Cubital Tunnel Syndrome
Cubital tunnel syndrome is one kind of peripheral nerve compression (CBTS). It is an irritation or injury to the ulnar nerve in the elbow’s cubital tunnel. Cubital tunnel syndrome can be brought on by compressing or irritating the ulnar nerve, which runs down the inside of your elbow. This could cause your hand and fingers to hurt, become numb, or tingle.
The course of treatment for cubital tunnel syndrome will depend on the severity of your symptoms. in modest situations that are treated conservatively. Surgery might be necessary to release the pressure on the ulnar nerve if your symptoms are more severe. The cubital tunnel syndrome symptoms and possible reduction treatments are discussed in this article.
What is Cubital Tunnel Syndrome?
- Cubital tunnel syndrome, sometimes referred to as ulnar nerve entrapment, is a disorder caused by irritation or compression of the ulnar nerve nearby of the inside elbow.
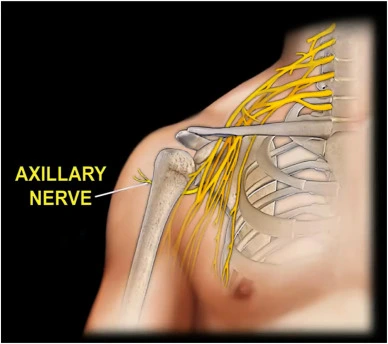
- Nerves are groups of fibers that resemble strings and are utilized by the body and brain to send and receive signals through electrical and chemical changes in the cells. The radial, median, and ulnar nerves are the three main nerves in your arm.
- The ulnar nerve extends down your arm and from your neck to your hand. You may have cubital tunnel syndrome if you have elbow pain or ulnar nerve compression. Additionally, there may be damage to the nerve further up the arm or close to the wrist.
- While the exact cause of cubital tunnel syndrome is not fully understood, it may result from overtly tense or repeated movements that place excessive pressure on the nerve. Other names for this illness that medical professionals may use include handlebar palsy, Guyon’s canal syndrome, bicycler’s neuropathy, ulnar nerve entrapment, and delayed ulnar palsy.
Anatomy of the Cubital Tunnel and Ulnar Nerve
The cubital tunnel, which passes beneath a bone bump on the inside of the elbow, is the tunnel through which the ulnar nerve passes at the elbow. The medial epicondyle is the name of this bony protrusion. The “funny bone” is the term used to describe the location where the nerve passes beneath the medial epicondyle. The nerve at the funny bone is near your skin, so hitting it gives you a shock-like sensation.
On the inside of the elbow, the ulnar nerve runs behind the medial epicondyle.
The ulnar nerve extends above the elbow, passing through the inside forearm muscles and into the hand’s little finger on the side of the palm. The nerve passes via Guyon’s canal, another tunnel, as it enters the hand.
The little finger and a portion of the ring finger receive sensation from the ulnar nerve. Additionally, it regulates some of the larger forearm muscles that aid in creating a firm grip as well as the majority of the small hand muscles that support delicate movements.
The little finger and a portion of the ring finger are sensed by the ulnar nerve. Additionally, it regulates some of the larger forearm muscles that aid in creating a firm grip as well as the majority of the small hand muscles that support delicate movements.
Since this nerve runs the arm’s full length, irritation can happen in several different places. The elbow in the cubital tube is one of the most often occurring locations. The ulnar nerve travels via a tiny gap in the bone, muscle, and ligament called the cubital tunnel inside the elbow.
Around the elbow, the ulnar nerve can be compressed in five main locations: Deep flexor aponeurosis, medial epicondyle, cubital tunnel, and the Arcade of Struthers.
Causes of the Cubital Tunnel Syndrome
It is possible that your healthcare practitioner will not be able to identify the exact root cause of your cubital tunnel syndrome. Among the potential reasons are:
- Anatomy: As you age, you may develop additional muscle or thicker soft tissues covering your ulnar nerve. These two conditions have the potential to impair nerve function and result in cubital tunnel syndrome.
- Pressure: The ulnar nerve can be compressed by the seemingly straightforward action of resting your elbow on an armrest. You may have numbness in your arm, hand, ring finger, and pinky finger when the nerve is crushed.
- Snapping: The ulnar nerve may not remain in its proper position. When you move it, it may break across the medial epicondyle. The nerve is irritated when it is snapped repeatedly.
