somewhat extends outward. To get back to the starting position, push off through the left.
To finish the first repetitions, repeat on the right leg.
On each leg, perform three to four sets of eight to ten repetitions.
When did you not complete this task?
if you were told to rest by your healthcare physician.
if you currently have knee and back pain.
if you recently had a fractured lower limb bone.
if this workout causes you any pain.
How to prevent Gracilis muscle pain?
Gracilis strain can be excruciating and prevent you from engaging in your favorite pastimes.
You can help avoid gracilis pulls caused by strains in a few ways:
Prior to engaging in any physical exercise, warm up your groin and leg muscles. Muscle stains can be prevented by engaging in activities that raise your body temperature, such as a light jog.
For optimal support, put on comfortable shoes.
Gradually increase the training’s intensity.
If you have tightness or soreness in the inside of your thigh or groin, stop exercising.
Regularly strengthen your thigh muscles, particularly if you’ve previously experienced a groin strain.
Consult your physician about other measures to reduce the risk of groin strain.
A recurrent issue could arise from subsequent Gracilis strains. Therefore, both primary and secondary prevention are equally crucial. The intrinsic and extrinsic risk factors for the pain type must be understood in order to identify the athlete who is at risk and potentially address the predisposing condition.
An increased likelihood of new groin pain is linked to lower levels of sports-specific training, higher levels of play, decreased hip adduction strength, and prior gracilis pains. Hölmich et al. showed that chronic groin strains could be effectively treated with an 8–12 week active strengthening program that included progressive resistive adduction and abduction exercises, balance training, abdominal strengthening, and skating movements on a slide board. The preventative program also includes core stability exercises, eccentric exercises, and coordination exercises (which target the muscles associated with the pelvis).
FAQs
How can gracilis muscle pain be treated?
Apply ice packs or give yourself a massage. Before beginning the stretching and strengthening exercises that your doctor, physical therapist, or athletic trainer has recommended, you may apply heat. Apply a warm soak or a heat pack.
What’s the name of the gracilis exercise?
Butterfly Isometric Exercise A few inches in front of your body, place the bottoms of your feet together on the floor while lying on your back and flexing your knees. For at least five seconds, have your partner kneel in front of you and press his hands on the insides of your knees.
What is a biopsy of the gracilis muscle?
The gracilis muscle motor nerve biopsy is a straightforward process. Its rate of complications is tolerably low. None of the patients reported of more weakness or sensory loss as a result of the biopsy, despite the fact that most of them already had impairment from their underlying condition.
What is gracilis commonly known as?
Eastern Mexico is home to the species Galphimia gracilis, which belongs to the genus Galphimia in the family Malpighiaceae. Common names for it include “gold shower,” “shower-of-gold,” “slender goldshower,” and even “thryallis.” It is extensively grown in warm climates all over the world.
What are the gracilis muscle’s trigger points?
The Trigger Point of Gracilis The thigh, ankle, and foot contain the gracilis muscle’s trigger sites. Medial thigh pain is the main symptom of transferred pain, while anteromedial knee pain is the secondary sign.
How much time does it take for a gracilis strain to recover?
A person with grade 1 strains will need to rest for one to two weeks before they can resume their activity routine. Within a few days, you should be able to walk and move normally. It could take three to six weeks for grade 2 strains to completely heal. When most or all of the muscle is torn, a grade 3 strain occurs.
Why does my gracilis hurt?
If the bursa beneath the sartorius, gracilis, and semitendinosus tendons becomes inflamed due to direct trauma, overuse, or pain, an individual may develop this condition, which is typically caused by overuse in athletes and is a common cause of persistent knee weakness and pain.
Is the muscle gracilis deep?
Within the medial (adductor) compartment of the thigh, the gracilis is the most superficial muscle. The skin and subcutaneous tissue cover it superficially, while the deep layer of fascia lata covers its medial portion as well.
How can the gracilis muscle be relaxed?
Sit on the floor with your legs straight out in front of you and your back securely pressed against a wall to stretch the Gracilis muscle. Drop your foot toward the floor and spread your legs as wide as you can.
What is a sickness of the gracilis muscle?
Traumatic osteitis pubis and pain to the adductor longus muscle origin are similar to the “gracilis syndrome,” a fatigue fracture of traumatic aetiology involving the bone origin of the gracilis muscle at the pubic symphysis.
What is the sensation of a strained gracilis?
Symptoms of a Potential Gracilis pain An pain to the gracilis muscle can cause knee pain in addition to groin or thigh pain. Still, gracilis dysfunction can also cause knee pain. Depending on the kind of groin pain, muscle weakness and even bruises may be present.
What is the duration of the healing process for gracilis?
Conclusion: A gracilis muscle rupture should be suspected if there is pain in the medial thighs following an eccentric contraction during hip adduction. Full recovery from the damage happens within six weeks, and ultrasound is helpful.
How can gracilis muscle pain be prevented?
Handling and Therapy Rest: To prevent further pain to your muscle, stop the physical activity that generated the strain. Ice. Compression: Compression minimizes swelling and lowers blood flow to your affected muscle.
References
Valand, B. (2022, August 26). Gracilis muscle pain – Cause, Symptoms, Treatment, Exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/gracilis-muscle-pain/
The sternoclavicular (SC) joint is a synovial joint that connects the sternum (breastbone) to the clavicle (collarbone). It is one of the major joints in the shoulder girdle and plays a vital role in shoulder movement and stability.
The manubrium of the sternum and the medial side of the clavicle articulates to produce the Sternoclavicular Joint (SC joint). The least restricted joint in the human body, the SC joint is the only real articulation that joins the upper limb to the axial skeleton. With its fibrocartilage joint disk, the SC joint is frequently categorized as a plane-style synovial joint. The strong ligamentous reinforcements of this joint frequently cause a clavicle fracture before an SC joint dislocation.
Introduction
Due to the saddle shaped synovial sternoclavicular (SC) joint, the axial skeleton must travel through the upper limb. When the clavicle fractures, the upper limb becomes almost non-functional.
The sternoclavicular joint is one of five articulations which impact upper limb use. Three vital anatomical sections that attach to the sternoclavicular joint are the brachiocephalic arterial trunk, internal jugular vein, and common carotid artery.
As well, there are the phrenic, vagus, esophageal, and tracheal nerves. Thus, the clavicle and sternum, which make up the sternoclavicular joint, provide a vital protective role for structures entering the thorax and their fundamental role in maintaining and supporting the upper limb.
Anatomy
Three bones articulate together to form the SC joint:
The word “manubrium” means “handle” in Latin. The sternum and manubrium are joined.
The clavicle
The band that connects the first rib to the coastal cartilage
Structure and Function
The superior surface of the first costal cartilage and the clavicle’s articulated to the sternum’s manubrium form the sternoclavicular joint.The joint is concave vertically. The fibrocartilaginous articular disc, which has functional mobility in both the anteroposterior and vertical axes, physically divides the articulating surfaces of the SC joint.
The posterior sternoclavicular ligament is the main factor for anteroposterior the support of the SC joint. This ligament is located from the posterosuperior manubrium to the posterior portion of the clavicle’s sternal end. The anterior sternoclavicular ligament additionally avoids excessive superior displacement and stabilizes the SC joint. The manubrium’s superior anterior edge attaches to the clavicle’s medial end through this ligament.
The interclavicular ligament, which enables medial traction of both clavicles, and the costoclavicular ligament, which mediates bilateral clavicle and anterior first rib stability, are additional ligaments that support the stability of the SC joint. The most difficult area of the SC joint is the costoclavicular ligament, which connects the first rib to the inferior surface of the sternal end of the clavicle.
Another crucial role of the subclavius muscle is for keeping the stability of the SC joint. The inferior surface of the central part of the clavicle is where this muscle inserts following a brief laterally. The brachial plexus and the arm’s blood supply are shielded in part by the subclavius muscle. When it contracts, the clavicle is compressed by the subclavius muscle.
Not to mention, significant anatomical linkages of the SC joint are noteworthy. Before the SC joint are the brachiocephalic trunk, internal jugular vein, and common carotid. The esophagus, trachea, vagus nerve, and phrenic nerve are even mediastinal structures that are located behind the clavicle and SC joint.
Articulating Surfaces
For the sternoclavicular joint to form, the following three elements must articulate:
Sternal end of the clavicle
Manubrium of the sternum
The joint of the first rib and the costal cartilage
Fibrocartilage, as opposed to hyaline cartilage, which is found in most synovial joints, covers the articular surfaces.
Joint Capsule
The SC Joint capsule is primarily surrounded by the ligaments due to their relative strength.
The sternoclavicular joint capsule approaches the articular surface’s edges.
A synovial membrane that produces synovial fluid to lessen friction between the articulating tissues along its interior.
Joint Disk
An example would be the inter-articular fibrocartilage disc, which separates the joint into two parts. The disc splits from the manubrium in compartment two and from the clavicle in compartment one.
Unexpectedly, the SC Joint is not congruent, and as a result, a joint disk is provided to improve joint curvature and surface contact. Through absorption of potential loads that could be spread through the clavicle, the SC joint for the meniscus in the knee show joint congruence. Attached to the clavicle’s upper and posterior edges as well as the first rib’s cartilage, the disk helps to stop the clavicle from migrating medially. With the clavicle, the disk goes more than with the manubrium.
