Radius Bone
Introduction
The radius is one of the two long bones that make up your forearm, along with the ulna. It is located on the lateral side of the forearm, which is the same side as the thumb. The radius plays a crucial role in the movement and stability of the forearm and hand, enabling activities such as lifting, rotating the wrist, and fine motor skills.
Radius and ulna make the forearm. It creates the radio-carpal joint at the wrist and the radio-ulnar joint at the elbow.
Structure
Proximal radius
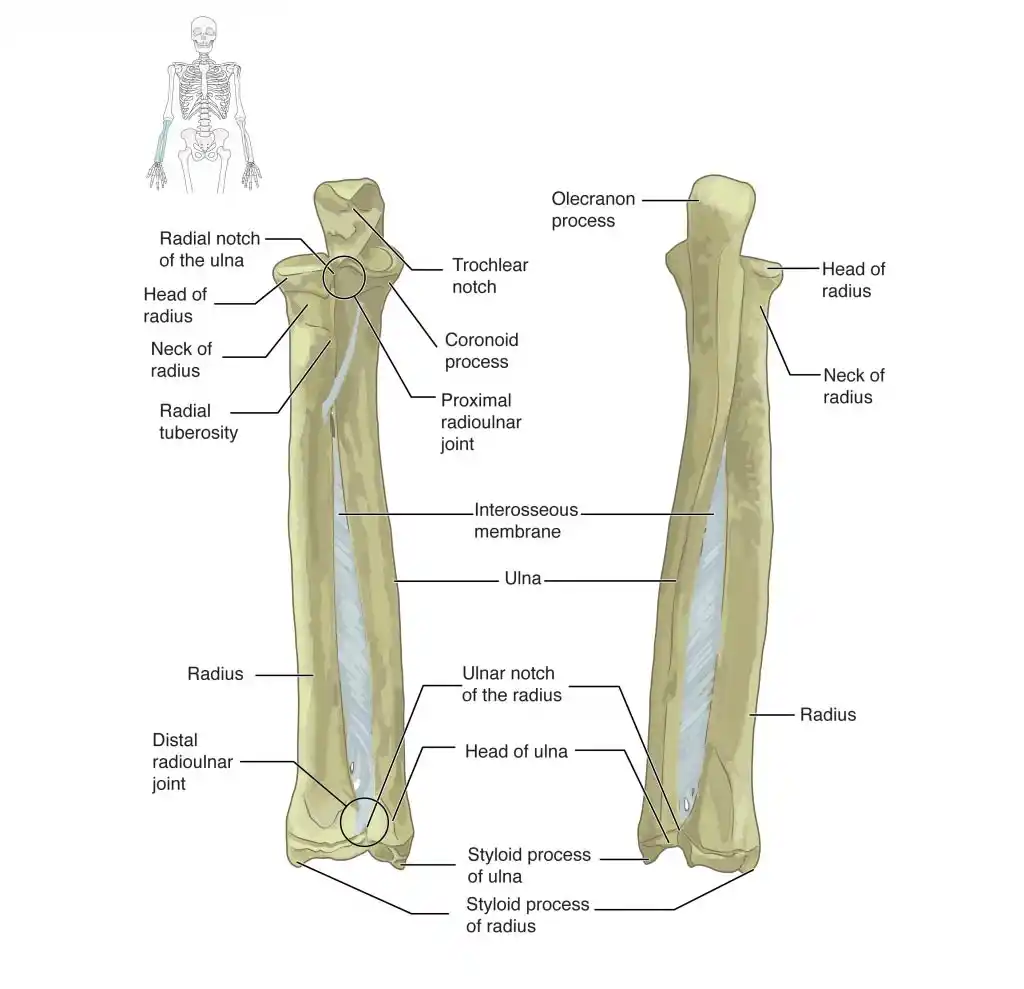
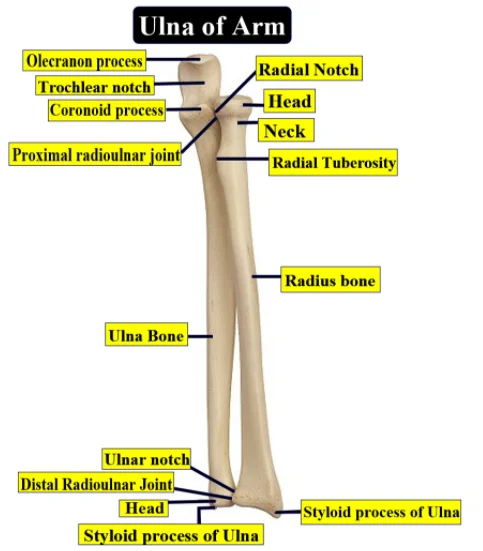
The proximal radius comprises the tuberosity, neck, and radial head.
