Lumbar Plexus
Introduction
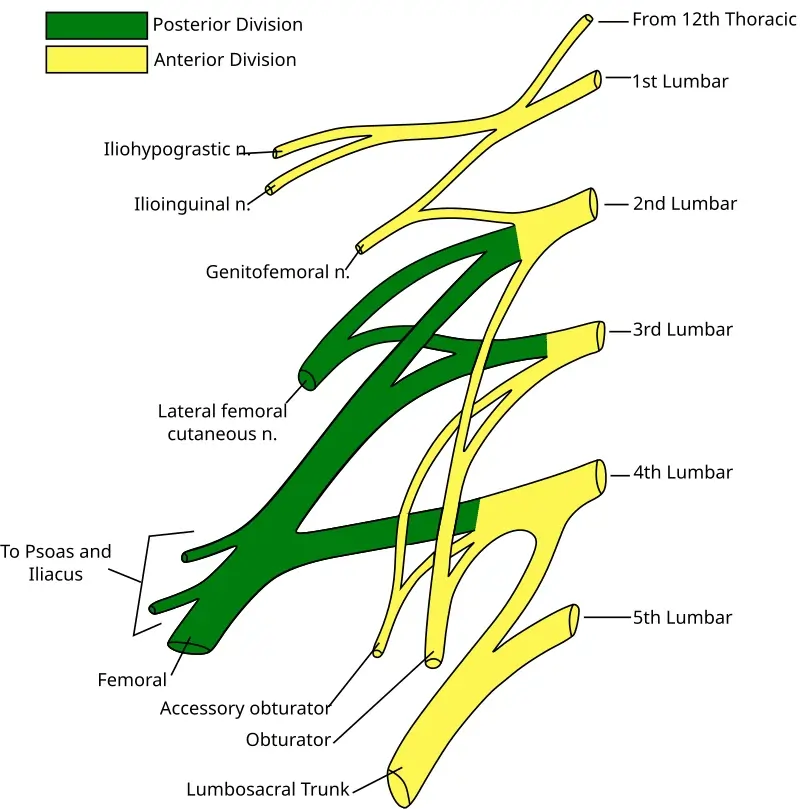
The lumbar plexus is a neural network formed by the anterior rami of spinal nerves L1 through L4 and the anterior ramus of spinal nerve T12. It is situated on the posterior abdominal wall, anterior to the transverse processes of the lumbar vertebrae, and inside the posterior section of the psoas major muscle.
The lumbar plexus gives rise to branches that nourish different muscles and areas of the posterior abdominal wall and lower limb. The branches are the iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, femoral, and obturator nerves. Furthermore, the lumbar plexus produces muscle branches from its roots, including a branch to the lumbosacral trunk and, in rare occasions, an accessory obturator nerve.
Root
The lumbar plexus arises from the anterior rami of spinal neurons L1-L4 and is mostly produced in the posterior side of the psoas major muscle. The dorsolumbar nerve connects the anterior ramus of spinal nerve L1 to the anterior ramus of spinal nerve T12, which helps create the lumbar plexus. These roots (T12, L1) create a single trunk from which the iliohypogastric and ilioinguinal nerves originate. The anterior rami of L1 and L2 each give rise to a branch, which goes on to unite with one another to produce the genitofemoral nerve.
As the spinal rami of spinal neurons L2–L4 travel out from the lumbar vertebrae, they split into anterior (ventral) and posterior (dorsal) divisions. The anterior divisions combine to create the obturator nerve. The anterior divisions of the L3 and L4 anterior rami may give rise to branches that connect to create an accessory obturator nerve. In contrast, fibers from the posterior divisions mostly combine to create the femoral nerve. The posterior divisions of L2 and L3 also produce branches that join to form the lateral femoral cutaneous nerve.
The anterior ramus of L4 gives birth to an extra branch that eventually merges with the anterior ramus of the L5 spinal nerve to form the lumbosacral trunk. The sacral plexus is formed when the lumbosacral trunk connects the anterior rami of sacral spinal nerves S1–S4 in the pelvis. Thus, this branch of the lumbosacral trunk connects the lumbar and sacral plexuses.
Branches
Unlike the brachial plexus, which experiences multiple distinct mergers and splits, the lumbar plexus is more complex. However, the primary branches of the lumbar plexus can be arranged into groups about the psoas major muscle. These branches arise either lateral, anterior, or medial to the muscle.
- Lateral: The iliohypogastric nerve, ilioinguinal nerve, lateral cutaneous nerve of the thigh, and femoral nerve
- Anterior: Genitofemoral nerve
- Medial: Obturator nerve, accessory obturator nerve, and nerve to the lumbar trunk
- Furthermore, the lumbar plexus generates multiple tiny motor muscle branches from its roots, which innervate the psoas major and quadratus lumborum.