- Stretching: You run the risk of overstretching the nerve if you bend your elbow repeatedly, as you would when you sleep. Cubital tunnel syndrome could be brought on by excessive stretching.
- Elbow trauma: An elbow fracture, dislocation, or other injury can harm the cubital tunnel or ulnar nerve.
- Arthritis: Rheumatoid arthritis or osteoarthritis can enlarge the elbow joint, compressing the ulnar nerve.
- Bone spurs: The ulnar nerve may be compressed by these bony growths that may form around the elbow joint.
- Ganglions, or sacs packed with fluid, have the potential to form around the elbow joint and compress the ulnar nerve.
Symptoms of the Cubital Tunnel Syndrome
Cubital tunnel syndrome symptoms include:
- Tingling or numb fingers that make it difficult to move (fall asleep).
- Your hand and fingers may get numb occasionally.
- Discomfort in the inner regions of your elbow.
- Tingling that comes and goes in your fingers and hand.
- The most typical symptoms include numbness and tingling in your hands and inner elbow pain. Your elbow is bent when this occurs most frequently. You may have a bent elbow when you: drive, grab a phone, rest.
If any of the symptoms have persisted for longer than six weeks or if they are severe, you should consult a doctor. If you put off getting therapy for the compressed nerve for too long, you risk developing muscle atrophy in your hand. If you receive treatment, though, your symptoms should become better or go away.
Risk Factors of the Cubital Tunnel Syndrome
Many factors increase your chance of cubital tunnel syndrome. Among them are:
- Previous elbow injury: The cubital tunnel or the ulnar nerve may be harmed by an elbow fracture, dislocation, or other injury. Compression of the nerve can also result from healed fracture contracture.
- Arthritis: Rheumatoid arthritis or osteoarthritis can enlarge the elbow joint, compressing the ulnar nerve.
- Obesity: Being overweight can aggravate the ulnar nerve, particularly in people who are anatomically predisposed to cubital tunnel syndrome.
- Diabetes: Nerve injury, especially damage to the ulnar nerve, is more common among diabetics.
- Gender: Compared to women, men are a little more prone to get cubital tunnel syndrome.
- Joint swelling in the elbow
- Tumors close to the elbow joint
- lengthy or repetitive tasks requiring the elbow to be bent or flexed
Diagnosis of the Cubital Tunnel Syndrome
Cubital tunnel syndrome diagnosis is made up of a complete medical history, physical examination, and, if necessary, further diagnostic testing.
Medical history and physical examination:
Your physician will inquire about the nature and timing of your symptoms, as well as any activities that appear to worsen them. Additionally, they will examine your elbow and hand physically, looking for the following:
- Tenderness: You may feel pain or discomfort when you press on the inner side of your elbow.
- Numbness and tingling: Your physician may apply a light tap to your ulnar nerve to check if it causes tingling in your fingers and hand (Tinel’s sign).
- Weakness: Your ability to grasp and the strength of your hand and forearm muscles may be tested.
- Claw hand deformity: In more severe situations, your physician may be looking for evidence of permanent finger clawing or hand muscle wasting.
Imaging tests:
Although not usually required, imaging tests such as MRIs or X-rays can be useful in certain situations to:
- Eliminate alternative reasons for your symptoms: These tests can assist in determining whether any underlying medical conditions such as arthritis, bone spurs, or fractures may be the cause of your suffering.
- Determine the degree of nerve compression: In certain situations, sophisticated MRI methods can show the degree of nerve compression or injury.
Electrodiagnostic investigations:
These examinations involve:
- NCS, or nerve conduction studies: This examination gauges the electrical signals’ intensity and speed as they pass through the ulnar nerve. Weak or sluggish signals may be a symptom of nerve injury.
- Electromyography (EMG): This test can assist in identifying whether the weakness you’re feeling is caused by nerve injury by monitoring the electrical activity of your muscles.