The cylindrical radial head, which articulates with the humerus’s capitellum at the elbow joint, is covered with hyaline cartilage. The superior radioulnar joint is established when the radial head’s circumference precisely fits into the socket created by the radial notch of the ulna and the annular ligament. The forearm can supinate or pronate due to this joint’s ability to rotate the head inside the annular ligament.
The neck and tuberosity provide supinator brevis and Biceps brachi points of attachment, which also support the head.
Radial shaft
The radius shaft is convex from the body due to a very small degree of curvature. The majority of the shaft is surrounded by the anterior, posterior, and interosseous borders.
Distal radius
Five surfaces make up the distal radius
- Lateral: that grows to create the styloid process.
- Medial: has a concave ulnar notch that articulates with the pronating ulnar head.
- Posterior: the region is convex and features a noticeable ridge known as Lister’s tubercle.
- Anterior: The anterior region forms a boundary and is smooth, extending to the styloid process from the anterior border of the radial tuberosity.
- Distal articular surface: articulates laterally with the scaphoid and medially with the lunate.
Distal articular surface: articulates with the lunate medially and the scaphoid laterally.
At the wrist and elbow, it forms the radio-carpal and radio-ulnar joints. When in the anatomical position, it is situated in the lateral forearm and represents the tibia of the lower limb. The radius bone consists of a shaft, an upper end, and a lower end.
Function
The radius primarily articulates with the ulna and humerus to create supination and pronation at the elbow joint. After that, articulate with the scaphoid and lunate to allow complete wrist motions.
Articulations
Elbow
The ulna and radius articulate at a synovial pivot joint. Pronation of the forearm is caused by the radial notch on the ulna and the radial head rotating inside the annular ligament. The distal articulation of the ulna and radius, which occurs in the opposite direction of their elbow articulation, also results in supination. This motion happens when the ulna’s head goes through the radius’s ulnar notch.
Wrist
The radio-carpel joint is formed by the radius’s articulation with the first row of carpal bones, namely the scaphoid laterally and the lunate medially. Rarely does the triquetral bone come into touch with the ulnar abduction. The radio-carpel joint is an ellipsoid joint in which the convex surface of the scaphoid, lunate, and triquetral bones articulates with the concavity of the distal radius. The radio-carpel joint may move in the following four directions: ulnar, radial, and extension.
Embryology
The onset of endochondral ossification in the creation of the radius occurs in the lateral plate mesoderm, the earliest form of all long bones. Endochondral ossification is the process by which hyaline cartilage gives way to bone. Mesenchymal cells produced from mesoderm multiply quickly to become chondrocytes, which serve as a template for new bone formation.
Collagen and fibronectin are introduced to the matrix by chondrocytes in the model’s core, enabling calcification. Around week six of pregnancy, the calcification prevents nutrition from reaching the chondrocytes. At some point, the chondrocytes experience apoptosis. As chondrocytes leave empty spaces, blood vessels multiply and finally create the medullary cavity. The periosteal collar, a thick region of compact bone in the diaphysis that serves as the site of initial ossification, is formed by osteoblasts around the 12th week of pregnancy. Proliferating chondrocytes found in the epiphyseal plates (growth plates) at either end of the bone cause the bone to continue growing longer until adolescence. Sex hormones trigger the formation of secondary ossification centers during puberty, and the epiphyseal plates ossify together with the diaphysis.
Blood Supply and Lymphatics
The proximal radius receives most of its blood supply via the radial and radial recurrent arteries. The radial collateral and radial recurrent arteries anastomose as they move proximally.
The deep lymphatic vessels, which follow the deep veins like the radial, ulnar, and brachial veins, drain the lymph from the radius. The draining veins are the lymph nodes in the humeral axilla.
Nerves
The brachial plexus nerves innervate the forearm, providing it with motor and sensory functions. The extensor carpi radialis brevis, extensor carpi radialis longus, supinator, extensor carpi ulnaris, abductor pollicis longus, abductor pollicis brevis, extensor pollicis longus, extensor pollicis brevis, extensor indicis, extensor digitorum, and extensor digiti minimi are all supplied by the radial nerve, which also innervates the posterior forearm sensory innervation.
