Silfverskiold Test
Introduction
The Silfverskiold test is a clinical examination used to differentiate between gastrocnemius and soleus muscle tightness in cases of ankle dorsiflexion limitation. The test involves assessing passive ankle dorsiflexion with the knee extended and then with the knee flexed.
A greater range of dorsiflexion with the knee flexed suggests gastrocnemius tightness, while no significant difference indicates soleus tightness or other joint restrictions.
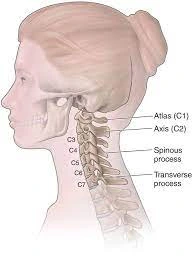
Anatomy of the Foot

The foot is among the most complex areas of the body. The structure comprises 26 bones linked by numerous joints, muscles, tendons, and ligaments. The foot can be affected by various stresses. Foot problems can lead to pain, swelling, or damage. These problems can lead to restricted movement and mobility.
Gastrocnemius muscle
Origin
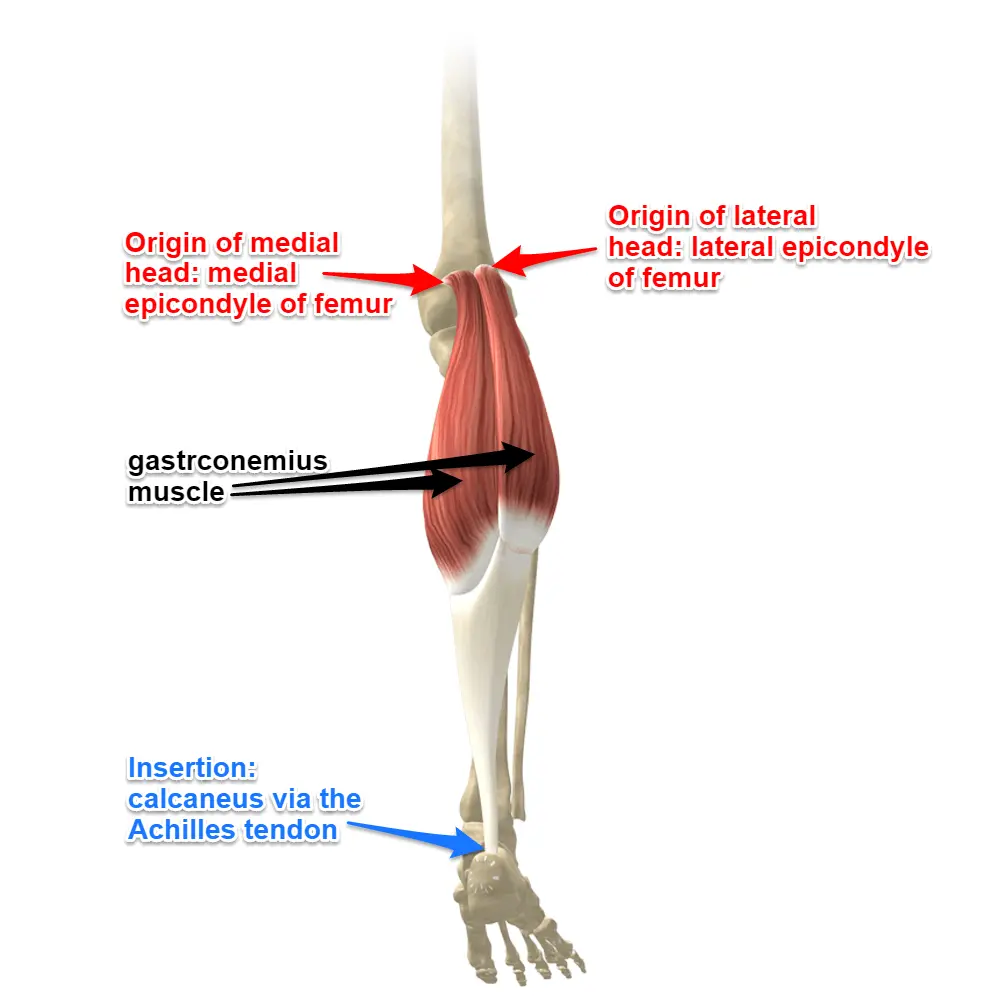
The two heads are situated from the femur’s medial and lateral condyles.
- The medial head is located behind the medial supracondylar ridge and the adductor tubercle on the femur’s popliteal surface.
- The lateral head is on the outer side of the femur’s lateral condyle, positioned just above and behind the lateral epicondyle. An accessory tiny bone known as the fabella is typically located in the lateral head of the gastrocnemius. Both heads are connected to the knee joint capsule and the oblique popliteal ligament.
