Medial Pectoral Nerve
Introduction
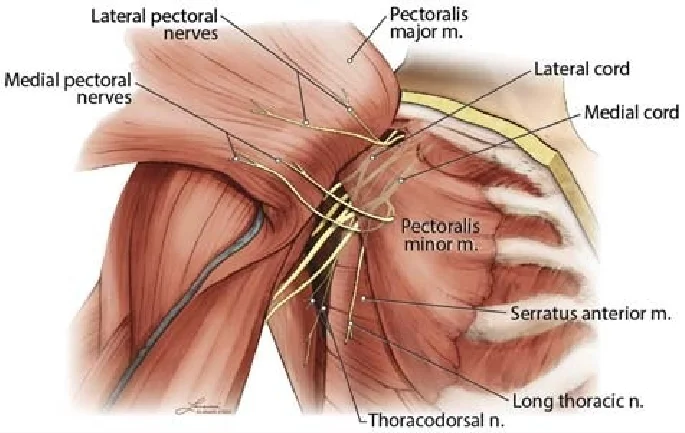
The medial pectoral nerve arises from the medial cord of the brachial plexus (C8-T1). It primarily innervates the pectoralis major (sternocostal head) and pectoralis minor muscles.
Unlike the lateral pectoral nerve, it pierces the pectoralis minor before reaching the pectoralis major. This nerve plays a role in shoulder adduction, internal rotation, and scapular stabilization.
Structure and Function
After arising posterior to the axillary artery, the medial pectoral nerve curves forward between the axillary artery and vein before receiving a communicating branch from the lateral pectoral nerve. The medial pectoral nerve then enters the pectoralis minor muscle, where it gives off multiple branches that supply the muscle, and then it passes through the pectoralis minor muscle to reach the pectoralis major muscle, which is made up of a clavicular part and a sternal part.
The function of the medial pectoral nerve is to extend the arm at the shoulder from a flexed position. With the scapula and upper limb locked, the pectoralis minor muscle, which attaches to the coracoid apophysis, aids in producing a medial rotation of the scapula against the opposition. Therefore, the inability to lift the shoulder may result from damage to the medial pectoral nerve. For forced inspiration, the pectoralis minor muscle can also function as an auxiliary muscle.
The medial pectoral nerve develops from the medial cord of the brachial plexus with C8 and T1 nerve roots. The medial pectoral nerve may emerge straight from the anterior portion of the inferior trunk of the brachial plexus. It has also been stated that the nerve originates straight from the brachial plexus’ main trunk.
This nerve branches into two primary patterns. In the most prevalent form, the nerve enters the pectoralis major by piercing the deep aspect of the muscle as a single trunk, ramifying within the muscle, and releasing branches that emerge on the superficial surface.
In the alternative arrangement, the nerve splits before it reaches the pectoralis minor, and its branches get to the pectoralis major by going through the muscle or around its edge.
Course
The lateral branch of the brachial plexus’s medial cord gives birth to the medial pectoral nerve (C8, T1). The origin of this is behind the axillary artery. The nerve originates along the axillary vein and axillary artery and travels anteriorly towards the pectoral muscles. The lateral pectoral nerve sends a communication branch to the nerve before it reaches the inferior edge of the pectoralis minor muscle, creating a nerve loop called the ansa pectoralis.
The pectoralis minor muscle is where the nerve partly stops. The lateral side of the muscle gives rise to some fibers that supply the pectoralis major muscle.
Muscle Supply
The medial pectoral nerve innervates the lower portion of the pectoralis major and the pectoralis minor muscle, which contributes to the thoracic-brachial motion. The pectoralis major is the most superficial muscle in the pectoral region and is a fan-shaped muscle that runs across the upper chest from the shoulder to the sternum.
The pectoralis minor muscle lies beneath the pectoralis major muscle and inserts superolaterally into the anterior scapula’s coracoid process and anteromedially into the third, fourth, and fifth ribs. The medial pectoral nerve may innervate the shoulder girdle’s accessory muscles, including the axillary arch, chondrofascialis, pectoralis quartus, axillary arch, chondroepitrochlearis, and sternalis muscles.
Branches
The pectoralis minor and a portion of the pectoralis major are supplied by two sets of muscular branches that emerge from the medial pectoral nerve, as was previously indicated.
The purpose of this particular pectoralis major muscle is to extend the arm from a flexed posture at the shoulder. As a result, the inability to raise the shoulder is frequently caused by damage to this nerve.
Embryology
The brachial plexus gives birth to the peripheral medial pectoral nerve. The ventral rami of C5 to T1 produce trunks that make up the brachial plexus. Anterior and posterior divisions of the trunks give rise to cords, which ultimately terminate as terminal branches. The neural plate, which folds in on itself to produce the neural tube, is formed when the neuroectoderm separates from the ectoderm.