Ligaments
The sternoclavicular joint is largely stabilized by its ligaments. Four primary ligaments are identified:
The anterior and posterior sternoclavicular ligaments provide stability for the joint capsule’s frontal and back surfaces.
The upper part of the joint capsule is facilitated by the interclavicular ligament, which adheres to the sternal ends of both clavicles.
The costoclavicular ligament separates the costal cartilage and first rib on the clavicle’s inferior surface.
It is the primary stabilizing force that functions in the joint, preventing the pectoral girdle from rising.
Muscles
The scapula and the entire shoulder girdle, including the clavicle, are the primary movers of the sternoclavicular joint (SC joint), even though no muscles directly affect the SC joint. The clavicle-insertion muscles affecting the SC joint’s movement consist of the sternocleidomastoid, deltoid, pectoralis major, and trapezius muscles.
Deltoid
The axim, lateral third clavicle, and scapular spine are the origin.
insertion: Deltoid tuberosity
Innervation: Axillary nerve (C5, C6)
Arm action: The front portion bends and rotates; the center part abducts the arm; the back part extends and rotates the arm.
Pectoralis Major
Although the origin is reached by the sternum and superior six costal cartilages, the sternocostal head appears in the medial half of the clavicle.
Insertion: Intertubercular sulcus of the lateral lip
Medial pectoral and lateral nerves T1, C5, and C6 are situated in the lateral head, whereas medial pectoral and lateral nerves C7 and C8 are the same way located in the lateral head.
The scapula grows anteriorly and inferiorly, where as the humerus rotates and adducts medially.
Trapezius
The origins belong to the nuchal line, spinous processes C7–T12, ligamentum nuchae, and the outside occipital protuberance.
Inserted are the scapular spine, acromion, and third clavicle.
Innervation: Cervical nerves (C3, C4) – pain and proprioception; spinal accessory nerve (cranial nerve eleven, XI) – motor function
Action: intricate; see the previous section on nerves
Sternocleidomastoid
Origin: The sternum’s manubrium and the clavicle’s medial aspect
Insertion: superior nuchal line; mastoid process
Innervation: C2, C3 (pain and proprioception); spinal accessory nerve (cranial nerve XI – motor);
Head movement: tilting the head to the ipsilateral side and turning it to face the other side
Blood Supply
Blood circulation to the sternoclavicular joint is delivered by the internal thoracic and suprascapular arteries.
Innervation
It gets its blood by both the subclavius nerve (C5 and C6) and the medial supraclavicular nerve (C3 and C4).
Mobility and Stability
Strong and flexible sternoclavicular joints enable the upper limb to move easily while sustaining a stable connection between it and the trunk.
Here, we’ll look at the elements that support both its stability and mobility:
Mobility:
This joint type, a saddle joint, allows for two axes of motion.
Articular disc: this facilitates more natural sliding between the clavicle and the manubrium, enabling mobility and rotation in a third plane.
Stability:
Strong, thick joint capsule.
Stress gets passed on from the clavicle to the manubrium by the costoclavicular ligament, particular, via the costal cartilage.
Movements
The sternoclavicular joint can move in a variety of ways and is very mobile. These movements include:
Elevation of the shoulders: shrugging them or extending the arm past 90 degrees
Shoulder depression can manifest as drooping shoulders or extending the arm behind the body at the shoulder.
This anterior displacement of the shoulder girdle is called protraction of the shoulders.
The movement of the shoulder girdle posteriorly is known as shoulder retraction.
The passive rotation of the clavicle and scapula occurs when the arm lifts over the head.
Clinical significance
Dislocation
Although sternoclavicular dislocation is uncommon, it can happen as a result of indirect forces applied to the shoulder or direct trauma to the clavicle. Surgical intervention may be necessary to correct posterior dislocations, as self-healing is not likely to occur. These dislocations pose a life-threatening risk due to the potential damage they may cause to critical tissues in the mediastinum. Occasionally, there may also be a spontaneous partial dislocation.
Arthritis
The SC joint may have osteoarthritis, which can cause discomfort, edema, and restricted movement. This is particularly prevalent in senior citizens.
Costoclavicular Syndrome
This disorder compresses the neurovascular systems beneath the collarbone, which frequently results in upper limb discomfort. Postural problems or repeated activities may be linked to it.
Sternoclavicular Joint Pain
Tendinitis or bursitis are two conditions that can produce pain at the SC joint, which can interfere with daily activities and arm movement.
Post-surgical Complications
Shoulder and thoracic surgery can affect the SC joint, resulting in problems or changed biomechanics.
Infection
Infections in the SC joint are rare, although they can happen, especially in immunocompromised people or after intravenous drug usage.
FAQs
How does one define the sternoclavicular joint?
Sternoclavicular (SC) joints interact the clavicle (collar bone) to the sternum (breastbone). The only joint that supports the shoulder and joins the arm to the body is the SC joint.
What kind of joint is the sternocostal joint?
Osteochondral joints, also called costosternal articulations or sternocostal joints, are synovial plane joints that connect the sternum to the costal cartilages of the happen ribs. The first rib is the sole exception, as its cartilage forms a synchondrosis joint with the sternum right away.
Sternoclavicular joint palpation: how to do it?
Pressing one hand laterally from the manubrium and following the clavicle medially can allow you to feel the SC joint. The patient should be supine for the best evaluation of this joint.
Does the sternoclavicular joint exhibit stability?
The sternoclavicular joint is largely stabilized by its ligaments. Four primary ligaments are identified: The anterior and posterior sternoclavicular ligaments support and strengthen the joint capsule on both sides.
What does the sternoclavicular joint consist of?
Its two sections are separated by a fibrocartilage-based articular disc. The superior surface of the costal cartilage of the first rib, the clavicular notch of the sternum, and the sternal end of the clavicle interact to form the joint.
The sternoclavicular joint is acted upon by which muscles?
The clavicle’s interposing muscles, the sternocleidomastoid, trapezius, deltoid, and pectoralis major, control how the SC joint moves.
What is the sternoclavicular joint’s depression?
Assumed values for the elevation and depression are 45 and 10 degrees, respectively. A strain on the subscapularis muscle and the costoclavicular ligament prohibits the elevation. It has been proven that bone contact with the front rib, the interclavicular ligament, and the superior sternoclavicular ligament improves depression.
How much movement is permitted at the sternoclavicular joint?
The sternoclavicular joint can move in three different ways: axial rotation, elevation-depression, and protraction-retraction.
References
Epperson, T. N., Black, A. C., & Varacallo, M. (2023, November 17). Anatomy, shoulder and upper limb, sternoclavicular joint. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK537258/
Wikipedia contributors. (2024, August 26). Sternoclavicular joint. Wikipedia. https://en.wikipedia.org/wiki/Sternoclavicular_joint
Sternoclavicular joint. (2023, October 30). Kenhub. https://www.kenhub.com/en/library/anatomy/sternoclavicular-joint
Protein powders have gained popularity among individuals seeking quick weight loss solutions. These convenient supplements have the potential to transform your weight loss journey. They can help maintain muscle mass, boost metabolism, and control hunger.
You can improve your weight decrease efforts and more efficiently accomplish your goals by including a premium protein powder that has all nine essential amino acids. In this thorough guide, we’re going to discuss the top protein powders for weight loss and how to use them to get the most out of your diet.
According to studies, protein may improve your metabolism by having thermic effects, which means that consuming protein causes your body to burn more calories than digestion fats or carbohydrates.
This becomes important as well as helpful during weight loss since it promotes fat loss while maintaining lean muscle mass. Selecting a premium protein powder could ensure that you receive the vital amino acids your body needs for both muscle repair and general wellness.
The best protein powder may help you lower weight and lead a better lifestyle by reducing appetite, increasing metabolism, and preserving muscle mass. Take a look at the best choices if you want to reach your weight loss objectives.
How Does Protein Affect Weight Loss?
One vital element that has significant effects on weight loss is protein. It lessens the chance of overeating and consuming too many calories by enhancing feelings of fullness. Moreover, the body burns more calories when digesting protein since it has a larger thermic effect than fats and carbohydrates. Over time, this improvement in combustion may lead to more fat loss.
Lean muscle mass is essential for maintaining a healthy metabolism, and protein aids in maintaining it while losing weight. You may maximize your weight loss efforts and get more favorable results by incorporating enough protein in your diet. All of these benefits can be increased by selecting the appropriate protein powder.
How Can We Select the Best Protein Powder for Losing Weight?
There are several essential factors to take into account when selecting a protein powder to help you reach your weight loss objectives. Examine the source of the protein first. Whey, casein, or alternatives based on plants like soy or pea protein can be included. Aim for 20–40 grams of protein per serving and choose a product with a high protein-to-calorie ratio, minimizing artificial chemicals and added sugars. To verify the product’s purity and safety, look for third-party certification labels.
Look for natural flavoring and extra nutrients like fiber in the ingredient list as well, as these help support digestive health and satiety. You can select a protein powder that helps your weight loss goals by carefully weighing these factors. Knowing how to effortlessly incorporate the product into your diet and lifestyle is crucial after you have made your choice.
How Can Protein Powder Benefit With Weight Loss?
Eat appropriate protein: To promote muscle maintenance and satiety, aim for about 2 grams of protein per kg of body weight per day.
Along with exercise and a healthy diet: Incorporate protein powder into a regulated, low-calorie diet and do frequent physical activity, such as resistance training.
Plan when you will use the protein powder: Take it between meals to control hunger and cravings, or after your workout to help with muscle recovery.
