Torticollis of The Neck (Wryneck)
What Is Torticollis?
Torticollis, commonly known as “wryneck,” is a condition characterized by a twisting or tilting of the neck, resulting in the head being held in an abnormal position.
When your infant has torticollis, his head twists and turns to the side due to the muscles in his neck. Also known as Wryneck. It may be acquired or congenital. Swelling and stiffness in the neck muscles are symptoms. The symptoms of torticollis vary according to the cause of the disease, as there are several varieties. Positional corrections and mild muscular stretching are typical forms of treatment.
Ninety percent of persons are expected to have at least one episode of torticollis throughout their lifetime. Torticollis is a frequent diagnosis. Congenital torticollis is a benign form of the condition, although it can also result from more catastrophic conditions including brain damage. longer in the body. Babies that are between 19.7 and 20.4 inches long have an 88% increased chance of torticollis.
When a newborn has torticollis, the muscles in his neck twist and tilt his head to one side. It might appear as though your baby’s neck is bent abnormally. They can have their chin tipped to one side and their head cocked to the other. The torticollis is represented by the Latin terms “tortus,” which means twisted, and “collum,” which means neck. In infants and kids, torticollis is a rather common condition. Torticollis may be congenital, meaning it exists from birth. Alternatively, it might come about later in childhood or infancy (acquired).
A prolonged stiff neck can cause pain in the neck and make it difficult to move the neck in certain ways, such as rotating the neck to the side. Medication and exercise can help treat this condition in its early stages and aid in recovery. Sometimes surgery is necessary to treat the illness. Early intervention is used to address this problem. For children in particular, this is accurate.
The majority of cases appear to be associated with focal dystonia, a disorder of the local neuromuscular processes. One of the most prevalent focal dystonias in adults is cervical dystonia, which results in tetanic contraction of the trapezius and/or sternocleidomastoid muscles.
The muscles that are impacted determine how the neck is shaped. It should be stressed that torticollis may not cause further alterations in the head and neck positions. A fixed or dynamic posture of the head and neck in the positions of flexion, rotation, and tilt can occasionally result in torticollis. Head twisting or tipping is caused by spasms of the sternocleidomastoid, trapezius, and other neck muscles, which are often more prevalent on one side.
This article teaches us condition-related exercises, including a stretching exercise that lengthens the muscles and gives them flexibility. muscular sternocleidomastoid. Additionally, you may learn the mobility exercise that gives your neck joint its usual range while maintaining face symmetry.
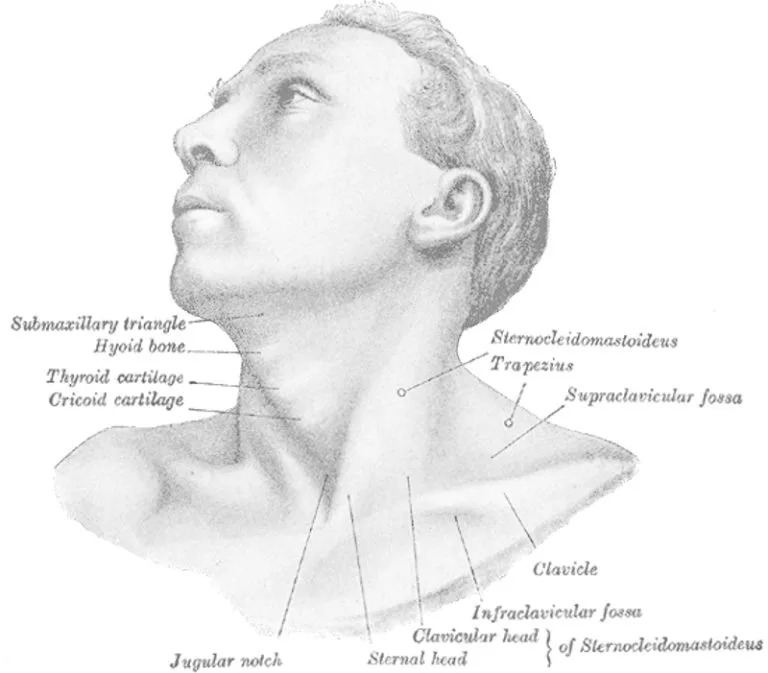
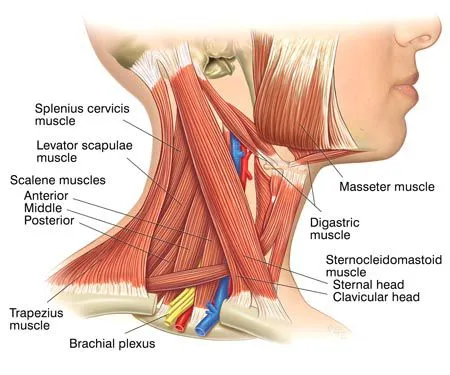
Anatomy of the Neck :
A shortened sternocleidomastoid muscle is the underlying anatomical deformity responsible for torticollis. This neck muscle begins at the clavicle and sternum and ends at the mastoid process of the temporal bone on the same side.