This process is termed neurulation. The neural crest cells in the most dorsal part then move to various, occasionally remote, areas of the embryo after undergoing an epithelial-to-mesenchymal transition and delaminate from the neural tube. The sheath of the primordium of the arm muscles is located at the level of the humerus, where the primordium of the dorsal nerves stops.
Nerve extensions from C5 to T1 start to develop on day 32. On day 33, the nerves unite and the plexus brachialis starts to take shape. By days 49 and 50, it is evident that the plexus brachialis is orientated and provided similarly to the adult. The medial pectoral nerve emerges from its medial cord in a primitive brachial plexus, which is shown by the many anastomoses of the nerve roots from the fourth cervical through the first thoracic segment.
Anatomical Variation
Because medial pectoral nerve variations are less common than, say, lateral pectoral nerve variants, there aren’t many accounts of them. The medial pectoral nerve most often originates from the medial cord, although it can also occasionally originate from the anterior division of the lower trunk and, less commonly, straight from the brachial plexus trunk.
Although the medial pectoral nerve has been reported to originate from the anterior division of the middle trunk and the C6 root, it has not yet been reported to originate directly from the middle trunk of the brachial plexus.
Clinical Importance
Medial pectoral nerve injury
Direct trauma to the axillary area typically results in damage to the medial pectoral nerve. Furthermore, it may sustain an iatrogenic injury during surgery in this area (e.g., axillary node dissection, and breast surgery).
The degree of nerve damage determines the clinical presentation. Patients typically complain of shoulder aches or difficulty elevating their shoulders. Electrodiagnostic tests and imaging techniques like MRI are the most effective ways to make the diagnosis. Usually, conservative or surgical methods are used for treatment.
Surgical Importance
Direct trauma, muscular compression, and iatrogenic situations like breast surgery and axillary node dissection can all harm the pectoral nerves. Pectoralis major muscle transfers can potentially damage the nerve, yet nerve transfers can help with surgical recovery. At the level of the medial cord, the medial pectoral nerve can be surgically approached by the supraclavicular or infraclavicular routes. It is a desirable donor nerve for upper plexus injuries due to its high quantity of motor fibers, expandability, and surgical accessibility.
However, there are differing views about the medial pectoral nerve’s suitability as a motor donor for brachial plexus injury. When the medial pectoral nerve is used as a donor, there are reports of positive outcomes, such as the restoration of elbow flexion, shoulder abduction, and enhanced serratus anterior strength with transmission to the axillary, long thoracic, and musculocutaneous nerves, respectively.
As previously stated, the pectoralis minor muscle is the primary route for the medial pectoral nerve, albeit it occasionally leaves the body along the lateral portion of this muscle. A section of the innervation of the pectoralis major muscle may be disrupted if a surgeon does a dissection between the pectoralis major and minor muscles.
FAQs
What is the medial pectoralis major muscle?
The biggest and most prominent muscle in the anterior chest wall is the pectoralis major. The anterior wall of the axilla is formed by this thick, fan-shaped muscle, which is located beneath the breast tissue.
What is the function of the pectoral nerve?
The lateral pectoral nerve mostly carries motor fibers. Its primary role is to provide the pectoralis major muscle with motor innervation, while it also makes a little contribution to the pectoralis minor muscle.
What happens if the medial pectoral nerve is damaged?
With the scapula and upper limb locked, the pectoralis minor muscle, which attaches to the coracoid apophysis, aids in producing a medial rotation of the scapula against the opposition. Consequently, the inability to raise the shoulder may result from damage to the medial pectoral nerve.
How do you treat nerve damage in the shoulder?
Treatment for shoulder nerve damage depends on the cause of the injury and may include rest, medication, physical therapy, or surgery.
Rest Avoid sports and intense activity and Avoid heavy lifting.
Medication
Take pain relievers like acetaminophen, ibuprofen, or naproxen
Using NSAIDs, such as naproxen or ibuprofen, regularly
Take corticosteroids, either orally or as an injection
Physical therapy
Build muscle strength and flexibility
Do shoulder rotation exercises
Do shoulder and arm stretches
Do soft tissue mobilization (massage)
Do shockwave therapy
Do dry needling
Do taping
Do TENS treatment
Surgery Release a trapped nerve and Decompress the suprascapular or other identified nerve.
Can a massage help a pinched nerve?
Massage therapy may help relieve the pain associated with a pinched nerve, but it will not cure the underlying condition. If you do decide to try massage therapy, be sure to see a qualified therapist who has experience treating people with pinched nerves.
References
- Medial pectoral nerve. (2023, November 3). Kenhub. https://www.kenhub.com/en/library/anatomy/medial-pectoral-nerve
- Medial pectoral nerve. (2023, August 28). StatPearls.https://www.ncbi.nlm.nih.gov/books/NBK556059/