Select outstanding products: To guarantee safety and effectiveness, choose protein supplements that have been tested by a third party.
Top 10 Protein Powders for Weight Loss
Including protein powder in your diet can be a good way to reduce weight. Protein increases muscle maintenance during weight reduction, increases satiety, and speeds up metabolism. The top ten protein powders that can assist you lose weight are presented below:
Transparent Labs completely Grass-Fed Whey Protein Isolate: Every teaspoon of this high-quality protein powder has 140 calories, 1 gram of sugar, and 28 grams of protein. A 30-serving container costs around Rs 13300, making it a great option for anyone looking for expensive, grass-fed whey protein isolate.
Dymatize ISO100: Each serving of Dymatize’s ISO100 has 119 calories, 0 grams of sugar, and 25 grams of protein. Generally costing more than Rs. 10800 for a container of 71 servings, this whey protein isolate is a well-liked option for individuals who want to support their weight loss and fitness objectives.
Isolate from My Proteins Clean Milkshake: MyProtein’s Clear Whey Isolate has 90 calories, 23 grams of protein, and 0 grams of sugar per serving. It is inexpensive for those wishing for a low-calorie, free-from-sugar protein powder, ranging in at about Rs. 4289 for a 40-serving container.
The most common protein powder from Optimum Nutrition:100% Gold Standard Whey, has 119 calories, 1 gram of sugar, and 24 grams of protein per serving. Commonly costing approximately Rs. 3000 for a 29-serve container, it is a reliable choice for anyone wishing to aid in their weight loss.
20 grams of protein, 115 calories, and 0 grams of sugar are all provided in each serving of Ritual’s Essential Protein 18+. This plant-based protein supplement is a great choice for vegetarians and vegans, and it costs about Rs. 4100 for a container that contains 15 dosages.
Nutrition Without Cloth Bare Milkshake: Each serving of Naked Nutrition’s Naked Whey contains 160 calories, 5 grams of sugar, and 25 grams of protein. This minimally processed whey protein powder, which is typically priced at around rupee 6985 for a 12-serving container, is an excellent alternative for anyone looking for a clean, additive-free product.
Transparent Labs Casein: A single serving of Transparent Labs Casein has 120 calories, 3 grams of sugar, and 25 grams of protein. This slow-digesting casein protein powder, which generally retails at about rupees 13300 for a 30-serve container, is perfect for persons who want to aid in weight loss and muscle rehabilitation.
Premier Energy Powder: Every spoonful of Premier Protein’s Powder has 150 calories, 1 gram of sugar, and 30 grams of protein. This whey protein blend, while usually costs about Rs. 3800 for a container of 17 servings, is a feasible and reasonably priced choice for anyone looking to up their protein consumerism.
Productive Vegan Plant Protein: Each serving of Gainful’s Vegan Plant Protein contains 110 calories, 0 grams of sugar, and 21 grams of protein. This adjustable plant-based protein powder, which is typically priced at almost Rs. 1500 for a 10-serving container is a great option for vegans and anyone with certain dietary needs.
The protein Casein+ Casein Protein Powder from Legion Athletics: Every serving of Casein+ has 130 calories, 26 grams of protein, and 0 grams of sugar. Usually charging more than Rs. 5000 for a 30-serve container, the highest-quality casein protein powder is a great option for everyone trying to aid in weight loss and muscle rehabilitation.
Protein Powder’s Potential Hazards and Security Protocols for Weight Loss
Be careful of the following potentially adverse effects when taking protein powder to lose weight:
Troubles with digestion such as gas, bloating, and cramping in the stomach, particularly if you have an intolerance to dairy products or are sensitive to specific protein sources.
Overconsumption may strain renal function and cause an imbalance of other nutrients.
Always select expensive third-party-tested products and adhere to the suggested dosage to reduce dangers. Take a peak at the subsequent table to compare the top protein powders for weight reduction.
Compare and evaluate the top protein powders for losing weight.
You could make an informed choice based on your dietary habits and weight management goals by evaluating the top protein powders for weight reduction. Ultimately, when joined with a healthy diet along with frequent exercise, the correct protein powder can greatly aid in your weight loss efforts. A comparison of several protein powder brands and their recommended applications may be found here.
According to research, eating 500 fewer calories while consuming a significant quantity of whey protein can aid in weight loss. The top protein powders for weight loss that will help you reach your weight reduction goals are listed below:
Bimuscles Nutrition Essential Whey Protein 1Kg
The Essential Whey Protein Powder from Big Muscles Nutrition can help you achieve your weight loss objectives. This premium, global-grade whey protein was created to improve energy levels, aid in rest and recovery, and provide more muscle definition. You can receive the recommended 24 grams of protein per dish.
Consuming this protein powder regularly may help you fulfill your daily protein specifications, preserve optimal muscle health, help you develop and repair muscles, complement your weight goals for weight loss, and keep you feeling full in between meals. According to the company, this product has the necessary amino acids and is minimal in sugar and carbohydrates.
Details of the Essential Whey Protein from Bigmuscles Nutrition: Flavor: Dutch Chocolate
Why choose this product?
After training out, use this protein supplement to help your muscles grow and heal. It might support your weight control goals, enable you to achieve your daily protein requirements, and help you feel satisfied in between meals.
NAKPRO Perform Whey Protein Concentrate
There are 24 grams of protein and 5.3 grams of BCAA in Nakpro Perform Whey Protein Concentrate. It is a nutritious and abundant source of energy that could encourage an appropriate metabolism, improve recovery, lessen muscle loss, and promote the growth of lean muscle. Consuming this protein powder regularly may aid in weight loss and the development and maintenance of lean muscles.
According to the makers, this product is excellent for meal replacement shakes and weight loss plans because it lacks preservatives, additives, soy, gluten, and genetically engineered organisms.
I chose this product because it lacks chemical-based coloring, sugar, genetically modified crops, preservatives, soy, banned ingredients, and additives. Strengthening and promoting muscular growth are two possible applications of this substance.
Protein Powder Mypro Athletic Nutrition Slim Shake:
The ideal meal substitute is Mypro Sport Nutrition Slim Milk Protein Powder. For as long as four hours, it might help decrease appetite. In addition to 31 vitamins, minerals, and herbs, this meal substitute product claims to provide 11 grams of protein. Additionally, it has 3.60 g of fiber, which could aid in digestion.
You could potentially able to increase your metabolism, burn additional calories, and gain muscle using this product.
Mypro Sport Nutrition Compact Shake Protein Powder specifications: Flavor: Belgium chocolate
Item weight: 500 grams
Why select this particular product?
Select this item to promote fullness and satisfaction. Moreover, this product has GMP, WHO, ISO, and FSSAI certifications.
Chocolate, OZiva Protein & Supplements for Women
23 grams of cold-processed whey protein are part of the clean protein combination found in OZiva Protein & Supplements for Women. Better weight management and a lower fat percentage might arise from using this protein powder. This product may aid with digestion, metabolism, and achieving a stable weight because it combines vitamins and minerals including green tea, cinnamon, and flax seeds. Additionally, it contains extracts of tulsi, curcumin, and Shatavari, which may help give women more energy. According to the brand, this product is gluten and soy-free.
OZive Protein & Herbs for Women’s Specifications:
Flavor: Chocolate
Item weight: 500 grams
Why select this particular product?
Select this product to safeguard your hormonal balance, improve digestive health, and lower your body fat percentage. It could potentially enhance the health of both your hair and skin.
Amway Nutrilite All Plant Protein
This protein powder, which is packed with the goodness of a blend of soy, wheat, and yellow peas, may aid in the upkeep and repair of tissues and cells. This plant-based food protein powder has no lactose or cholesterol.
With a high protein level of 80% and 8 grams of protein per 10-gram serving, frequent use of this form of protein powder may aid in weight loss.
Amway the company All Plant Protein Powder specifications:
Flavor: Unflavoured
Item weight: 1 kg
Why select this particular product?
This product can help you accomplish the goals you have for losing weight. It is a protein that is devoid of lactose and cholesterol and might provide you with a synergy of all the important amino acids.
Nitro-Tech Ripped Chocolate Fudge Brownie
Lean muscle development and weight loss may be possible with MuscleTech Performance Series Nitro-Tech Shredded Chocolate Fudge Brownie Protein Powder. Thirty grams of whey protein peptides and whey protein isolate are indicated. Rosehip extract, MCT oil, C, canephora robusta, among others, and L-carnitine L-tartrate comprise some of the special constituents in this product that may aid lessen fatigue and boost weight reduction and muscle growth.
Details of the Nitro-Tech Ripped Chocolate Fudge Brownie Protein Powder courtesy of the MuscleTech Performance Series: Flavor: Chocolate fudge brownie
Item weight: 1.82 kg
Why select this particular product?
Select this product to increase your goat’s milk fat and muscle mass. It has a weight-loss formula, amino acid metabolites, and ultra-clean whey protein sources.
Herbalife Nutrition Personalized Protein Powder
With the power of protein, Herbalife Nutrition Customized Protein Powder claims to help you suppress your desire for food while sustaining your energy levels. With 5 grams of soy and whey protein and 9 essential amino acids, this fat-free protein supplement may help keep and regulate a healthy weight.
Details of the Customized Protein Powder from Herbalife Nutrition:
Flavor: Unflavoured
Item weight: 400 grams
Why select this particular product?