Humans have two sternocleidomastoid muscles, and when they contract together, the neck is flexed. The transverse scapular, transverse cervical, superior thyroid, and occipital arteries provide the majority of the blood flow to these muscles. The accessory nerve, or cranial nerve XI, provides the majority of the innervation to these muscles; however, the second, third, and fourth cervical nerves are also implicated. Torticollis can result from diseases in these blood and nerve supplies. of torticollis
Causes of torticollis
There are several etiologies for torticollis. It may be linked to severe or complicated illnesses. There are many varieties of torticollis:
Congenital torticollis:
Injury sustained during pregnancy or childbirth can result in muscular swelling and congenital fibrosis, which shortens the pectoral muscle fibers.
Congenital Torticollis often manifests as a hard mass that forms between 1-4 weeks of life. Ultrasonography and a color histogram are often used for diagnosis, alternatively, the infant’s passive cervical range of motion can be assessed clinically.
Most instances of torticollis recognized in clinical practice are congenital. Congenital torticollis has a reported incidence of 0.3-2.0%. At the age of two to four weeks, a lump, such as a sternocleidomastoid tumor, may occasionally be seen in the affected muscle. It eventually goes away, generally by the time the child is eight months old, but the muscle remains fibrotic.
Dermatogenic pain:
Usually associated with burns or scars, this neck pain can impede movement when the neck skin is damaged and shortened.
Ocular torticollis:
This condition is caused by the extraocular oblique muscles paralyzing the muscles responsible for compensating for head tilting and rotation.
Rheumatologic torticollis:
This variation develops as a result of many rheumatologic conditions. The cochlear labyrinth is part of the inner ear, or vestibular torticollis, which is in charge of balance.
Neurogenic tormentor:
Any neurological condition or trauma, including a stroke, can result in a neurogenic tormentor.
Spastic torticollis:
The most typical cause of stiff necks is spastic torticollis, also known as dystonia. The reason for this kind is increased muscular tone. The most frequent causes are abrupt movements, physical overload, and mental stress.
Acquired torticollis:
Noncongenital muscular torticollis can be caused by cerebellar tumors, swollen cervical glands, rheumatism, tonsillitis, adenitis, or illness of the cervical vertebrae. It might be persistent (tonic) or spasmodic (clonic). The latter type could result from spinal tuberculosis or Pott’s Disease.
The most common type of torticollis, known as “stiff neck,” is a self-limiting, spontaneously occurring condition that affects one or more painful neck muscles and goes away on its own in 1-4 weeks. Usually, either the trapezius or the sternocleidomastoid muscles are affected. Draughts, colds, or strange postures are occasionally blamed, but in many cases, no obvious reason is identified. Doctors frequently observe these events.
Torticollis can be caused by tumors of the posterior fossa, which compress the nerve supply to the neck. Surgical intervention is required to correct these issues.
If a posterior pharyngeal infection is not too serious, it may be treated with antibiotics; however, in situations where the infection is unmanageable, surgical debridement may be necessary. Torticollis is a condition caused by irritation of the nerves supplying the neck muscles.
Grisel’s syndrome, a subluxation of the upper cervical joints, primarily the atlantoaxial joint, is a result of inflammatory laxity of the ligaments caused by an infection and can be caused by ear infections and surgical adenoid removal.
Torticollis can result from using specific medications, such as antipsychotics. Many additional uncommon reasons can also lead to torticollis. FOP, or fibrodysplasia ossificans progressiva, is an extremely uncommon cause of acquired torticollis, characterized by deformed great toes.
Spasmodic torticollis:
Spasmodic torticollis is a kind of torticollis characterized by repetitive, fleeting contractions of the neck muscles, particularly the sternocleidomastoid.
Spasmodic torticollis is a kind of torticollis characterized by repetitive, fleeting contractions of the neck muscles, particularly the sternocleidomastoid.
Spasmodic torticollis is a kind of torticollis characterized by repetitive, fleeting contractions of the neck muscles, particularly the sternocleidomastoid.
Spasmodic torticollis is a kind of torticollis characterized by repetitive, fleeting contractions of the neck muscles, particularly the sternocleidomastoid. “Intermittent torticollis,” “cervical dystonia,” and “idiopathic cervical dystonia” are synonyms, depending on the underlying cause.
Trochlear torticollis:
Damage to the trochlear nerve, which feeds the superior oblique muscle of the eye, may be the cause of torticollis rather than the sternocleidomastoid muscle. The eye’s depression, abduction, and intorsion are all influenced by the superior oblique muscle. An extorted eye results from injury to the trochlear nerve, which impairs the function of the superior oblique.
Causes of torticollis
If the affected individual does not tilt their head away from the affected side, the extorsion of the eye will be balanced out by intorsion, resulting in visual issues. The Bielschowsky test, commonly known as the head-tilt test, involves turning the head to the side that is affected in order to identify this. An elevated, seemingly floating affected eye indicates a positive test.
