Sternoclavicular Joint
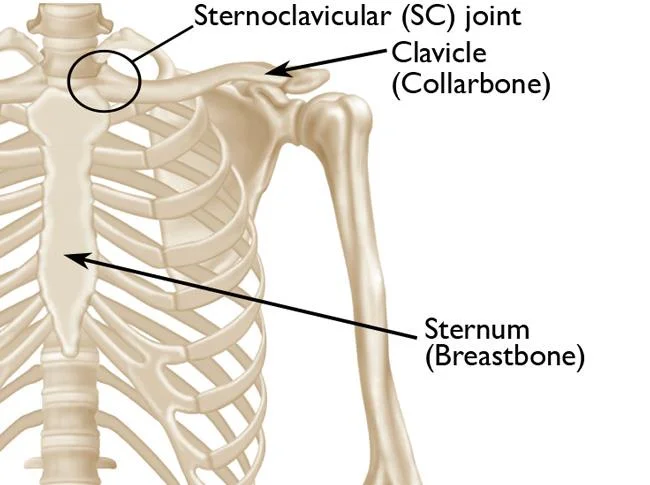
The sternoclavicular (SC) joint is a synovial joint that connects the sternum (breastbone) to the clavicle (collarbone). It is one of the major joints in the shoulder girdle and plays a vital role in shoulder movement and stability.
The manubrium of the sternum and the medial side of the clavicle articulates to produce the Sternoclavicular Joint (SC joint). The least restricted joint in the human body, the SC joint is the only real articulation that joins the upper limb to the axial skeleton. With its fibrocartilage joint disk, the SC joint is frequently categorized as a plane-style synovial joint. The strong ligamentous reinforcements of this joint frequently cause a clavicle fracture before an SC joint dislocation.
Introduction
Due to the saddle shaped synovial sternoclavicular (SC) joint, the axial skeleton must travel through the upper limb. When the clavicle fractures, the upper limb becomes almost non-functional.
The sternoclavicular joint is one of five articulations which impact upper limb use. Three vital anatomical sections that attach to the sternoclavicular joint are the brachiocephalic arterial trunk, internal jugular vein, and common carotid artery.
As well, there are the phrenic, vagus, esophageal, and tracheal nerves. Thus, the clavicle and sternum, which make up the sternoclavicular joint, provide a vital protective role for structures entering the thorax and their fundamental role in maintaining and supporting the upper limb.
Anatomy
Three bones articulate together to form the SC joint:
- The word “manubrium” means “handle” in Latin. The sternum and manubrium are joined.
- The clavicle
- The band that connects the first rib to the coastal cartilage
Structure and Function
The superior surface of the first costal cartilage and the clavicle’s articulated to the sternum’s manubrium form the sternoclavicular joint.The joint is concave vertically. The fibrocartilaginous articular disc, which has functional mobility in both the anteroposterior and vertical axes, physically divides the articulating surfaces of the SC joint.
The posterior sternoclavicular ligament is the main factor for anteroposterior the support of the SC joint. This ligament is located from the posterosuperior manubrium to the posterior portion of the clavicle’s sternal end. The anterior sternoclavicular ligament additionally avoids excessive superior displacement and stabilizes the SC joint. The manubrium’s superior anterior edge attaches to the clavicle’s medial end through this ligament.
The interclavicular ligament, which enables medial traction of both clavicles, and the costoclavicular ligament, which mediates bilateral clavicle and anterior first rib stability, are additional ligaments that support the stability of the SC joint. The most difficult area of the SC joint is the costoclavicular ligament, which connects the first rib to the inferior surface of the sternal end of the clavicle.
Another crucial role of the subclavius muscle is for keeping the stability of the SC joint. The inferior surface of the central part of the clavicle is where this muscle inserts following a brief laterally. The brachial plexus and the arm’s blood supply are shielded in part by the subclavius muscle. When it contracts, the clavicle is compressed by the subclavius muscle.
Not to mention, significant anatomical linkages of the SC joint are noteworthy. Before the SC joint are the brachiocephalic trunk, internal jugular vein, and common carotid. The esophagus, trachea, vagus nerve, and phrenic nerve are even mediastinal structures that are located behind the clavicle and SC joint.