To satisfy your hunger and maintain your energy, choose this product.
Vegan Pea and Brown Rice Protein Powder | MYHERB Plant Protein Powder
Each serving of Myherb Plant Protein Powder may provide 6 grams of branched-chain amino acids, as well as 21 grams of protein, and 21 vitamins and minerals. It’s easy to digest this plant-based food vegan protein. This protein powder is appropriate for after a workout and may aid in muscle building and recuperation. It may assist with controlling your appetite and metabolism. According to the brand, this food remains entirely vegan and free of sugar, gluten, soy, and genetically modified organisms.
My herb Plant Protein Powder’s specifications: Flavor: Chocolate
Item weight: 500 grams
Why select this particular product?
Choose this product because it has FDA, GMP, and certifications from ISO. This vegan, sugar-free, gluten-free, soy-free, and genetically modified product may help promote digestion, boost energy and stamina, and enhance the utilization of fat.
DREXSPORT Wild Whey Protein Powder
Whey protein isolate and concentrate are merged in DREXSPORT Wild Whey Protein Powder for Men and Women. Manufactured from the milk of the A2 category of grass-fed Guernsey cows, this protein powder is low in carbohydrates and fats and contains no added chemicals. It has a highly absorbable 25 grams of protein per 31 grams. Frequent use of this product may aid with weight management, fat loss, immunity optimization, muscle growth and maintenance, and general health promotion.
DREXSPORT Wild Whey Protein Powder’s features for both men and women include: Flavor: Chocolate
Item weight: 1 kilogram
Why select this particular product?
Select this food based on its digestion, taste, quality, mixability, and authenticity.
Sparkfusion True Slim Protein Powder
The Sparkfusion True Slim Protein Powder Meal Replacement Shake has 21 vitamins and minerals, eight Vedic superfoods, and 23 grams of protein with milk. It has the perfect ratio of fiber, advantageous fats, and natural whey protein. This protein powder, which is free of gluten, artificial flavors, and additives for preservation, may aid in weight loss. Consuming this protein powder regularly will help you maintain a healthy lifestyle and aid in weight loss.
The Sparkfusion True Slimp Protein Powder Meal Replacement Shake’s specifications include: Flavor: Chocolate smoothie
Item weight: 500 grams
Why select this particular product?
It might provide all the vitamins and minerals needed and aid in weight loss and the development of muscles.
How can I choose the best protein powder for losing weight?
Protein type: Learn more about each of the kinds of protein powders before choosing the ideal one for women’s weight loss. There are several various types of protein powder, comprising plant-based proteins, casein proteins, and whey proteins.
Components list: Assess the product’s ingredients list. Consider protein powders that are low in ingredients and devoid of artificial sweeteners, excessive sugars, or fillers. To promote satiety and digestive health, look for natural flavorings and additional nutrients like fiber.
Protein content: Get a protein powder with a high ratio of protein to carbohydrates. Choose goods with 20–30 grams of protein if you want to lose weight. This will assist you to control your calorie intake and gain muscle.
Extra features: Search for additional characteristics such as vitamins and minerals, branched-chain amino acids, and added fiber. This mixture is going to market muscular growth and recuperation while preserving feelings of fullness.
Mixability: Pick protein powders that mix easily with either water or milk.
Review: To evaluate the protein powders’ flavor and efficacy, read consumer evaluations and academic viewpoints. For complete quality and purity, look for brands that use third-party testing and transparent labeling.
Is the possible to lose weight with protein powders?
Indeed, through retaining muscle mass and encouraging fullness, protein powders can aid in weight loss. A high-protein diet has been shown to lower appetite, which promotes the control of cravings. Protein powders can help you lose weight, improve your protein utilization, speed up your metabolism, and supply critical amino acids all of which are required for muscle repair. A National Library of Medicine study suggests that protein powders could aid in calorie restriction, which could result in a reduction in body fat.
For several reasons, protein is often thought of as a crucial food for weight loss. Here’s why decreasing weight requires protein:
Satiety: Protein makes you feel fuller for longer because it is a highly satiating food. Eating meals high in protein or even protein powders for weight loss might help block appetite and desires, which may result in consuming fewer calories overall.
The energy expenditure required for breaking down, absorbing, and assimilating nutrients is known as the thermal impact of food (TEF). Because protein has a greater TEF than fats and carbs, when you eat foods high in protein, your body burns more calories. Therefore, if you use protein powder to lose weight, this greater expenditure of energy may raise your metabolic rate and help you lose weight.
Muscle preservation: Maintaining your muscle mass is crucial when aiming to reduce weight. Maintaining and regenerating muscle tissue is a necessity when using protein supplements for weight loss. Lean muscle mass is maintained when you eat enough protein, which is beneficial for general health and a greater metabolic rate. Maintaining your muscle mass while losing weight will also assist avoid a drop in your resting metabolic rate, which can happen when you lose weight.
Benefits for metabolism: It has been proved that protein powder for weight loss enhances several metabolic processes. Certain hormones that assist control of blood sugar levels and encourage fat burning may be synthesized in greater quantities as a result. Protein may additionally mitigate insulin surges that can cause fat storage by stabilizing blood sugar levels.
Exercise and muscle growth: Eating enough protein becomes more important than ever if you’re attempting to reduce weight and regularly participate in physical activity. You might want to try protein powder for weight loss because it can be very challenging to get this protein from your diet alone. Protein offers the fundamental building blocks needed for muscle growth and repair, which enables you to recuperate from exercises efficiently and maybe enhance your body composition.
FAQs
Does protein powder help people lose weight?
By increasing metabolism, suppressing appetite, and preserving muscle mass amid a calorie deficit, it can assist individuals lose weight.
For weight loss, what should you use protein powder with?
To avoid adding unnecessary calories, combine the protein powder with water or a low-calorie liquid.
Which protein powder is excellent for women looking to lose weight?
Transparent Labs Grass-Fed Whey Protein and Garden of Life Sport Organic Plant-Based Protein Powder are two of the top protein supplements for young women hoping to lose weight.
Can protein powder assist with losing weight?
Protein shake companies may claim that their goods aid in weight loss or the reduction of body fat. However, protein shakes aren’t a miracle weight loss therapy. According to some research, there may be advantages to eating more protein than is typically consumed.
Does a high-protein diet assist those who lose weight?
Consuming more protein than the suggested daily intake of food has been shown in several clinical trials to improve body composition by decreasing fat percentage while maintaining fat-free mass (FFM) in both low-calorie and standard-calorie diets, in addition to lowering body weight.
Is protein powder safe to consume?
When taken orally: When taken as directed, whey protein is probably safe for most adults. Increased bowel movements, acne, nausea, thirst, bloating, decreased appetite, fatigue, and headaches are some of the adverse responses that high dosages may produce.
What advantages does protein powder offer for losing weight?
Using protein powder to lose weight may help you feel satisfied for longer. This may lessen calorie intake and regulate hunger. Additionally, it may encourage muscle growth and maintenance, increasing metabolism and fat burning.
What is the suggested protein intake?
Age, sex, intensity of activity, and health objectives all affect the required protein consumption. For adults, 0.8 grams of protein powder per kilogram of body weight is the dietary recommended intake.
Reference
Panjwani, A. (2024, November 14). Best protein powders for weight loss: A comprehensive guide. Truemeds. https://www.truemeds.in/blog/best-protein-powder-for-weight-loss
Shree, T. (2024, October 16). Best protein powders for weight loss: Discover the top 10 options to fuel your weight management goals. Hindustan Times. https://www.hindustantimes.com/lifestyle/health/best-protein-powder-for-weight-loss-10-top-choices-to-control-your-appetite-and-support-your-weight-management-goals-101726217239925.html
A supracondylar humerus fracture is an injury to the humerus, or upper arm bone, at its thinnest point, just above the elbow. Supracondylar humeral fractures are a common elbow injury in children, but they are uncommon in adults.
Most commonly incidence peaks age between 5 to 7. Dropping onto an outstretched hand when the elbow is amplified is the most frequent way to get an injury (particularly landing onto a flexed elbow has a low risk).
Compared to adult patients, children patients get elbow fractures more frequently. When they fall, children often use their outstretched arms as a safety mechanism, which raises the possibility of elbow fractures. Supracondylar humeral fractures account for up to 18% of all pediatric fractures and 60% of elbow fractures.
When treating supracondylar humerus fractures, even accomplished trauma surgeons feel nervous and uneasy, as noted by Dr. Gartland in 1959. Despite improvements in the diagnosis and management of these fractures, orthopedic doctors still confront significant challenges in their practice Guidelines for treatment for the supracondylar humerus It is common practice to portray break designs utilizing the adjusted Gartland classification. These injuries can be highly dangerous because of the possibility of brain injury, vascular injury, and compartment syndrome. Inadequate reduction and fixation may lead to malunion and deformity. Nonetheless, a malunion may eventually allow some individuals to function well.
Due to the close affection of neighboring neurovascular structures, injuries are frequent and require a thorough and thorough examination. Not every case calls for surgery. In certain situations, a firm cast could be enough to promote recovery.
Relevant anatomy:
Anatomy of Supracondylar Humerus
Anatomy of Supracondylar Humerus
Your forearm may rotate because the elbow joint bends like a hinge. In your elbow, there are three primary bones. Both articular and non-articular characteristics can be found on the humerus’ distal end. Your elbow’s muscles, tendons, and ligaments hold each bone in alignment.