Congenital thyroid muscle occurs when one of the baby’s sternocleidomastoid muscles (SCM) is shortened. The two big muscles in your neck are called your SCMs. They join the sternum (sternum) and clavicle (clavicle) to the rear of the cranium. Why certain children’s muscles shrink is a mystery to scientists. This might be because of:
- Dystonia
- There are situations where a baby is born breech—positioned outside of the mother’s uterus—and the origin of the condition is unknown (idiopathic).
- abnormal thickening of the muscular tissue (fibrosis).
- abnormal growth of the muscles of the sternocleidomastoid.
- You have mouth, neck, and head abscesses; your baby’s neck muscles have developed a mass of blood (hematoma).
- some illnesses, such as Parkinson’s (which causes spasms in the muscles).
- spinal abnormalities, including scoliosis, disc herniation, and modifications to the C1 and C2 vertebrae in the neck;
- onset of a neck muscular spasm that might be the result of a strained or injured muscle.
- In Klippel-Feil syndrome, the baby’s spine’s vertebrae bond together at birth.
- Some medications include conventional dopamine receptor blockers (phenytoin, carbamazepine, or metoclopramide).
Symptoms of torticollis condition:
- stiff neck
- Fever with headaches
- Head tremor Modifications in walking style A chin tilt to the affected side
- One side of your neck hurts
- Periodically forming a bulk
- the sternocleidomastoid muscle is either tight or thick.
- sensitivity in the cervical region
- Asymmetrical faces feature unequal shoulder heights, with one shoulder higher than the other
- incapacity to move your head (reduces neck range)
Other typical symptoms are often seen in babies with torticollis. Parents and guardians may see that their child possesses:
- difficulties placing the hands in the middle of the body.
- delayed visual development, including difficulties paying attention, tracking, and using both eyes simultaneously.
- issues with space movement planning (engine design). issues with quick movements (disorders of the inner ear or balance).
- After eating, pain is caused by reflux, which is the reflux of stomach acid back through the tube that connects the mouth and stomach.
- reduction of feeling in the hand and arm on the other side of the stretched muscle.
- reduced or absent protective responses when a stressed side loses equilibrium.
- increased trunk lateral flexion (bending to one side) on the side where the muscle is stressed.
- reduced eye movement toward the narrow side during visual tracking.
- loss of muscular strength in the non-longer side of the muscle. Late fall on both sides or better still, only on the long side that is not constrictive.
Differential Diagnosis:
- Fourth cranial nerve palsy.
- Sandifer of spasmus nutans Syndrome.
- Myasthenia Gravis.
- Since specialized imaging methods typically fail to identify a cause, it has been assumed that adult-onset cervical dystonia is idiopathic in origin.
How is torticollis diagnosed?
It may be required to get an MRI or X-ray if a kid is suspected of having torticollis and underlying bone problems in order to confirm the diagnosis.
Medical history
To assist in identifying the type of torticollis your child has, the doctor will first ask you a number of questions. Possible inquiries are:
- What age is your child?
- When was the onset of torticollis?
- Did the torticollis appear slowly at first or suddenly?
- Has there been any head or neck trauma?
- Is your child experiencing a fever?
- Does your child have a sickness?
- Has your child undergone neck or head surgery?
- Do you currently have any additional symptoms?
- Has your child had any exposure to drugs or medications?
Medical examination
The type of torticollis the child has will be determined by a thorough physical and neurological examination conducted by your child’s physician. During this examination, the jerky neck and head movement will be controlled, and the SCM muscle in the neck will be palpated (examined by touch) to check for a small lump, or “pseudotumor,” which affects about one in three instances of congenital muscular thyroid disease.
checking for signs of a disorder termed plagiocephaly, which is defined as the presence or absence of facial and head asymmetry or asymmetry (this is vital to assess since a baby’s head and face might develop unevenly owing to the gravity of a tilted head).
Examine your infant’s hips and their rolling gait, as hip dysplasia is a little more common in newborns with muscular spines.
In addition, your physician could prescribe further imaging tests, such as an ultrasound, to check for anomalies in the spine that might suggest uncommon but severe health issues.
The first step in evaluating a child with torticollis is to take their medical history in order to rule out any possible trauma or related symptoms as well as any particulars following their birth. Reduced rotation and bending to the side opposing the injured muscle are observed during a physical examination.
A complete neurologic examination should be included in the physical evaluation, and any potentially associated diseases like clubfoot and hip developmental dysplasia should be looked at.
To rule out any visible bone abnormalities, radiographs of the cervical spine should be taken. If structural issues or other disorders are an issue, an MRI should be taken into consideration.
Muscle tissue may be seen by ultrasonography, which also produces a color histogram that shows the cross-sectional area and muscle thickness.
Children should be evaluated by an optometrist or ophthalmologist to make sure that visual issues (IV cranial nerve palsy, nystagmus-associated “null position,” etc.) are not the cause of the torticollis.