Insertion
- The gastrocnemius muscle’s bulk from each head converges and attaches to the posterior side of a wide membranous tendon.
- It subsequently merges with the soleus tendon to create the upper section of the tendo calcaneus.
- This broad tendon tapers until it reaches the calcaneus, where it expands once more for its insertion on the middle part of the posterior surface of the calcaneus.
Nerve supply
- The tibial nerve (S1 and 2) supplies both heads of the gastrocnemius.
- The main cutaneous supply comes from L4, L5, and S2.
Function of gastrocnemius muscle
The gastrocnemius, along with the soleus, serves as the primary plantar flexor of the ankle joint and a secondary flexor of the knee. It cannot exert maximum force at both joints at the same time; for instance, when the knee is bent, the gastrocnemius cannot produce as much force at the ankle. When the ankle is flexed, the opposite holds.
The gastrocnemius generates a considerable amount of propulsive force during running, walking, or jumping. Taking into account the force needed to launch the body upward, the triceps surae is capable of producing considerable force.
The gastrocnemius muscle tension has numerous fascial connections, and this tension extends to the foot, as well as the knee, hip, and lumbar region. A shortened gastrocnemius muscle may lead to dysfunctions in the physiological movements of the hip, resulting in a decrease in its anteversion (inward rotation of the femur). A key function of the fascial system is to transmit the force generated by the muscle’s contractile component during contraction.
What Is a Contracture?
A contracture happens when your muscles, tendons, joints, or other tissues tighten or shorten, resulting in a deformity. Symptoms of contracture consist of pain and restricted movement in the joint. In such a case, it is advisable to obtain treatment immediately. Contractures can be treated by doctors using medication, casts, and physical therapy.
Since tissue that stretches becomes less flexible, you might:
- Start showing signs of contracture.
- Have difficulty moving the affected area.
- Showing a restricted range of motion.
Risk factors for contracture
- Scarring from burns or injuries.
- Cerebral palsy.
- Muscular dystrophy.
- Nerve damage.
- Stroke.
- Central nervous system diseases.
- Rheumatoid arthritis.
- Tenosynovitis (inflammation of a tendon and its sheath).
- Traumatic injury.
- Being inactive for a long time.
Achilles tendon contracture

A common clinical condition is Achilles tendon contracture, which impacts ankle dorsiflexion. The risk of developing this condition can be various factors, such as neurological conditions, trauma, and developmental abnormalities. A successful treatment for Achilles tendon contracture is Achilles tendon lengthening. This surgical procedure aims to enhance dorsiflexion of the ankle and fix deformity.
Symptoms of Achilles tendon contracture include pain and stiffness in the back of the heel or calf, challenges with foot flexion, and a sensation of tightness or shortening in the Achilles tendon.
- Pain and Rigidity: Pain at the rear of the heel or in the calf region, particularly when extending the foot or rising onto the toes.
- Stiffness in the ankle, which complicates smooth foot movement.
- Pain and rigidity may be more noticeable in the morning or following times of inactivity.
- Challenge in Foot Flexing: Diminished capability to flex the foot downwards or “push off” from the injured leg while walking.
- Inability to rise onto the toes of the injured leg.
Purpose
The Silfverskiold test serves to detect isolated gastrocnemius contracture linked with various foot and ankle disorders. Nils Silfverskiold was the first to describe the test. By assessing ankle dorsiflexion with the knee extended and then flexed, the Silfverskiold test differentiates between gastrocnemius tightness and Achilles tendon contracture.
Technique
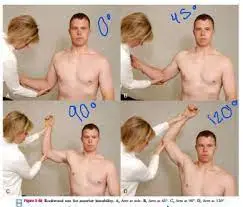
It assesses the dorsiflexion (DF) of the ankle joint when the knee is extended and when it is flexed at a 90-degree angle. A test result is considered positive when the DF at the ankle joint is higher with the knee flexed than when it is extended.
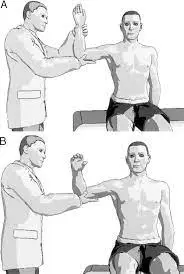
In the Silfverskiold test, the patient must assume a prone position (face down) with both legs off the edge of a table or examination bed. The examiner subsequently dorsiflexes the ankle passively, while keeping the knee joint stable in both full extension and 20 degrees of knee flexion. The available range of ankle dorsiflexion is subsequently assessed and contrasted between the two positions.
A notable difference in ankle dorsiflexion between the two positions, with increased dorsiflexion in the flexed knee position, indicates the presence of gastrocnemius muscle contracture. This is due to the fact that the gastrocnemius muscle crosses both the ankle and knee joints, and when the knee is extended, the muscle is shortened, which restricts ankle dorsiflexion.