There are various types of elbow fractures. There are some big ones. One of these situations is a humeral supracondylar break. Some are smaller than others. An epicondylar fracture, which only affects the point of the elbow, is an example of this. Any sort of break can cause extreme harm to ligaments, muscles, and nerves if cleared out untreated.
supracondylar fracture is a sort of break that most commonly happens in the humerus. The thick bone the fact that joins your elbow and shoulder is this one. The fracture occurs close to the area just above the joint. Supracondylar breaks happen when the humerus breaks fair over the elbow joint at its distal end. The transverse portion of the humerus is fundamentally round, but it becomes flatter as it descends to meet the distal end of the humerus.
Both articular and non-articular characteristics can be seen on the humerus’ distal end. The non-articular structure comprises a front coronoid, spiral fossa, back olecranon fossa, average and sidelong epicondyles, front coronoid, and outspread fossa. On the other hand, the articular structure comprises the average trochlea that is expressed with an ulna and the horizontal capitulum that verbalizes with the spiral head.
The common root of the lower arm flexor musculature is found in a groove on the back of the average epicondyle, where the ulnar nerve travels. The common genesis of the forearm’s extensor muscles is the lateral epicondyle. Because of the association of these muscles, the distal part moves and pivots. Permit the front perspective of the distal humerus to be navigated by the brachial supply route and middle nerve.
Located very superficially to the brachialis muscle along the anteromedial portion of the distal humerus, the brachial artery is often involved in supracondylar humeral fractures. The radial nerve travels between the brachialis and brachioradialis muscles before entering the supinator muscle and traveling into the elbow.
Epidemiology:
The distal humerus’s supracondylar region is the most often fractured elbow in youngsters. Children between the ages of five and seven are typically affected. The median age is roughly six years old, and the incidence gradually declines with age. research shows that the prevalence is higher in men than in women, however, some research suggests a higher frequency in women. Nonetheless, a recent epidemiological analysis found no discernible gender disparities.
Extension-type fractures, which are significantly more prevalent than flexion-type fractures, can occur from falls on outstretched wrists.
Elbow hyperextension in children with ligamentous laxity raises the possibility of extension-type fractures. It has also been demonstrated that these fractures happen more often throughout the summer and on weekends. Children who are elderly are more prone to fractures of the flexion type. These wounds typically affect the upper extremity that is not dominant. Open supracondylar fractures take place in around 1% of cases.
Pathophysiology:
The distal humerus is approximately triangular in the coronal plane, with the medial epicondyle, trochlea, capitellum, and lateral epicondyle forming the base. The slender bone plate located at the intersection of the olecranon and coronoid fossas gives it a dumbbell-like form in the axial plane. The majority of fractures happen when a kid falls on an outstretched arm, causing the elbow to become hyperextended. The distal humerus experiences a significant load as a result of the olecranon process engaging the olecranon fossa. Under stress, the anterior humeral cortex compresses, fracturing the bone at its weakest point.
There may be intact periosteum and posterior cortex. Up to 95% of supracondylar fractures are of the extension-type fracture type, which has this mechanism of damage. Although far less often, flexion-type fractures happen when someone falls on a flexed elbow.
The etiology of the injury and the displacement of the fracture that comes from it also serve as guidelines for the reduction maneuver. The distal component’s posteromedial displacement preserves the medial periosteum. Because of this, the reduction is carried out in a pronated position, preventing varus malalignment by tensing the medial periosteum. Conversely, reduction is done in supination because posterolateral displacement often results in the rupture of the medial periosteum.
Mechanism of injury:
It is more common in children, especially in the age range when skeletal maturation has left the supracondylar bone cortex weak. Age causes the humerus’ distal end to ossify. Being reconstructed between the ages of 6 and 7, the supracondylar region often has a thinner, more slender cortex, making it more susceptible to fracture.
Because it is divided into two columns with a thin bone between them, the distal humerus structure is especially prone to injury and creates a weakness. Most often, falls on an outstretched hand (FOOSH), falls from a height, and falls while playing sports or relaxing cause supracondylar fractures.
The olecranon engages on the olecranon fossa when the hand falls onto the extended hand; if elbow extension is maintained, the olecranon eventually serves as a fulcrum on the fossa—An anterior periosteum dislocates and fractures as the consequence of anterior tensile strain from an anterior elbow joint capsule. Extension type injuries are more common (97% to 99%) than flexion type injuries (1-3%).
As a result, the fracture first occurs anteriorly but later shifts posteriorly. High energy levels disrupt the posterior cortex, which ultimately results in the distal fragment’s total posterior relocation. Fractures of the extension are operated in this manner.
The primary trigger of flexion-type fractures is elbow trauma. In the coronal plane, the distal component likewise has a tendency to translate.
Causes of Supracondylar Humerus Fracture:
Almost any circumstance can result in a broken bone.
One of three things can usually cause an elbow fracture: Your elbow strikes something: You could trip and land squarely on your elbow. On the other hand, you could unintentionally bang your elbow on anything solid. A direct blow could cause a fracture.
Something strikes your elbow: Something in your surroundings could strike your elbow and cause it to break. This might have resulted from a car accident or a football helmet contact while the game was in progress.
Striking your extended arm: When your arm is fully extended, the tendons and muscles are tense and flexed. If you land on your outstretched arm, there’s a chance the broken bones will drift apart.
Risk Factors:
Supracondylar fractures are more prevalent in younger children, though they are occasionally seen in older children. These are also the most common types of fractures in children that require surgery. It used to be thought that boys had a higher risk of supracondylar fractures. However, according to recent research (Reliable Source), females are just as likely as boys to suffer this form of fracture. In a summer season where the injury is most prone to occur.
Symptoms of Supracondylar Humerus Fracture:
Because supracondylar fractures often present with accompanying forearm fractures, soft tissue damage, neurological injury, and a significant risk of developing compartment syndrome, a thorough evaluation of the entire upper extremity should be performed.
Among them are:
History:
In the traditional past history of an outstretched hand fall, pain and swelling on above the elbow, and loss of upper limb function, the onset of discomfort requires particular attention.
It is essential to ascertain if the pain is the result of a fracture or late-onset muscle ischemia.
Observation:
A painful edema in the elbow and forearm that limits movement.
It consists of bruising and skin puckering, which is caused by the proximal fragment “puckering” the deep dermis after crossing the brachialis muscle.
A bleeding puncture wound suggests an open fracture.
The so-called “S-deformity” is frequently observed in fractures of the misplaced extension type.
Vascular status evaluation:
As many as 10% to 20% of displaced fracture occurrences may result in vascular damage. One must palpate the wrist of the damaged extremity to feel for both radial and ulnar pulses. In cases of pulselessness, also known as pulseless hand, other markers of perfusion, such as color (the hand should be pink), temperature, capillary refill (less than 2 seconds), and It is necessary to look at the pulse oximeter’s oxygen saturation.
Neurologic status:
While neuropraxia normally takes two to three months to resolve, neuropraxia is more prevalent and usually does so when normal alignment and lengths are restored. It is crucial to know the extent of the nerve’s involvement and whether the symptoms could worsen or get better before and after treatment.
The Anterior Interosseous Nerve Branch (AIN) of the median nerve is more likely to be involved in the postero-lateral displacement of the distal fracture fragment.
Radial nerve impingement, which typically occurs when the distal fracture fragment is shifted posteromedially, can be evaluated by looking for a reduced feeling in the dorsal portion of the hand and weak wrist extensors.
Flexion-type supracondylar fractures cannot harm the ulnar nerve, yet hand intrinsic muscle weakening can cause loss of feeling in its distribution.
Vascular compromise, ecchymosis, anterior skin puckering, and severe pain are symptoms of compartment syndrome.
Classification:
Class I: Radial, warm, crimson, and well-perfused pulse
Class II: adequately perfused but without a radial pulse
Class III: no radial pulse, pale or cool blue color, and inadequate perfusion
Gartland Classification of Supracondylar Fracture:
Based on Gartland’s system, supracondylar fractures in children have been classified. Fractures can be either extension- or flexion-type injuries, depending on the mode of damage and how the distal fragment is displaced. The most prevalent type of fractures are extension type fractures, whereby the distal fragment is longer than the proximal fragment. Extension injuries were originally divided into three categories: nondisplaced, moderately displaced, and severely displaced.
Wilkins added a division of type II injuries based on whether or not a rotational deformity was present to Gartland’s initial classification. In order to demonstrate multiplanar instability with a damaged periosteum, Leitch included the IV type of fracture. This subtype of fracture is detected intraoperatively when there is complete instability of the fracture.
The modified Gartland classification is as follows:
Type I: There is very little displacement (less than 2 mm) or no fractures at all.
Type IIA: Unbroken posterior hinge and fractures that have moved (>2 mm)
Type IIB: A posterior hinge that remains intact in spite of displacement fracture and malrotation
Type III: Fractures that are fully displaced and cause the posterior periosteum to be disrupted
Type IV: Multidirectional unstable fully displaced fractures are categorized
Gartland Classification of Supracondylar Fracture
Diagnosis:
Physical Examination:
An extension-type break may have happened sometime recently from falling on an expanded arm or flexed elbow. Even though they are uncommon, non-accidental injuries must be checked out because they account for less than half of all fractures. The kid or caregiver may provide a history of discomfort, swelling, or deformity in the affected limb. Youthful children may refuse to utilize the harmed limb. Carefully assessing the damaged limb’s distal neurovascular condition and the soft tissue envelope’s integrity is necessary. It is also necessary to thoroughly evaluate and record any assist wounds.