Treatment for torticollis:
Physiotherapy treatments include manipulation to promote symmetry, strengthening exercises to improve muscle balance, and stretching to relieve tension. Sometimes a TOT collar is used. Starting therapy as soon as possible is crucial for complete recovery and lowering the risk of relapse.
Physiotherapy Treatment:
One non-invasive, low-cost method for treating torticollis is physiotherapy. Congenital torticollis can be reversed at home with the help of a parent or guardian, while outpatient physiotherapy continues to be an effective treatment for the condition in babies. For the greatest outcomes for their child, physiotherapists should work with parents to develop a home treatment plan and to stress the value of their involvement in the child’s care.
Early stages – mild cases:
Physical therapy can be used to manage children with modest deformities who report early for treatment.
The methods used in physical therapy are:
- Evaluation: Thorough assessment of the degree of deformity and ROM.
- Massage: Before doing stretching exercises, massage can help relax the muscles.
- Hot Pack Therapy Modality: This kind of thermotherapy promotes relaxation when used carefully.
- Passive movements: A pillow is put beneath the child’s thoracic region to position the head over the table edge while the child’s neck is extended. An aide stabilizes the child’s shoulders.
All of the cervical spine’s motions are gradual, passive, and relaxing in order to promote relaxation.
A prolonged passive stretching exercise to the sternomastoid that is impacted should come next. For example, when the right sternomastoid is implicated, the head should be progressively rotated to the right and then kept in an inside flexion position to the left for a period of time. In order to achieve more stretching, apply gentle traction and try to get as much overcorrection as you can.
After the repair is made, it must be maintained. It must be upheld by holding or maintaining a weight cuff passively.
It is possible to use the same technique on the following visits.
The simplest method to do active correction is to help the child’s head follow an item that has been moved in the right correctional arc. The colorful, sound-producing item is perfect for drawing a child’s attention.
PNF: Patients who have neck extensions might benefit from using traction and stretch.
Program for at-home therapy: This takes on a significant function since these modifications must be made again. For this, the mother has to be correctly instructed. The optimal approach involves placing the kid in a prone position, instructing the mother to gently tilt the head towards the affected side, and encouraging the child to cast a backward look over his right shoulder.
Positioning: It’s important to place the head precisely during sleep. In order to get the best possible posture when sleeping, a child should be compelled to rest on the side with the lesion opposite from the lesion, with their head supported by a pillow or sandbag. There are two benefits to this positioning: First, during sleep, muscles naturally relax. Secondly, whatever adjustment is made is preserved for a longer amount of time. The mother should, nonetheless, periodically verify the modifications.
Older children and adults: As people mature, deformities become structured and resistant to conservative care.
Exercise for Torticolis
- Sternocleidomastoid muscles strech
Right where your collarbone is, using two fingers, gently push the region of your Sternocleidomastoid muscle. Just move your head sideways and bring it forward to find the Sternocleidomastoid muscle. The muscle called the Sternocleidomastoid should protrude. This muscle extends from the collarbone (the area just behind your ear) to the sternum.
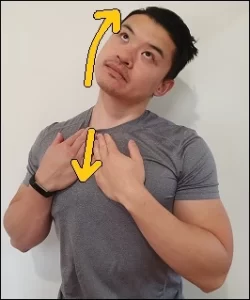
Put your ear on your shoulder and place one hand on the other side of your head. To maximize the stretch, be sure to grip the Sternocleidomastoid muscle above the collarbone with the opposite hand (two fingers). Raise your head and point at the ceiling now. Use your hand to move your head back and to the side to lengthen the stretch. It is required to hold the end range of motion for 15 to 30 seconds, but you may also progressively extend the stretch time if necessary. Take regular breaths throughout this phase. Work on the neck’s two sides. Avoid the stretch if you are in any pain or discomfort. As soon as you sense discomfort, stop it.
- Scalene stretch
The primary component of the neck muscles, the scalene muscles are prone to strain and discomfort if improperly stretched. The muscles that run down the sides of the neck aid in supporting and rotating the head. Raise your hands straight over your sternum and place them on top of one another. Next, tilt your head forward and away from the side that hurts until your neck begins to slightly extend on both sides.
Do this exercise twice or three times to reap the maximum benefits. Make an effort to do one or two sets of each exercise while holding each posture for around thirty seconds. For optimal effects, make sure you perform these exercises twice a day.
Stretching the scalene muscles can help you become more mobile and relaxed. In addition to keeping you energized, scalene stretches help increase flexibility and circulation in the back, shoulders, and neck regions of the body.
- Forward head pull

The muscles that run down the back and sides of the neck may loosen up with the aid of this stretch. If the torticollis pushes its head to the side or back, this is helpful. Putting your right hand behind your head, stand close to the counter. With your other hand, provide support to the plinth’s edge. Your head should be moved slowly to the right, between 30 and 45 degrees, and held there for five to ten seconds.
Your shoulders and neck should feel tense. To extend the stretch further, push your head lightly with your right hand if you can. If you feel comfortable, you can extend the hold time.For five to ten seconds, hold the end of the range of motion. To extend the muscles on the other side of the neck, you can perform this exercise in reverse. Perform three sets of three to five repetitions each day.