Differential Diagnosis of the Cubital Tunnel Syndrome
Since the symptoms of cubital tunnel syndrome may resemble those of several other disorders, a precise diagnosis is essential to ensure the right course of therapy. The following are some of the most important cubital tunnel syndrome differential diagnoses:
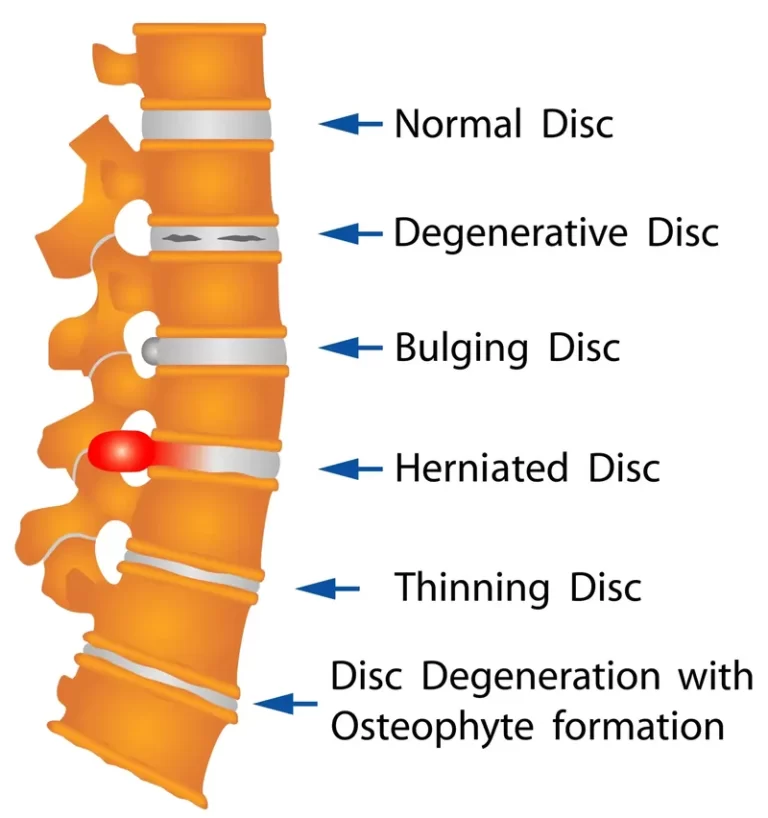
- Cervical radiculopathy: This disorder is caused by compression of the cervical spine’s nerve roots, frequently as a result of bone spurs or disc herniation. Similar symptoms such as numbness, tingling, and weakness can occur in the hand and arm; however, the distribution of these symptoms may vary slightly based on the damaged nerve root. The difference between cervical radiculopathy and cubital tunnel syndrome can be made with the aid of X-rays and MRI scans of the cervical spine.
- Thoracic Outlet Syndrome (TOS): Compression of the nerves, blood vessels, or other tissues in the upper chest results in thoracic outlet syndrome (TOS). It can cause discomfort, tingling, numbness, and weakness in the hand, shoulder, and arm, among other symptoms. As with cervical radiculopathy, classification can be aided by the particular symptoms and where they occur. To confirm TOS, nerve conduction investigations and other imaging procedures could be useful.
- Brachial plexopathy: Damage to the brachial plexus, a network of nerves that runs from the spinal cord and supplies the arm, shoulder, and hand, is known as brachial plexopathy. In the affected arm, it may result in tingling, weakening, numbness, and extensive discomfort. Diagnosing brachial plexopathy requires a thorough medical history, physical examination, imaging testing, and electrodiagnostic studies.
- Peripheral neuropathy: Damage to the nerves that can occur in any area of the body, including the hands and arms, is referred to as peripheral neuropathy. It can result in several symptoms, including discomfort, tingling, weakness, and numbness. The exact nerves implicated will determine whether or not the symptoms match with cubital tunnel syndrome. To differentiate cubital tunnel syndrome from peripheral neuropathy, electrodiagnostic investigations are necessary.
- Carpal tunnel syndrome: Although it affects the median nerve in the wrist, carpal tunnel syndrome can occasionally appear with comparable symptoms, especially in cases of severity, such as numbness and weakness in the hands. The precise location of the weakness and numbness, however, can aid in differentiating between the two ailments. Furthermore, a particular physical examination test called the Phalen’s maneuver is frequently positive for carpal tunnel syndrome but negative for cubital tunnel syndrome.
- Other conditions: Pancoast tumors, which are lung tumors that invade the chest wall and surrounding structures, syringomyelia, a hollow in the spinal cord, and ulnar neuropathy in other places, such as Guyon’s canal, are less prevalent disorders that might mimic cubital tunnel syndrome. To differentiate these disorders from cubital tunnel syndrome, a comprehensive clinical evaluation, and suitable diagnostic tests are required.