The arm may be bigger, deformed, and bruised. Any bleeding in the vicinity of the elbow needs to be examined since it can point to an open fracture. A typical twisting for an “off-ended” Gartland III hurt is an S-shaped distortion. A “pucker sign” in the antecubital fossa may indicate that the proximal piece penetrated the brachialis muscle, which indentations the deep dermis.
Given that it denotes a high-energy injury, the attending doctor should be alerted to the likelihood of a brachial artery or median nerve injury. These structures could become caught between the fracture fragments, so the surgeon should proceed with caution when conducting reduction. These people also have an increased chance of getting compartment syndrome.
The radial, ulnar, anterior interosseous, and median nerves’ functions need to be carefully evaluated and recorded. It is best practice to record the motor and sensory capacities of each neuron. There have been reports of brain harm in as numerous as 49% of cases. Vascular impedance has been depicted in 10–20% of uprooted supracondylar humerus fractures.
Similarly, traumatic neurapraxia has been observed in around 11% of fractures, with the most common nerve affected in flexion-type injuries being the ulnar nerve, and the most common nerve involved the anterior interosseous nerve in extension-type fractures.
Brachial course damage may happen in up to 38% of cases of uprooted Gartland III fractures. Verifying the limb’s perfusion in the region distal to the fracture is vital. It is essential to evaluate the ulna and radii beats. Note the warmth and color of the ipsilateral hand in addition to measuring the capillary refill time. It is necessary to distinguish between the “pulseless, pale, cold hand” and the “pulseless, pink, perfused hand.”
Some youngsters have a perfused hand but no pulse, which can be explained by good collateral circulation from the elbow. Both instances require emergency care, but because the latter has evidence of an ischemic limb, surgery is necessary. Vascular compromise and entrapment that involves an artery and a nerve within the fracture site are likely to occur if there is neurological impairment and a hand without a pulse.
Likewise, following every intervention, a comprehensive neurological evaluation is required and ought to be conducted again. Although doing a comprehensive nerve assessment on children can be challenging, certain games, including rock, paper, scissors, and ok, can aid in the evaluation of motor skills. To assess the motor function of the ulnar nerve, the kid is asked to abduct their fingers (scissors), the median nerve is tested by having them make a fist (rock), and the radial nerve is tested by having them stretch their fingers (paper). Lastly, they sign “ok” to indicate that the anterior interosseous nerve has been assessed.
Radiographic Evaluation:
To make the diagnosis, basic elbow radiographs are needed. Verification of the fracture type (flexion versus extension), degree of displacement, malrotation, and comminution requires anteroposterior and lateral views. The elbow is mainly cartilaginous in children. The capitellum is, to begin with, an epiphyseal center to shape at one year of age.
To appropriately interpret elbow radiographs for children, one must have a sufficient understanding of the ossified distal humerus with the age of look and fusion of all epiphyseal centers, such as the proximal radius or ulna.
Anteroposterior (AP) View:
A transverse or short oblique fracture line is sometimes visible in the distal humerus’ supracondylar region. They may even go undetected in nondisplaced fractures because they might be difficult to identify. Baumann’s point is often referred to as the humerocapitellar point when viewing the coronal plane. It is the angle created by a line parallel to the humerus’ longitudinal axis and a tangential line that crosses the capitellar physis. A distance of 64 to 81 degrees from the longitudinal axis line is typical. An elevated Baumann’s angle indicates a cubitus varus malformation. Baumann’s angle is a precise way to measure coronal plane alignment.
Radiocapitellar Line: In each view, a line drawn along the radius’s long axis should intersect the capitellum. Unless a radial head/neck fracture is present, this is typically intact in situations of supracondylar fractures.
Lateral View:
Sign of the Posterior Fat Pad: When the elbow is bent, the posterior fat pad is located next to the olecranon fossa. Each intra-articular bone fracture in the elbow results in bleeding at the location of the fracture. The fat pad separates from the olecranon fossa as a result of the hematoma or effusion that occurs. This comes about in the generation of a positive back fat cushion sign. Numerous scholarly research efforts have highlighted the significance of recognizing the existence of a posterior fat pad sign when diagnosing nondisplaced or hidden intra-articular elbow fractures.
Anterior Humeral Line: A straight line drawn longitudinally on the lateral view along the anterior humeral cortex should divide the middle third of the capitellum. In children younger than four, the line may extend across the anterior third of the capitellum. When the line is positioned anterior to the capitellum, it indicates a fracture pattern consistent with the extension type.
Angiography:
Angiography is not recommended before a decline in the frequency of cases of vascular compromise. The Pediatric Orthopedic Society of North America (POSNA) does not recommend arteriography prior to reduction since it delays treatment.
Differential Diagnosis:
Differential diagnoses include the following:
fractures of the radius head.
fractures that affect the distal humerus’s medial or lateral condyles
Transphyseal fractures of the distal humerus are another differential diagnosis to rule out in situations such as these; these injuries should not be mistaken for unintentional harm.
The history typically points to a pulled elbow, and in these cases, radiographs are rarely obtained.
Treatment of Supracondylar Humerus Fracture:
It is necessary to assess each patient by the Advanced Trauma Life Support (ATLS) recommendations. Every injury sustained by a child needs to be considered non-accidental.
Non-Surgical Treatment:
Nonoperative therapy is appropriate for nondisplaced Gartland I fractures and slightly displaced Gartland IIA fractures. There has been discussion over how to treat Gartland II fractures. For Gartland II wounds, non-operative treatment is attainable given the break arrangement is adequate. In instances of medial column comminution, malunion, and displacement may happen.
The possibility of developing a cubitus varus deformity exists with medial column collapse. It is not suggested to treat Gartland II breaks non-operatively due to three reasons: average comminution, back uprooting, and overabundance swelling.
The non-operative treatment consists of either an above-elbow cast that maintains the elbow at 80 to 90° of flexion for three to four weeks or immobilization in the neck and grasp. Excessive edema may damage the vascularity of the forearm and cause compartment syndrome. Above-elbow casts are a more effective means to alleviate pain than a collar and cuff for Gartland I fractures. One study indicated that patients with displaced fractures of the Gartland II type had favorable outcomes with cast treatment; however, some of them experienced cubitus varus. Patients should refrain from excessive flexion when they have considerable elbow edema, which may result in compartment syndrome.
Traction was once used to treat misplaced fractures. It can be applied in settings with limited resources, such as countries with low or middle incomes and limited access to surgical equipment.
Surgical Treatment:
Orthopedic intervention is recommended for fractures classified as Displaced Gartland II and I II. Patients who have neurovascular impairment, compartment syndrome, or open fractures need to see a surgeon right away. Surgical intervention for closed injuries includes K-wire percutaneous pinning and closed reduction.
Open reduction could be required for vascular exploration, irreducible fractures, and failed closure reduction. Orthopedic surgeons should confirm their capability to address complex fracture patterns that may lead to related neurovascular injuries and that a vascular surgeon is available to aid in the treatment.
Open Reduction and Percutaneous Pinning:
Open diminishment is required when the closed approach comes up short of delivering a decrease. In particular, soft tissue/neurovascular structures that become lodged at the fracture site may hinder anatomical reduction. Open reduction might be required for open fractures.
An open approach to the brachial artery needs to be investigated if perfusion is not established after fracture reduction and repair. Whether open exploration of the brachial artery should be done when the hand is perfused following reduction and fixation but there is no radial pulse is still up for contention. For open reduction, an anterior method is recommended. Other techniques include the posterior, lateral, and medial approaches.
Closed Reduction and Percutaneous Pinning:
This is recommended for Gartland IIB and III fractures. Furthermore, it is advised for Gartland IIA fractures when non-operative treatment (such as medial column comminution) is contraindicated and a cast is unable to produce a good reduction.
The Technique of Closed Reduction:
Closed reduction entails “milking” the soft tissues alongside in-line traction when a pucker sign is observed. While traction serves to extend the fracture to its full length, “milking” assists in freeing the soft tissues. Elbow flexion is necessary to apply traction.
The distal fragment’s medial/lateral translation and varus/valgus angulation are subsequently performed to correct the coronal plane displacement. It can be required to pronate when applying a valgus-directed force or to lie down when applying a varus force. Additionally, these motions help to correct rotational deformities.
Pronation aids in rectifying posteromedial displacement (internal rotation) while tightening the medial periosteum, while supination can assist with posterolateral (external) rotation correction. The sagittal plane distortion in extension-type fractures is addressed by hyperflexing the distal fragment. An extension may be needed in flexion-type fractures.
The Technique of Percutaneous Pinning:
It is possible to operate on bicortical structures like lateral pins and crossing pins (medial and lateral). Iatrogenic ulnar nerve damage is less common when lateral pin designs are used often. You can utilize one, two, or three lateral pins. When inserting pins, the ideal spacing between them—whether parallel or divergent—must be maintained. The divergent pattern is thought to be more stable than the parallel configuration.
Additionally, build rigidity for lateral pins is enhanced via a capitellar starting point rather than a straight lateral entry point. A trans olecranon fossa four-cortex purchase has been described as one technique for lateral pinning to increase construct rigidity. It has been shown that fixation stability is influenced by pin size. It is found that 1.6 mm pins are not as biomechanically strong as 2 mm pins.