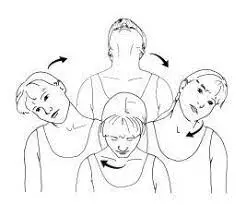
- Side neck rotation

By extending your neck forward during this activity, you can make it simpler for the person on the other side to reach for interesting objects or toys. Your neck muscles will feel somewhat stretched. This stretch helps increase the range of motion by focusing on the sides of your neck.
After the exercise, keep your shoulders and hips forward. Start by focusing directly ahead. Slowly turn your head to the left. Return to the starting position after holding for 10 seconds. Next, slowly turn your head to face the other side.
Hold the movement’s end range for the whole 10 seconds. Go back to where you were before. Every day, do three to five sets of eight to ten repetitions. Exercises like these are beneficial for those who have just developed torticollis, particularly if you have to maintain the position as it will help the problem initially. The exercises for side neck rotation can be done every 30 minutes to improve neck joint mobility.
- Lateral bending
These stretches aid in opening up the neck’s sides and shoulders. Place your arms at your sides as you begin to stand or sit. Pull your shoulders back and down and flex your abs to keep your spine straight.
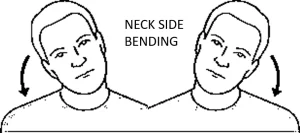
Maintaining the same posture for your shoulders, slowly bend your neck to bring your right ear up to your right shoulder. Hold this posture for a duration of five to ten seconds. Proceed to the left. Perform a set of two to four reps for every side. By applying gentle pressure on the head with your palm, you may extend the stretch farther.
Stretch the Sternocleidomastoid muscle by gradually elevating your chin when it feels comfortable. This stretch helps increase the range of motion by focusing on the sides of your neck. Throughout the exercise, keep your shoulders and hips forward.
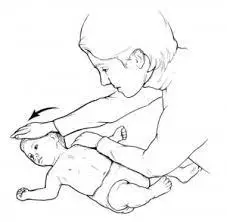
- Gentle Head Rotations
Another torticollis exercise that works well with the plinth is placing the baby on his back. If the baby tries to turn his head to the left, place your left hand on his right shoulder and hold the shoulder on the yoga mat or plinth. With your right hand, gently move the child.
Once more, maintain the stretch for five to ten seconds, and then give your child another five to ten seconds to unwind. Perform five sets of this every day, five to ten times a session. Put your right hand on the and move the head to the right if your baby has difficulty turning to the right. The collar joint might move because of the genital rotation of the head. the left shoulder of the infant.
- Lateral Neck Flexion Strengthening
Your baby will likely keep his head high when he is three or four months old, but if he has torticollis, he could choose to rotate to the side. Hold the infant upright with their head slightly bent toward the opposite side to strengthen that side of their neck.
It is better if the strengthened side is more horizontal. Your child is forced to exert effort to maintain his coolness. The angle can worsen if the child’s head falls back to the narrow side and they are unable to maintain their neck against gravity. If you see that the baby’s head is hanging, you should adjust the baby’s body angle so that it would be easier for them to hold their head up. Each time you carry your child, do this to strengthen the muscle in the side of the neck.
- Crib Exercises

Re-positioning the crib is a useful method to get a baby to move their head more. Once the child is old enough to sit, set him on the bed, bend his head to the other side, and hold or position the toy slightly above him.
This is good for newborns who have torticollis because it stimulates your baby to turn and tilt their head and neck in a way that facilitates healthy stretching.
Try to hold it for five to ten seconds, like with the previous exercises, and then take the toy away so the child can relax. Aim for six to ten repetitions of this crib exercise each day.
For a newborn with torticollis, these easy exercises can be really useful. It’s crucial to consult a doctor if you’re not certain of what to do if your child has torticollis in order to determine the severity of the condition and whether there are any other treatment options available than at-home exercises.
- Tummy Exercises
Monitoring a baby’s tummy time at frequent times throughout the day is important. Playing on his stomach with his toys during diarrhea exercises is an ideal way to soothe a baby with pain.

To get a child to tilt their head to the unattractive side, place all of their toys there. Before taking away the toys and letting the kid return to a comfortable posture for a little while, try to encourage them to stay in this position for five to ten seconds. To prevent your child from being irritated, try doing this five or ten times.
- Exercises on Therapy Ball
This is a session for strengthening. The muscles in the upper extremities, back, trunk, and head/neck are all treated by this exercise. When engaging in strengthening exercises, be mindful of imbalances and compensatory movements.
Use the therapeutic ball for tummy time practice.

Beginning with the child providing support at the trunk, progressively roll from front to back and from side to side.
To encourage alignment, you can also hold the mirror in front of the child.
To strengthen and stabilize the child’s trunk, do therapeutic ball work while they are sitting.
Reduce help as the child grows more independent.