Treatment and Management of the Cubital Tunnel Syndrome
Depending on how severe your symptoms are, cubital tunnel syndrome has several therapy choices. Among them are:
Non-surgical interventions:
- Resting and avoiding behaviors that worsen the condition: This can mean avoiding positions that force you to bend your elbow, such as sleeping with your arm flexed or resting on your elbows for extended periods.
- Wearing a brace or splint: Keeping your elbow straight might relieve pressure on the nerve by keeping it in place.
- Anti-inflammatory drugs: Ibuprofen and naproxen, two over-the-counter drugs, can help lower inflammation and pain.
- Exercises for nerve gliding: These can enhance the nerve’s capacity to pass through the cubital tunnel.
- Physical therapy: You can learn exercises and methods from a Physical therapist to enhance hand function and reduce symptoms.
Surgery:
- You could require ulnar nerve release surgery if nonsurgical therapies are ineffective in relieving your symptoms. Surgery for cubital tunnel syndrome involves releasing pressure on the ulnar nerve in the elbow.
- Cubital tunnel surgery is primarily divided into two types:
- Cubital tunnel opening: By severing the ligament that forms the cubital tunnel’s roof, the surgeon increases the nerve’s available area. The most typical kind of cubital tunnel surgery is this one.
- Transposition of the ulnar nerve: The ulnar nerve is moved to the front of the elbow during this treatment, where compression is less prone to occur. Usually, this technique is reserved for cases where a cubital tunnel release has failed or the nerve is severely compressed.
Seeing a physician is crucial to receiving a diagnosis and reviewing available treatments. Prompt identification and intervention might prevent irreversible nerve injury.
Physical Therapy of the Cubital Tunnel Syndrome
Your quality of life can be enhanced and your symptoms can be effectively managed with physical therapy. Cubital tunnel syndrome is frequently and successfully treated with physical therapy. It can assist with:
- Diminish discomfort and swelling.
- Enhanced nerve gliding (mobility).
- Expand your range of motion and flexibility.
- Boost hand function and strength.
- Avoid issues later on.
Usually, a physical therapist will create a plan of care that consists of:
- Education: Gaining knowledge about the causes, signs, and available treatments for cubital tunnel syndrome.
- Modalities: To assist lessen pain and inflammation, try using cold, heat, ultrasound, or electrical stimulation.
- Exercises: Targeted workouts to enhance function, strength, range of motion, flexibility, and nerve gliding.
- Bracing or splinting: Applying a brace or splint to help keep the elbow straight and relieve pressure on the nerve while doing activities or at night.
For cubital tunnel syndrome, a physical therapist could suggest the following particular exercises:
- Exercises for nerve gliding: To facilitate the nerve’s passage through the cubital tunnel, these exercises entail slowly moving the hand and arm in various directions.
- Exercises for flexion and extension of the elbow joint: These exercises enhance elbow flexibility and range of motion.
- Exercises for wrist extension: These stretch the forearm muscles and can potentially compress the ulnar nerve.
- Exercises for hand strengthening: These activities support the development of hand strength and function.
Remember that these are merely examples and that a physical therapist will create a customized program according to your specific needs and state of health.
Preventive Measure for the Cubital Tunnel Syndrome
Although it’s not always possible to prevent cubital tunnel syndrome, there are a few things you may do to greatly lower your risk:
- Maintain good posture: preserve proper posture by keeping your head in line with your spine, your shoulders back and relaxed, and your core active. Hunching over oneself might cause excessive strain on the ulnar nerve at the elbow.
- Avoid bending your elbows for prolonged periods: Compressing the ulnar nerve can occur from activities that demand prolonged elbow flexion, such as prolonged elbow leaning (on desks, countertops, etc.). To prevent extended static postures, take periodic breaks and shift positions.
- Follow proper sleeping techniques: The ulnar nerve might become irritated by sleeping with your elbows flexed or applying pressure to them all night long. To prevent strain on your inner elbow and to maintain a straight elbow, use pillows strategically.
- Warm up before exercising: If you don’t warm up properly before doing intense or repetitive exercises, you run the danger of compressing your nerves. To get your body ready for exercise, do some mild activity and dynamic stretches.
- Continue using proper lifting technique: Don’t use your back or arms to raise anything; instead, utilize your legs and core for strength. When lifting, try not to twist or bend awkwardly since this might strain the elbows and possibly compress the ulnar nerve.
- Enhance your forearm and core strength: Stronger forearm and core muscles can lessen elbow joint stress and enhance overall body mechanics, which helps to indirectly protect the ulnar nerve.