The construct’s rotational rigidity is enhanced when crossing pins are utilized in place of two lateral pins, however there is a higher chance of iatrogenic ulnar nerve injury. To protect the ulnar nerve, a large enough incision must be made on the medial side before the insertion of a medial pin. It is advisable to avoid percutaneous medial pin insertion because of the possibility of nerve damage.
Extending the elbow while inserting the medial pin is another technique to lower the risk of iatrogenic ulnar nerve damage This method moves the nerve even more posteriorly.
Physical Therapy of Supracondylar Fracture:
When we examine the humerus bone’s anatomy, we find that the lower end of the bone contains two condyles that contribute to the development of the elbow joint. A fracture that occurs directly above the condyles is referred to as a supracondylar fracture. To make matters more complicated, it is occasionally linked to an intercondylar fracture of the humerus.
When someone falls on an outstretched hand or receives a direct hit to the elbow, they may get a supracondylar fracture. had to defend yourself by extending your hand when you fell. In addition to causing a fracture, direct falls on the elbow also cause the broken section to shift.
Supracondylar fractures can occur as:
Fracture displacement: Surgical reduction is frequently necessary for displaced fractures. Undisplaced fracture: Care must be taken with caution.
In both situations, a posterior mold splint immobilizes the elbow for three to four weeks at a flexion angle of 70°. There are several difficulties associated with immobilizing the elbow joint for an extended length of time, such as restricted joint movement and muscle stiffness surrounding the elbow
Following immobilization with a joint plaster cast, we recommend physiotherapy. Exercise is a good early strategy to help lower these risks. These are the workouts you should perform while your cast is still on.
Phase 1: Distal humerus reduction fracture, weeks 0 to 3:
After surgery, one should begin exercising right away to lessen problems. We must begin shoulder and wrist joint workouts while the splint is in place. Consider that six weeks following surgery, vigorous elbow extension must be avoided. So let’s start with some range-of-motion exercises for the wrist joints.
1) Active wrist flexion-extension for an elbow fracture rehabilitation:
Exercises that promote recovery without impeding the healing process are essential during this stage. Among these exercises is angling the wrist joint while maintaining a comfortable sling over the forearm. This aids in maintaining muscular tone, encouraging normal blood circulation throughout the forearm, and preventing wrist joint stiffness.
Put your forearm on the sling and move your wrist joint up and down as demonstrated in the illustration to complete this exercise.
Try to complete 20 repetitions or more in each session if you are comfortable.
This is a simple exercise to fit into your daily schedule when you have a moment to spare, such as while you’re sitting and watching TV.
2) Wrist circumduction:
Wrist circumduction will be the exercise we talk about next. This is specifically made to avoid wrist tightness. This is a simple exercise that just involves rotating your wrists, as shown in the attached illustration.
With your forearm supported inside the sling, spin your wrist in both clockwise and counterclockwise directions to complete this exercise.
Start by softly turning your wrist in a circle. When you do this, make sure the muscles in your wrists and forearms are stretched.
Alternatively, you can perform this exercise while sitting or standing, whatever is more comfortable for you.
It’s important to do as many repetitions as you can, and as you get more accustomed to the workout, you can quicken the rotations.
3) Grip strength exercise:
Full-Grip-exercise
Grip strength deficiency is not uncommon following an extended period of immobilization. This weakness can show itself in something as basic as gripping a glass of water. For this reason, it’s critical to concentrate on grip strength training as well as any other recommended workouts. The use of a gel or sponge ball is one such activity.
Using the affected hand, forcefully squeeze the ball.
By increasing blood circulation around the hand, this exercise can help any fractures heal more quickly.
To strengthen your grip muscles and aid in healing, try to complete this exercise as often as you can.
4) Shoulder adduction abduction:
Shoulder joint stiffness is another typical problem that can result from prolonged immobilization. Making exercise a priority will help you improve your flexibility and supple. There’s one standing shoulder exercise that works especially well at reducing stiffness.
Starting from a comfortable standing position, use your other hand to support the injured forearm. This will lessen discomfort and assist in stabilizing the joint.
After you’re in position, softly shift your shoulder from right to left without exerting too much force.
Repeat the movement 15–20 times in a session, using the given figure as a guide. This exercise can help you feel less pain and have a wider range of motion with consistent use.
5) Shoulder flexion exercise:
shoulder flexion exercise for a postoperative elbow fracture
The first step in performing shoulder flexion extension is to use your other hand to support your forearm. Flex your shoulder slowly and forth until it is comfortable for you to do so. The shoulder muscles are strengthened and stretched as a result.
Once your shoulder is as comfortable as possible, start slowly bringing it back. To maximize the benefits, repeat this exercise fifteen to twenty times. This exercise can help you become more mobile and strong in your shoulders with consistent practice.
Phase-2: On Weeks 3 to 6 of reduction of distal humerus fracture:
During exercise, you can take the splint off after the third and in between the sixth week. All of the wrist and shoulder joint exercises that we covered must be repeated by you. Exercise repetitions can be increased. You should still resist moving your elbow joint, though.
Carry out these exercises again:
Wrist circumduction,
wrist flexion-extension in action,
Exercises for grip strength,
shoulder flexion exercise,
shoulder adduction and abduction
Phase-3: Week 6 to 10:
The posterior elbow brace will be taken off by the sixth week, at which point we should concentrate on elbow range of motion and strengthening activities. Elbow flexion, extension, forearm pronation, and supination are things we need to pay attention to.
6) Active wrist flexion-extension:
Certain exercises need to be done to restore elbow flexion and extension motion.
Let’s begin by positioning the afflicted arm on a table and taking a comfortable seat in front of it. Elbow exercises can be performed with an adequate basis of support when the arms are kept flat on the table.
First, straighten the elbow to the maximum extent achievable.
After a few seconds of holding the position, gradually bend the elbow to its maximum flexion.
At least 15 to 20 repetitions of this alternate flexion-extension exercise should be performed in a single session.
It is important to consistently carry out this exercise to help the elbow return to its typical range of motion.
7) Stretching of wrist flexor and extensor:
Stretching of wrist flexor and extensor
This particular stretching practice is intended to assist reduce stress and improve wrist flexibility.
Assume your initial posture and extend your arm in front of you to get started.
Gently push the wrist to its maximum flexion and extension with the opposite hand.
Start by slightly extending your wrist, then apply pressure on your palm with your other hand to stretch the flexor muscles.
Maintain this position for a minimum of thirty seconds to give the muscles time to unwind and expand completely. It should not hurt to feel a slight pressing feeling in your wrist.
Then, to stretch the muscles that make up the extensor group, perform the same motion by extending the wrist.
Apply pressure to the posterior aspect of your hand with your opposite hand once more, and hold the position for at least thirty seconds.
8) Forearm supination, pronation exercise:
forearm pronation supination for humerus supracondylar facture.
Exercises that promote forearm pronation and supination are essential for preserving elbow joint mobility during the healing process following a fracture to the shaft of the humerus. Rotating your forearm clockwise and counterclockwise while supporting it on a flat surface, such as a table, is one of the best exercises for this purpose sure your forearm is safe and solid by placing it flat on the table first. Next, perform supination, or slowly rotating your forearm in a clockwise manner. After a few repetitions, go on to forearm pronation, which is the rotation of your forearm in an anticlockwise manner.
You can attempt this exercise on your own after you feel more at ease with it. On the other hand, you can rotate your forearm while holding a cane or light rod to increase the exercise’s effectiveness. This will make the activity more difficult and advantageous for your rehabilitation by adding additional resistance and velocity.
9) Shoulder forward elevation exercise for elbow fractured:
In some circumstances, it’s normal to ignore shoulder joint soreness. If, however, this issue is not resolved, it may soon become problematic. It is essential to include shoulder workouts in your regular routine because of this. The straightforward yet powerful shoulder elevation exercise is one of these.
To begin with this exercise, take hold of your hand and slowly raise it as high as you feel comfortable going.
After holding it there for a short while, carefully bring it back down.
In a single session, repeat this technique fifteen to twenty times.
Try to perform this exercise twice a day for the best results.
Shoulder range of motion (ROM) exercises are beneficial for both preventing and treating shoulder stiffness.
10) Stretching of elbow flexor muscle:
ROM exercise supracondylar fracture
The flexors and extensors of the elbow, two muscle bunches fundamental to elbow development, are the center of this workout. The flexor muscles, which are found on the outside of the elbow, are in charge of allowing the elbow joint to flex. The extensor muscle, on the other hand, is found on the back of the elbow and is in charge of the elbow joint’s extension or straightening.
To start the elbow flexor stretching exercise, extend your elbow to its maximum and place your other hand on the front of your elbow.
Till the front of the elbow stretches comfortably, slightly overpress the area.
To help the muscles relax and release tension, hold this stretched position for at least 30 seconds.
It’s also time to extend your elbow extensors. You must do this by twisting your elbow and resting your other hand on the back of your elbow.
After you feel a comfortable stretch on the back of the elbow, slightly overpress the area and hold it there for at least thirty seconds.
It is advised to perform this procedure three to five times in a single session to avoid overdoing it and causing additional harm.
Phase-4: Weeks 10-12+ of supracondylar elbow fracture:
Return to light activities and exercise gradually. After 12 weeks, there are no further restrictions on activity.