- Shoulder Shrugs
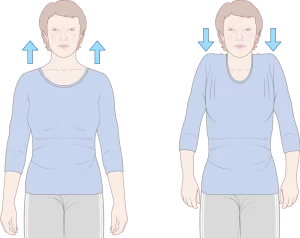
Another excellent physical therapy exercise for spastic torticollis is the shoulder rise. To run it, do the following actions:
With your chin parallel to the floor, take a straight seat or stand. Raise your shoulders slowly to your ears, then stay there for five seconds. Next, gradually reduce them. Do three to five sets of this workout every day and three to five repetitions every session. The neck muscles are strengthened and relaxed via shrugs.
You may lessen discomfort and straighten your posture in this way. For the course of the condition’s evolution, you can use shoulder shrug workouts, which improve your body’s posture.
Visual exercise for torticollis
- Visual Tracking
Promote eye tracking by making fluid motions to the left and right.
give stimulus from objects that are both visual and audible.
Promote visual tracking when in any of the following developmental positions: quadruped, prone, side-lying, supine, and supported sitting.
- Transferring Weight on a Therapy Ball
Shifting position when sitting, prone, or supine using a ball to distribute weight.
You may adjust the shoulder strength and stability in prone resting and the trunk strength and stability in sitting by using an incline wedge during the progression stage.
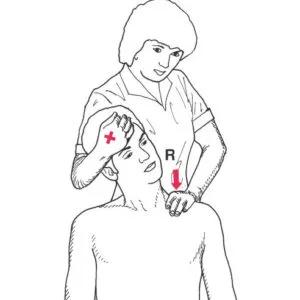
Massage
Once the infant has had a mild massage, you may begin the exercises.
The process involves lightly pressing the thumbs into the sternocleidomastoid muscle’s tight areas and running fingers down the muscular belly (highlighted above in red). The primary advantages of massage therapy are decreased muscular tension and increased range of motion and flexibility.
The sternocleidomastoid muscle, which rotates and tilts the head, is the main target of treatment. It is stretched and mobilized. The idea is to stretch the sternocleidomastoid muscle longitudinally and transversely, being cautious not to compress the carotid artery, by first relaxing the tissues and then working deeper into the muscle with the fingertips, knuckles, or palm.
Considerations and Indications for Massage Therapy for Torticollis
- If the vertebral artery test is positive or if the client has vertigo after performing the stretch, avoid performing complete Sternocleidomastoid muscle stretches.
When treating the sternocleidomastoid muscle, stay away from the carotid artery - Acutely acquired: utilize a less forceful approach, such as local rectal massage, for children with spasmodic torticollis; do not passively stretch the cramping muscle.
- Positioning for Play for Babies with Torticollis
- The shoulders, back, and core postures assist in strengthening your baby and are good for regular development.
- They stimulate the baby’s head and neck muscles. Either sit the baby on your lap, hold them facing out, or both. In order to get your child’s attention, point toys and lights to the right. With your right hand, bring their body forward and hold it against yours. With your left hand, encourage a mild stretch while keeping your head directed to the right. Hold for 15 to 20 seconds, then repeat 2 to 3 times on a regular basis throughout the day.
- Rotation (vertical)
Arrange all of the baby’s toys such that he must turn his head to the right while he is on his tummy. Once per hour, begin with 30 seconds, then progressively extend it for as long as you can. To make it simpler to raise and utilize the baby’s head, try exerting a little more pressure by placing your hands on their hips and bottom. If the infant is at ease, you can place his head on the right side. Your child should always go to sleep on their back and should never be left unsupervised in this position.
- Tummy time
To play, place the child on his right side. The arms are brought to the center of the body and a portion of the neck is stretched by gravity in this posture. A critical stage in the development of your baby’s hand-eye coordination, feeding skills, and other areas is bringing the hands to the midline.
Other Suggestions
Place them with their heads turned to the right while they are sleeping.
Place the child in such a way that the things going on in the room stimulate him to turn his head to the right.
When feeding the infant, try to get them to sit up straight. Place the infant on its right side while holding it on your shoulder.
A car seat should only be used when traveling or in a vehicle. You may store the child’s head in a neutral posture more easily by using quilted baby blankets and towels, as your therapist can teach.
When your child is playing, place him on his side to motivate him to play with the toys by raising his arms to his midline. Hold the baby on his abdomen.
To assist the child in turning his face to the left while playing, place the toys to the left.
Carrying your child (the football hold)
Don’t let a child get around you. With your right hand, place it between the child’s knees to support their torso as you hold their left shoulder. To assist the release of stiff muscles, put your left arm or hand between the child’s shoulder and ear.
Advice: To get the infant to look to the left, put them in the cradle. The infant is facing left when in the bottle/nursing position.
Your child’s head should be kept in a neutral position (car seat, high chair, rug) with the use of a towel. Speak with your physical therapist or occupational therapist in treatment if you have any questions or problems.