Articulating Surfaces
For the sternoclavicular joint to form, the following three elements must articulate:
- Sternal end of the clavicle
- Manubrium of the sternum
- The joint of the first rib and the costal cartilage
Fibrocartilage, as opposed to hyaline cartilage, which is found in most synovial joints, covers the articular surfaces.
Joint Capsule
The SC Joint capsule is primarily surrounded by the ligaments due to their relative strength.
The sternoclavicular joint capsule approaches the articular surface’s edges.
A synovial membrane that produces synovial fluid to lessen friction between the articulating tissues along its interior.
Joint Disk
An example would be the inter-articular fibrocartilage disc, which separates the joint into two parts. The disc splits from the manubrium in compartment two and from the clavicle in compartment one.
Unexpectedly, the SC Joint is not congruent, and as a result, a joint disk is provided to improve joint curvature and surface contact. Through absorption of potential loads that could be spread through the clavicle, the SC joint for the meniscus in the knee show joint congruence. Attached to the clavicle’s upper and posterior edges as well as the first rib’s cartilage, the disk helps to stop the clavicle from migrating medially. With the clavicle, the disk goes more than with the manubrium.
Ligaments
The sternoclavicular joint is largely stabilized by its ligaments. Four primary ligaments are identified:
- The anterior and posterior sternoclavicular ligaments provide stability for the joint capsule’s frontal and back surfaces.
- The upper part of the joint capsule is facilitated by the interclavicular ligament, which adheres to the sternal ends of both clavicles.
- The costoclavicular ligament separates the costal cartilage and first rib on the clavicle’s inferior surface.
- It is the primary stabilizing force that functions in the joint, preventing the pectoral girdle from rising.
Muscles
The scapula and the entire shoulder girdle, including the clavicle, are the primary movers of the sternoclavicular joint (SC joint), even though no muscles directly affect the SC joint. The clavicle-insertion muscles affecting the SC joint’s movement consist of the sternocleidomastoid, deltoid, pectoralis major, and trapezius muscles.
Deltoid
- The axim, lateral third clavicle, and scapular spine are the origin.
- insertion: Deltoid tuberosity
- Innervation: Axillary nerve (C5, C6)
- Arm action: The front portion bends and rotates; the center part abducts the arm; the back part extends and rotates the arm.
Pectoralis Major
- Although the origin is reached by the sternum and superior six costal cartilages, the sternocostal head appears in the medial half of the clavicle.
- Insertion: Intertubercular sulcus of the lateral lip
- Medial pectoral and lateral nerves T1, C5, and C6 are situated in the lateral head, whereas medial pectoral and lateral nerves C7 and C8 are the same way located in the lateral head.
- The scapula grows anteriorly and inferiorly, where as the humerus rotates and adducts medially.
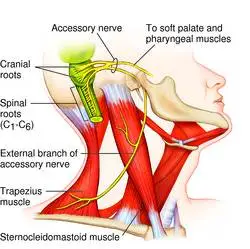
Trapezius
- The origins belong to the nuchal line, spinous processes C7–T12, ligamentum nuchae, and the outside occipital protuberance.
- Inserted are the scapular spine, acromion, and third clavicle.
- Innervation: Cervical nerves (C3, C4) – pain and proprioception; spinal accessory nerve (cranial nerve eleven, XI) – motor function
- Action: intricate; see the previous section on nerves
Sternocleidomastoid
- Origin: The sternum’s manubrium and the clavicle’s medial aspect
- Insertion: superior nuchal line; mastoid process
- Innervation: C2, C3 (pain and proprioception); spinal accessory nerve (cranial nerve XI – motor);
- Head movement: tilting the head to the ipsilateral side and turning it to face the other side
Blood Supply
Blood circulation to the sternoclavicular joint is delivered by the internal thoracic and suprascapular arteries.
Innervation
It gets its blood by both the subclavius nerve (C5 and C6) and the medial supraclavicular nerve (C3 and C4).
Mobility and Stability
Strong and flexible sternoclavicular joints enable the upper limb to move easily while sustaining a stable connection between it and the trunk.
Here, we’ll look at the elements that support both its stability and mobility:
Mobility:
- This joint type, a saddle joint, allows for two axes of motion.
