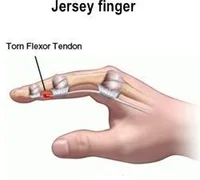
Jersey’s finger
Definition The Jersey finger, often known as the “rugby finger,” is an avulsion of the flexor digitorum profundus tendon (FDP) from the distal phalanx (zone I), where it is inserted. The most often impacted is the ring finger. In the gripping posture, the ring finger protrudes the farthest, making it more susceptible to FDP avulsion,…