- Be mindful of repeated work: Discuss ergonomic changes with your employer, such as cushioned armrests, other work positions, or taking regular breaks, if your job requires repetitive motions that cause you to bend your elbow for prolonged periods.
- Pay attention to your body. Keep an eye out for any early indications of pain, such as weakness, tingling, or numbness in your hand or arm. Early treatment of these symptoms can stop the cubital tunnel syndrome from getting worse.
Keep in mind that these are merely general precautions. For an accurate diagnosis and suitable therapy, you must speak with a healthcare provider if your symptoms are chronic or if you suspect cubital tunnel syndrome.
Summary
Cubital Tunnel Syndrome, or compressive neuropathy of the ulnar nerve, is caused by anatomic compression in the medial elbow. The presence of sensory anomalies in the ring and little fingers, intrinsic muscle weakness, and a positive tinea sign over the cubital tunnel is indicative of a clinical diagnosis. Bracing or surgical decompression are examples of therapeutic choices that may be available, depending on the degree, length, and efficacy of nonoperative treatment.
FAQs
What signs and symptoms indicate cubital tunnel syndrome?
Tingling and numbness in the little finger and hand, particularly when the elbow is bent.
Tingling and numbness at night.
Hand aches.
Clumsiness and poor grip because of weakened muscles in the hand and arm involved.
An acute ache in the inside elbow.
Will cubital tunnel syndrome heal itself over time?
If you avoid activities that exacerbate the symptoms and the nerve compression is modest, cubital tunnel syndrome may resolve on its own. For instance, you might need to take extra breaks and use a cushion or pad to lessen the strain on your elbow if your profession needs you to lean on it for extended periods.
Which exercises are beneficial for cubital tunnel syndrome?
Exercises that glide the nerves in the arm and hand may help lessen cubital tunnel syndrome pain. Exercises could involve head tilting, wrist and elbow flexion, and more.
What is the most effective method for ulnar nerve healing?
Strengthening the tendons and ligaments in the hands and elbows with physical therapy.
Medications such as aspirin, ibuprofen, and other over-the-counter analgesics assist in lowering inflammation and pain.
Splints to assist with elbow immobilization.
Which medication works the best for cubital tunnel syndrome?
NSAIDs, or nonsteroidal anti-inflammatory drugs: Ibuprofen and other medications may be helpful. They can lower cubital tunnel syndrome discomfort and the swelling surrounding your nerve.
Does cubital tunnel syndrome get better with massage?
In addition to improving blood circulation in the area, ice and heat therapy can help decrease inflammation, promote mobility, and lessen pain. Arm mobility can be improved and pressure can be decreased with massage therapy, which involves applying gentle and, even pressure to the muscles and nerves.
Is cubital tunnel syndrome irreversible?
If left untreated, cubital tunnel syndrome can cause irreversible harm, however the illness itself is not. Cubital tunnel syndrome may be treated surgically or non-invasively by an elbow specialist. Although the illness may occasionally heal on its own, it is best to plan for all possible scenarios.
References
- Cubital Tunnel Syndrome: Signs & treatment | The Hand Society. (n.d.). https://www.assh.org/handcare/condition/cubital-tunnel-syndrome#google_vignette
- Articles. (n.d.). https://www.cedars-sinai.org/health-library/diseases-and-conditions/c/cubital-tunnel-syndrome.html
- Cubital Tunnel Syndrome. (2021, August 8). Johns Hopkins Medicine. https://www.hopkinsmedicine.org/health/conditions-and-diseases/cubital-tunnel-syndrome#:~:text=What%20is%20cubital%20tunnel%20syndrome,inflamed%2C%20swollen%2C%20and%20irritated.
- Ulnar nerve entrapment at the elbow (Cubital tunnel Syndrome) – OrthoInfo – AAOS. (n.d.). https://orthoinfo.aaos.org/en/diseases–conditions/ulnar-nerve-entrapment-at-the-elbow-cubital-tunnel-syndrome/
- Professional, C. C. M. (n.d.-a). Cubital Tunnel Syndrome. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/21997-cubital-tunnel-syndrome
- Chauhan, M., Anand, P., & Das, J. M. (2023, August 14). Cubital Tunnel Syndrome. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK538259/
- Huizen, J. (2024, January 16). How does cubital tunnel syndrome occur? https://www.medicalnewstoday.com/articles/322593


3 Comments