Helping Your Baby at Home
Teach the child to look both ways with his head. It aids in strengthening weak muscles and relaxing tight neck muscles. when a baby’s neck aches prevents them from trying on their own when they are unable to lift their heads. Here are some activities to attempt:
Offer a bottle or breast to a baby in a way that motivates him to turn away from his preferred side when he wants to nurse.
Your baby will sleep better if you hold him up against a wall. The baby will actively turn away from the wall since they prefer to stare into the space, which will stretch the muscles in their necks. To avoid SIDS, always put newborns to sleep on their backs.
These Modifications may include :
For the best neck alignment, the car seat’s neck supports should be added.
Cutting down on time spent motionless Using toys to help the kid look in the direction of restricted neck movement
When nursing or using a bottle, switch sides.
promoting fun when prone (tummy time). Parents should nevertheless make sure that their newborns spend some awake hours on their stomachs, even if the Back to Sleep campaign advocates for infants to sleep on their backs in order to prevent sudden infant death syndrome while they sleep.
One sternomastoid muscle malformation or incorrect neck positioning within the uterus might result from a developmental problem. The main contributing component is the sternomastoid’s shortening. The scalenii, platysma, splenius, or trapezius muscles may all shorten in tandem. Girls are more likely to experience it, and the affected side is often left. It might occasionally be bilateral.
Benefits of physical therapy for Torticollis condition
Simple posture adjustments may be made at home with these physical therapy stretches and exercises to help strengthen your child’s neck muscles and instill preventative behaviors.
- Flexibility of movement
When a baby is born, if he or she wants to rotate their head in one direction, purposefully keep them on your chest and tilt their head in the other direction for a comfortable and gentle stretch. Depending on your child’s degree of injury and neck stretch tolerance, see a certified pediatric physical therapist for advice on further torticollis stretches.
- Exercises for strengthening
Babies can the treated for torticollis and other conditions. Visit this blog to learn more about physical therapy for Torticollis! Having tummy time while swaying back and forth and side to side with a therapeutic ball. You can use toys, mirrors, dogs, siblings, and other objects to get the child to turn away from the prohibited area. To strengthen and stabilize your core, sit on the therapy ball, roll from side to side or front to back, and work with your kid to get back into a sitting posture.
To promote head movement and arm weight, place the infant on a soft wedge, cuff, or cushion (Boppy works great) to slow down tummy time. Reduce the size of the support to make it more difficult (pillow ? diaper cover on the roll ? tiny towel roll).
- Sitting activities
By putting the toy on the shorter side, you may encourage muscle rotation to the weaker side and weight transfer to the tighter side. The child frequently bends with the body or falls from the shorter side to the longer side when performing seated activities.
- Positioning
Positioning and managing sleeping and play areas: Spend no more than 15 to 20 minutes on swings, bouncers, and soft surfaces as they impede head and body mobility and, if used excessively, can lead to bad posture.
When your baby is to sleep on your side, you may easily move them off your back and play midline by bringing your hands to the center of your body. Use a cushion or a roll of towels to support them while they remain in this posture.
- Football hold (also known as a side carry):
Place your hand between your knees and your hand under your baby’s tummy, resting your shoulder on the shorter side of their neck. They attempt to hold their heads up in this position, strengthening the weak and long sides and extending the short side. Holding the infant far away and in front of you helps strengthen the neck and relieve pressure on the head. Until the infant can position himself and has strong head control, he should remain facing inward in the carrier.
- Position and Alignment
Putting weight on the ball by sitting, reclining on one’s back, or resting on one’s stomach.
Make sure to take the baby on its side before lifting it off the floor, baby, or changing table; alternate the baby’s sides frequently. We provide torticollis-affected children and newborns with physical therapy exercises and postural advice on our blog.
The environment
Make sure your baby is not staring in one direction all the time when you put him to sleep by turning his head. A further method to encourage this is to place the infant’s head at a different end of the cot every day. Every time you bottle feed (since nursing feeds your baby naturally!), swap sides and the hip you hold your baby on. Keep the kid away from places where the head is prone to rest all at once, such as car seats, booster seats, swings, trays, etc. During tummy time, move toys to the opposite side of the shorter side to help the infant turn his head.
Precaution while exercising for a baby.
- Take great care to respect your child’s tolerance.
- Gradually increase the movement.
- Choose the ideal time and position for your infant.
- Give these simple stretches a half-minute hold.
- If the child starts to object to the movements or gets cranky, stop worrying more quickly.
- Never let yourself feel as though you are pushing a movement.
- You may hold the stretch for as long as a minute if the child is really at ease.
- To amuse and soothe your child, use your voice or their favorite toys.
- Throughout the day, perform these stretches frequently: after baths, during playing, and/or after changing diapers. The objective is to do this eight times a day every two stretches.
- Give these simple stretches a half-minute hold. If the child starts to object or gets cranky, stop stretching early.
Medical Treatment
Medication and physical therapy (extending the SCM muscle and the scalene) are examples of non-surgical therapies. Stretching exercises include e.g. The child’s neck should be turned from side to side so that the chin hits both shoulders. The head should also be gently tilted to bring the affected side’s ear down to the shoulder. You should perform these exercises many times each day. You will learn how to perform the exercises from your child’s physician or physical therapist.