The muscles innervated by the median nerve include the flexor teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor pollicis longus, pronator quadratus, and the lateral part of the flexor digitorum profundus. Motor impulses are sent to the flexor digitorum profundus and flexor carpi ulnaris muscles by the ulnar nerve.
Muscles
Anterior compartment: The superficial layer muscles include the flexor carpi ulnaris, flexor carpi radialis, pronator teres, and palmaris longus. The deep anterior layer is composed of the flexor digitorum profundus, flexor pollicis longus, and pronator quadratus.
Posterior compartment: There are layers within the posterior compartment of the forearm as well as layers outside.The muscles of the superficial layer include the anconeus and extensor carpi ulnaris, as well as the extensor carpi radialis brevis, extensor carpi radialis longus, extensor digitorum, brachioradialis, and extensor digiti minimi.
Anatomical Variations
The proximal radio-ulnar synostosis is a deformity caused by the skeletal fusion of the proximal radius and ulna, in addition to examples of small, hypoplastic, or missing radial bones that have been recorded. The proximal portion of both bones is where fusion most commonly occurs The deformity is associated with a higher frequency of posterior dislocation of the radial head. Proximal radio-ulnar synostosis is linked to Cenani-Lenz syndactyly, Poland syndrome, and Cornelia de Lange syndrome.
Surgical Considerations
The metaphysis and epiphysis are fractured most frequently. Distal radial fractures most frequently happen when a patient falls on an extended hand, which causes the fragment to shift dorsally. More complicated fractures need to be seen by an orthopedic specialist, although these fractures typically heal without the need for surgery. In cases of ligamentous instability, carpal fracture, articular involvement, or volar displacement, a complicated fracture of the distal radius results. Often, surgery is required to heal these fractures.
Clinical Significance
Annular ligament subluxation, sometimes referred to as radial head subluxation or nursemaid’s elbow, is one of the most common pediatric injuries that orthopedics treats. It happens when a youngster under five years old has their hand or forearm suddenly pulled in a longitudinal direction. there is a sudden traction that pushes the radial head out from under the ligament, and it gets stuck between the capitulum and the radial head. The youngster frequently displays a pronated forearm and minimal bending of the elbow when presenting, failing to utilize the injured limb.
A distal radius Smith fracture is often caused by a direct blow to the dorsal wrist or forearm. Another way to get hurt is to fall on a flexed wrist. This fracture is displaced ventrally as opposed to dorsally as in a Colles fracture. In contrast to nursemaid’s elbow, which usually exclusively affects patients in their pediatric years, distal radius fractures typically affect people who are younger than 18 or older than 50.
A colles fracture also affects the distal radius. The most typical way that an avulsion fracture happens is when someone falls on an extended hand with their forearm pronated. The bone fragment has moved dorsally, and the annular ligament has subluxed. According to clinical descriptions, the damage results in a “dinner fork” or “bayonet” deformity.
Holt-Oram syndrome (HOS) is an autosomal dominant mutation in the TBX5 gene that results in heart and upper limb abnormalities. Upper-limb anomalies include the triphalangeal thumb or absence of thumbs, aplasia or hypoplasia of the radius, and fusion of the carpal and thenar bones. abnormal wrist adduction and abduction, as well as aberrant pronation and supination of the forearm, are caused by aplasia or hypoplasia of the radius.
FAQs
What is the function of the radius?
Radius permits adduction, abduction, extension, flexion, and circumduction of the wrist in addition to flexion and extension at the elbow, pronation, and supination of the hand and forearm. The complicated articulation that causes pronation and supination involves the cylindrical radial head, which is secured to the ulnar notch by the annular ligament.
Is the radius on the thumb side?
The radius and ulna, which make up the forearm, are found on the thumb and pinky sides of the body.
How do you treat a fractured radius bone?
Non-Surgical Care
A cast or splint may be utilized, depending on how well the distal radius fracture is positioned.
Can you move your hand with a radius fracture?
Even with a cracked bone, some persons are still able to move or utilize their wrist or hand. The wrist may seem twisted due to a misplaced bone or swelling. Pain when moving the fingers and close to the break is common. The tips of the fingers may tingle or feel numb.
How long is recovery from radius surgery?
Recovery Period
It takes around three months for a surgically repaired wrist or distal radius fracture to fully recover.
Reference:
Bair, M. M., & Gondal, A. Z. (2023, July 31). Anatomy, Shoulder and Upper Limb, Forearm Radius. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK544512/



2 Comments