- Articular disc: this facilitates more natural sliding between the clavicle and the manubrium, enabling mobility and rotation in a third plane.
Stability:
- Strong, thick joint capsule.
- Stress gets passed on from the clavicle to the manubrium by the costoclavicular ligament, particular, via the costal cartilage.
Movements
The sternoclavicular joint can move in a variety of ways and is very mobile. These movements include:
- Elevation of the shoulders: shrugging them or extending the arm past 90 degrees
- Shoulder depression can manifest as drooping shoulders or extending the arm behind the body at the shoulder.
- This anterior displacement of the shoulder girdle is called protraction of the shoulders.
- The movement of the shoulder girdle posteriorly is known as shoulder retraction.
- The passive rotation of the clavicle and scapula occurs when the arm lifts over the head.
Clinical significance
Dislocation
Although sternoclavicular dislocation is uncommon, it can happen as a result of indirect forces applied to the shoulder or direct trauma to the clavicle. Surgical intervention may be necessary to correct posterior dislocations, as self-healing is not likely to occur. These dislocations pose a life-threatening risk due to the potential damage they may cause to critical tissues in the mediastinum. Occasionally, there may also be a spontaneous partial dislocation.
Arthritis
The SC joint may have osteoarthritis, which can cause discomfort, edema, and restricted movement. This is particularly prevalent in senior citizens.
Costoclavicular Syndrome
This disorder compresses the neurovascular systems beneath the collarbone, which frequently results in upper limb discomfort. Postural problems or repeated activities may be linked to it.
Sternoclavicular Joint Pain
Tendinitis or bursitis are two conditions that can produce pain at the SC joint, which can interfere with daily activities and arm movement.
Post-surgical Complications
Shoulder and thoracic surgery can affect the SC joint, resulting in problems or changed biomechanics.
Infection
Infections in the SC joint are rare, although they can happen, especially in immunocompromised people or after intravenous drug usage.
FAQs
How does one define the sternoclavicular joint?
Sternoclavicular (SC) joints interact the clavicle (collar bone) to the sternum (breastbone). The only joint that supports the shoulder and joins the arm to the body is the SC joint.
What kind of joint is the sternocostal joint?
Osteochondral joints, also called costosternal articulations or sternocostal joints, are synovial plane joints that connect the sternum to the costal cartilages of the happen ribs. The first rib is the sole exception, as its cartilage forms a synchondrosis joint with the sternum right away.
Sternoclavicular joint palpation: how to do it?
Pressing one hand laterally from the manubrium and following the clavicle medially can allow you to feel the SC joint. The patient should be supine for the best evaluation of this joint.
Does the sternoclavicular joint exhibit stability?
The sternoclavicular joint is largely stabilized by its ligaments. Four primary ligaments are identified: The anterior and posterior sternoclavicular ligaments support and strengthen the joint capsule on both sides.
What does the sternoclavicular joint consist of?
Its two sections are separated by a fibrocartilage-based articular disc. The superior surface of the costal cartilage of the first rib, the clavicular notch of the sternum, and the sternal end of the clavicle interact to form the joint.
The sternoclavicular joint is acted upon by which muscles?
The clavicle’s interposing muscles, the sternocleidomastoid, trapezius, deltoid, and pectoralis major, control how the SC joint moves.
What is the sternoclavicular joint’s depression?
Assumed values for the elevation and depression are 45 and 10 degrees, respectively. A strain on the subscapularis muscle and the costoclavicular ligament prohibits the elevation. It has been proven that bone contact with the front rib, the interclavicular ligament, and the superior sternoclavicular ligament improves depression.
How much movement is permitted at the sternoclavicular joint?
The sternoclavicular joint can move in three different ways: axial rotation, elevation-depression, and protraction-retraction.
References
- Epperson, T. N., Black, A. C., & Varacallo, M. (2023, November 17). Anatomy, shoulder and upper limb, sternoclavicular joint. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK537258/
- Wikipedia contributors. (2024, August 26). Sternoclavicular joint. Wikipedia. https://en.wikipedia.org/wiki/Sternoclavicular_joint
- Sternoclavicular joint. (2023, October 30). Kenhub. https://www.kenhub.com/en/library/anatomy/sternoclavicular-joint

One Comment