The Silfverskiold test can aid in the diagnosis and monitoring of gastrocnemius muscle contracture, which may lead to various foot and ankle problems such as plantar fasciitis, Achilles tendonitis, and flatfoot deformity. Options for treatment can include stretching exercises, physical therapy, and orthotics to enhance ankle range of motion and prevent additional complications.
Clinical Importance:
Tightness in the gastrocnemius muscle can lead to conditions such as:
- Plantar fasciitis
- Achilles tendonitis
- Flatfoot deformity
The Silfverskiold test proves useful for identifying and handling these conditions.
Essentially, it serves to determine which calf muscle is primarily responsible for restricted ankle movement.
Prevention
Though preventing Achilles tendinitis may not be possible, you can implement strategies to lower your risk:
- Increase your activity level gradually. If you are new to exercising, begin at a slow pace and progressively extend the training duration and increase its intensity.
- Take it easy. Avoid actions that put undue strain on your tendons, like running up hills. Before engaging in vigorous activity, start with a warm-up that consists of slower-paced exercises. Should you feel pain while doing a certain exercise, cease the activity and take a break.
- Choose your shoes carefully. While exercising, your footwear should have sufficient heel cushioning and a solid arch support to alleviate tension on the Achilles tendon. Substitute your shabby shoes. If your shoes are still in good condition but lack proper foot support, consider using arch supports in both shoes.
- Do stretching exercises every day. To preserve flexibility, dedicate some time to stretching your Achilles tendon and calf muscles in the morning, before working out, and following your workout. This is crucial for preventing a recurrence of Achilles tendinitis.
- Strengthen your calf muscles. Strong calf muscles help the calf and Achilles tendons manage the stresses they face during physical activity and exercise more effectively.
- Cross-train. Mix high-impact activities like running and jumping with low-impact ones like cycling and swimming.
Conclusion
Gastrocnemius tightness is mainly diagnosed clinically through the Silfverskiold test. This test reveals an equinus deformity at the ankle when the knee is extended, but the deformity disappears upon knee flexion. The Silfverskiold test must be carried out consistently regarding the strength applied during the maneuver, the correction of a flexible hindfoot valgus deformity while conducting the test, and its reproducibility.
This diagnosis is derived from the clinical examination; however, this article introduces further clinical signs that can assist in making the diagnosis when retraction is not clinically apparent. This includes knee recurvatum, hip flexion, lumbar hyperlordosis, and forefoot overload.
In summary, the Silfverskiold test is a straightforward and non-invasive clinical method that can produce useful insights into the degree of gastrocnemius muscle contracture in the lower leg and assist in determining treatment options for various foot and ankle problems.
FAQs
What is indicated by a positive Silfverskiold test?
Before the diagnostic nerve block, all patients underwent assessment via the Silfverskiöld Test. This test was considered positive if passive dorsiflexion of the ankle joint with the knee flexed exceeded that with the knee extended.
How to perform a Silfverskiold test?
In the Silfverskiold test, the patient must assume a prone position (face down) with both legs off the edge of a table or examination bed. The examiner subsequently dorsiflexes the ankle passively, while keeping the knee joint stable in both full extension and 20 degrees of knee flexion.
What is the specific test for the soleus?
The Silfverskiold Test is a physical examination used to evaluate the tightness of the gastrocnemius and soleus muscles. This test is frequently used to assess injuries of the ankle joint and lower leg.
What does the Silfverskiold technique involve?
By assessing ankle dorsiflexion with the knee extended and then flexed, the Silfverskiöld test differentiates between gastrocnemius tightness and an Achilles tendon contracture.
What is the method for testing for shortening of the Achilles tendon?
The test consists of these steps: Your position will be prone, lying on your stomach with your feet and ankles extending over the edge of the examination table. Your provider will apply a gentle squeeze to your calf muscle. While applying pressure, they will check for any movement of your foot or heel.
What difficulties occur from contractures?
Conditions that may be associated include spasticity, heterotopic ossification, degenerative joint disease, fracture, dislocation, and cartilaginous tears, among others. Some contractures can lead to abnormal positioning (such as in a wheelchair or bed), which increases the risk of pressure ulcers.
Reference
- Steve. (2023, March 15). Silfverskiold test – Dr Steve Edwards. Dr Steve Edwards. https://stevenedwards.com.au/silfverskiold-test/
- OrthoFixar. (2024, April 16). Silfverskiold Test Interpretation | OrthoFixar 2025. OrthoFixar Orthopedic Surgery. https://orthofixar.com/special-test/silfverskiold-test/