Progressive strengthening exercises:
supracondylar fracture exercise
It’s important to gradually return to modest activity and exercise as part of your recovery. There are no further activity limitations after the first twelve weeks.
To perform this exercise, you will need a set of 1.5–2 kg dumbbells. It’s necessary to remember that this exercise should only be done if you have developed the grip strength to grasp the dumbbell firmly.
Start by standing erect posture and using the hand on the affected side to hold the dumbbell. Hold it firmly enough that your elbow joint feels a mild stretch from the dumbbell’s weight.
As long as it suits you, maintain this posture for one to five minutes.
The weight of the dumbbells can be gradually increased to 5 kg as you get more used to this exercise
Home care advice:
To lessen edema during the initial two days:
When your child is seated or sleeping, use pillows to lift their arm above their heart.
For a few days, apply cold packs covered in a towel to the cast for 20 to 30 minutes every 3.4 hours.
To keep the cast or splint dry, avoid placing ice directly on it.
If your child’s physician recommends giving them pain medication, you can give them either Ibuprofen (any brand) or Paracetamol (any brand).
To determine your child’s appropriate dosage, refer to the instructions on the medication container.
Giving your child aspirin can result in serious consequences, so avoid doing so..
As advised, make sure your youngster shows up for the follow-up visit.
Make sure your youngster stays away from playground equipment, sports, gym classes, and other activities until you give the all-clear.
Daily cast or splint care:
Remind the child to wriggle their fingers to maintain regular blood flow.
Examine the splint’s or cast’s margins.
Make sure the edge padding isn’t being removed or picked at by your child.
Ensure that the child doesn’t fill it with food, toys, or other items.
Keep powder, lotion, sand, and contaminants away from the splint or cast.
When your child is up and moving around, make sure they are wearing the sling. The child should not sleep with the sling on.
Keep the cast dry:
Avoid swimming.
Give your kids sponge showers.
Older children should bath rather than shower.
When the child bathes, cover their arm with a plastic shield. To keep the cast or splint entirely out of the water, raise the arm up on anything.
Use a hair dryer preset to cool and gently blow air into the cast or splint if it has accidentally spilt.
Complication:
Immediate effects associated with neurovascular involvement include the following: Vascular insufficiency is most frequently associated with Type II and III supracondylar fractures, which are frequently observed in fractures that are displaced postero-laterally, and pink pulseless hand involvement of the brachial artery.
0.1% to 0.3% of cases may have compartment disorder. Compartment weights are expanded by elbow flexion past ninety degrees and related lower arm fractures To lower the risk of compartment syndrome, the elbow should be immobilized at a flexion of around 30° in the emergency department and 60° to 70° following surgery.
The neurologic deficit ranges from 10% to 20% of humeral supracondylar fractures and is primarily linked to Type III fractures.
Pediatric patients often have long-term difficulties due to their exceptional ability for bone growth and remodeling. As a result, the immediate post-management condition and the long-term functional outcome of a fracture may be very different.
The cubitus varus deformity, occasionally referred to as a “gunstock” deformity, is brought on by a malunion. The displacement of the medial head of the triceps, delayed postero-lateral rotatory instability (PLRI), and secondary distal humeral fractures are important problems associated with posttraumatic cubitus varus deformity.
Modern surgical methods, such as closed decrease with percutaneous sticking, have diminished the predominance of this method in children treated for supracondylar breaks from 58% to generally 3%. The disease is treated with a humeral osteotomy, which also prevents future difficulties of the same kind.
If associated ischemia is not treated right away, compartment syndrome may lead to Volkmann’s ischemic contracture. Fixed elbow flexion, forearm pronation, wrist flexion, and metacarpal-phalangeal joint extension are the characteristics of this syndrome. Infarction could also result from it.
Prognosis:
The prognosis is influenced by the patient’s remodeling potential, injury-specific factors, and bone quality.
Remodeling Factors:
Remodeled areas are subject to the following requirements:
The age of the patient and their potential for further growth
The distinction between a real break and a genuine
The displacement level of the deformity plane
The humerus’s physis is accountable for 20% of the distal humerus’s longitudinal expansion. Compared to the coronal plane, the elbow’s sagittal plane distortion offers more remodeling potential. Consequently, the supracondylar area of the distal humerus has limited potential to heal after injury in situations of malunion deformity.
Younger patients have more possibility for remodeling because they still have more growth in them, but only for sagittal plane deformity. Coronal plane deformity does not remodel.
Injury-Specific Factors:
Damage level
Enough reduction and fixation
The neurovascular state of the leg
Taking a proper treatment at the right time improves the long-term prognosis for many injuries. However, comes about can be made strides with anatomical lessening, steady obsession, and suitable care of the delicate tissues, counting neurovascular wounds and compartment disorders, higher-grade wounds may have a more awful prognosis.
Non-displaced Gartland I breaks more often than not mend well without any problems. Cubitus varus needs to be recognized, minimized, and stabilized if it appears in Gartland II fractures with medial comminution. Even in spite of the fact that Gartland III and IV wounds have a higher chance of neurovascular harm, opportune and fitting treatment can lead to effective comes about.
Summary:
In the time frame of the ages of five and eight, the most frequent type of fracture in children is a supracondylar fracture of the humerus. The most visited mode of harm for a humeral supracondylar break is FOOSH.
Preoperative and postoperative neurovascular evaluations are crucial. For displaced fractures without neurovascular involvement, closed reduction with percutaneous pinning is the advised medical procedure. It is recommended that children with elbow fractures engage in physical activity as opposed to passive care.
FAQs
What nerve damage is typical in fractures of the supracondylar humerus?
While ulnar nerve palsy is the most frequent postoperative consequence, anterior interosseous nerve injury is the most frequent starting injury.
What is the name for a supracondylar fracture?
Your child’s humerus fractured near the elbow, just above the joint. The term supracondylar (pronounced soo-pruh-kaan-duh-lr) refers to this kind of humeral fracture. The most prevalent kind of elbow fracture, affecting kids less than eight, is this one.
What surgical procedure is used to treat supracondylar fractures?
Treatment for supracondylar humerus fractures in children (SHFC) can result in iatrogenic brain injury, functional deficiency, and residual deformity. The conventional treatments include closed reduction and various configurations of percutaneous Kirschner wire fixation.
What symptoms indicate a supracondylar fracture?
severe arches in both forearms and elbows. Swelling in your elbow. You can’t extend your arm because of tingling in your hands and a loss of elbow function.
How is a pediatric supracondylar humerus fracture treated?
The recommended courses of therapy for the majority of displaced supracondylar fractures include closed reduction and percutaneous pinning (with two or three lateral pins). Medial pin implantation is necessary in some fracture patterns, and surgical procedures are described to minimize damage to the nerves.
What is the healing period for a supracondylar humerus fracture?
Supracondylar humerus fractures often heal in 4 weeks after therapy (casting or surgery). It can take your child four weeks to be able to move their elbow normally when their cast is taken off. Your youngster will receive a sling or a removable long-arm splint if they have pins in their arm.
Is surgery required for all supracondylar fractures?
Patients with non-displaced type 1 traumas (bones that shattered but did not move) are placed in a long arm cast for protection while the arm recovers. In type 2 and 3 injuries, the bone shifts or displaces, therefore surgery is usually necessary to realign the bones.
How should someone with a supracondylar fracture sleep?
When your child is seated or sleeping, use pillows to lift their arm above their heart. For a few days, apply cold packs covered in a towel to the cast for 20 to 30 minutes every 3.4 hours. Ice should not be applied directly to a cast or splint because they need to be dry.
How is a supracondylar fracture detected?
Anteroposterior (AP) and lateral x-rays of the distal portion of the humerus (not the elbow) should be obtained if a supracondylar fracture of the humerus is suspected. ADVICE: Refrain from wearing a short, fragile backslab.
What deformity follows a supracondylar fracture most frequently?
The elbow deformity known as cubitus varus (red arrow) may be caused by a supracondylar humeral fracture that is not healing properly. The forearm deviates towards the midline and the arm’s typical carrying angle is reversible when the elbow is stretched.
In what way does a supracondylar fracture harm?
The symptoms of a supracondylar fracture include severe, excruciating elbow and forearm pain. a pop or snap at the moment of harm. swelling in the elbow’s surrounding area.
What is the name of a supracondylar fracture?
Supracondylar fractures occur into two categories: flexion (<5%) and extension (95–98%). Supracondylar fractures of the extension type usually originate from falls onto an overextended elbow.
What does a supracondylar fracture angle mean?
if evaluating supracondylar fractures, or distal humeral fractures, Baumann’s angle is utilized. By drawing a line across the center of the humeral shaft, the trochlea, and finally a line perpendicular to the humeral shaft line, one can determine the angle.
Where is the supracondylar region?
The upper arm’s long bone is called the humerus. A fracture of this bone’s lower portion, at the elbow, is called a supracondylar fracture. Especially in younger children, it is one of the most frequent fractures we find.
Reference:
Solanki, G. (2024d, January 27). Supracondylar Humerus Fracture – What You Need to Know. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/supracondylar-humerus-fracture/
Hope, N., & Varacallo, M. (2023b, August 4). Supracondylar Humerus Fractures. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK560933
Ekka, S. S. (2024, March 4). 9 Easy Supracondylar Fracture Humerus Physiotherapy Exercises| Elbow Fracture. Physiosunit. https://physiosunit.com/supracondylar-humerus-fracture-treatment-physiotherapy/