You can assist with other tasks at home:
Set up the toys so that the child has to turn to look at them. Keep your kids out of the restricted area. Place the crib and changing table so that your child has to look over the closed side to see you. When waking, position your for a short period of time (“tummy time”) to strengthen the muscles in your neck.
Surgical treatment
The surgeon may suggest surgery to treat your child’s torticollis if non-surgical measures fail to relieve it.
Surgery is necessary for about 10% of children with congenital muscle torticollis. When the kid enters preschool age, the procedure is often scheduled. Your child can have this outpatient operation, which lengthens the short sternocleidomastoid muscle, and return home the same day.
Surgical procedures include Near the origin, the sterna and the clavicular heads of the sternomastoid split, and the taut fascia is released. After that, the head is immobilized for two to four weeks in an overcorrected posture within a plaster cast. Immediately with the removal of the cast, mobilization starts.
Prognosis
For infants and young children, torticollis is a rather common problem. The issue is usually treated by moving your baby’s head and stretching their neck. Your infant should start to show some improvement in a few months. Early therapy should prevent any long-term problems for them.
Living with Torticollis condition:
A small injury or disease may occasionally be temporary and curable due to torticollis. There are two kinds of torticollis diseases that might cause long-term health issues: congenital and more severe. Complications from chronic torticollis might include:
enlarged muscles in the neck
neurological signs caused by pinched nerves
Prolonged discomfort challenges carrying out daily duties an incapacity to drive The socialization Isolation
Depression.
Conclusion
A head and neck in a tilted, rotated, or flexed position is the outcome of a torticulosus. Head twisting or tipping is caused by spasms of the sternocleidomastoid, trapezius, and other neck muscles, which are often more noticeable on one side than the other.
Numerous maxillofacial disorders and consequences can result from torticollis. The mandible may exhibit a lateral displacement that causes it to seem asymmetrical, leading to a permanent malformation known as mandibular retrognathism.
FAQ
Does physical therapy help with torticollis?
Additionally, the therapist will teach you daily posture and stretching exercises to perform at home with your kid. The following are the objectives of physical treatment for torticollis: Enhance your child’s left-to-right head movement. Boost your infant’s capacity to lift their chin up to their chest.
Can you fix torticollis at home?
Generally, a hot pack, pain medication, and neck massage can be used to treat torticollis. Seek guidance on positioning your torticollis-affected infant during eating and sleeping. It is also possible to train your head to move gradually in order to facilitate neck stretching.
Which exercises are most beneficial for babies with torticollis?
Head movement, lateral bending, neck side rotation, and SCM stretch Put a hand on the left shoulder of the young child. The shoulder is held in place. With the other hand, place it from the forehead to the chin on the left side of the child’s face. Turn the baby’s face to his or her right shoulder carefully and with caution.
Is torticollis curable?
For infants and young children, torticollis is a quite common condition. Treatment for the issue generally involves rotating the baby’s head and stretching its neck. You should see a change in your child’s condition in a few months. Early intervention in therapy should prevent long-term issues.
Can torticollis be temporary?
Temporary torticollis
This temporary issue might occasionally arise when your child has a cold or ear infection and their lymph nodes are heated and swollen (inflamed). Your child may potentially have torticollis if he has a head or neck injury. The neck’s intervertebral joints swell and hurt.
Is massage good for torticollis?
Improving cervical mobility and function in newborns with congenital muscle torticollis can be achieved safely and effectively with massage treatment.
Can torticollis be neurological?
It is typically a muscular issue that is readily resolved. In other cases, a neurological issue or infection is the cause of the illness. Certain individuals may be more prone to the illness due to a genetic abnormality. Treatment is available for torticollis in newborns, kids, and adults.
What is the cause of torticollis?
The reason may be damage to the neck muscles caused by the position of the developing baby within the uterus. A viral infection, an accident, or strong movement can irritate the cervical ligaments and result in acquired torticollis. Another potential reason might be sleeping in an uncomfortable posture.
Does torticollis go away?
The majority of infants with torticollis recover with positional adjustments and stretches. But exercise patience; it may take up to six months, or longer, to go away entirely.
Is torticollis curable in adults?
Torticollis can be treated with localized heat therapy, mild massage, and pain management. Usually, your symptoms go away within a week or so.
What is the duration of healing for torticollis?
How much time will it take to become better? More than half of individuals with torticollis get relief in 24 to 48 hours. On the other hand, some individuals may experience lingering soreness that takes up to six weeks to go away.
References
- Dhameliya, N. (2021, September 18). Torticollis of the neck : Symptom, Physiotherapy Treatment, Exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/torticollis/
- Prajapati, D. (2023, September 20). 13 Best Exercise for Torticollis – Fast Relief, Long-Term Results. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/13-best-exercise-for-torticollis/
- Professional, C. C. M. (n.d.). Torticollis. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/22430-torticollis




2 Comments