Iliohypogastric nerve
The iliohypogastric nerve originates from the anterior ramus of spinal nerve L1, however it may get a branch from the anterior rami of T12. It emerges from the psoas major muscle’s superolateral border and travels anterolaterally over the lower posterior abdominal wall. This nerve is a mixed nerve that innervates both the internal oblique and transversus abdominis muscles, as well as the skin in the posterolateral gluteal and suprapubic regions.
Ilioinguinal nerve
The ilioinguinal nerve, like the iliohypogastric, originates in the anterior ramus of spinal nerve L1 and may also receive input from the subcostal (T12) nerve. It travels inferior to the iliohypogastric nerve in the same inferolateral direction. The ilioinguinal nerve is a mixed nerve that, like the iliohypogastric nerve, innervates the internal obliques and transversus abdominis muscles. The ilioinguinal nerve’s sensory fibers innervate the skin of the upper medial thigh as well as sections of the external genitalia.
Lateral cutaneous nerve of the thigh
The lateral cutaneous nerve of the thigh, also known as the lateral femoral cutaneous nerve, is composed of fibers from the posterior divisions of the anterior rami of spinal neurons L2 and L3. It arises from the lateral border of the psoas major muscle and travels inferolateral into the iliac fossa, eventually reaching the thigh. This nerve innervates the peritoneum of the iliac fossa and fascia, as well as the skin of the anterior and lateral thighs (along the iliotibial tract) and the knee.
Femoral nerve
The femoral nerve is the biggest branch of the lumbar plexus, generated by the posterior divisions of the anterior rami of spinal nerves L2–L4. It arises from the psoas major muscle’s lower lateral border, passing beneath the inguinal ligament and lateral to the femoral vessels before reaching the thigh. This is a mixed nerve that supplies motor and sensory innervation to the thigh and leg via multiple branches.
The femoral nerve supplies motor function to the following muscles:
Flexors of the hip: pectineus, iliacus, sartorius
Knee extensors: quadriceps femoris (rectus femoris, vastus medialis, vastus lateralis, and vastus intermedius).
The femoral nerve supplies sensory information to the following regions:
The skin of the anteromedial thigh.
Skin of the Medial Leg and Foot
Genitofemoral nerve
The genitofemoral nerve originates from the anterior rami of spinal nerves L1 and L2. The nerve begins on the anterior aspect of the psoas major muscle and proceeds inferiorly, splitting into two branches:
In men, the genital branch passes via the inguinal canal and sends motor fibers to the cremasteric muscle as well as sensory fibers to the higher anterior scrotum skin. In females, this branch innervates the mons pubis and labium majus skins.
The femoral branch is located posterior to the inguinal ligament and provides cutaneous nerves to the skin of the upper anterior thighs.
Obturator nerve
The obturator nerve originates from the medial border of the psoas major muscle and is comprised of the anterior divisions of spinal nerves L2 and L4. This nerve is mixed and reaches the medial compartment of the thigh via the obturator canal. The obturator nerve controls motor function in the obturator externus and hip adductors (adductor longus, brevis, magnus, gracilis, and pectineus). It also provides a sensory supply to the skin of the medial thigh.
Accessory obturator nerve
The accessory obturator nerve, if existent, arises from the psoas major muscle’s medial border. It is usually generated by the anterior rami of the spinal neurons L3 and L4. This nerve nourishes both the pectineus muscle and the hip joint.
Muscle Supply
The lumbar plexus innervates numerous key muscles. Notable muscles include the psoas, quadratus lumborum, lumbar transverse muscles, quadriceps femoris, transversus abdominis, and internal obliques. The psoas muscles, quadratus lumborum, and lumbar transverse muscles are innervated by nerves that originate straight from the plexus. The nerves emerging from the lumbar plexus innervate the remaining muscles.
Proprioception of the hip and knee requires innervation of the quadriceps. The vastus lateralis, vastus intermedius, and vastus medialis are innervated, allowing the central nervous system to receive proprioceptive information about the knee. The rectus femoris is innervated, which serves to convey proprioceptive information to the central nervous system regarding the hip.
Embryology
The neural plate serves as the foundation for the spinal cord. Neuroepithelial cells are responsible for the formation of peripheral nerves. These nerves play a role in the development of neurons, support cells, and axons that make up the peripheral nervous system. These are essential in the formation of peripheral nerve systems like the lumbar plexus.
When comparing fetal and adult lumbar plexus structures, the morphology stays comparable. Nerve thickness, length, and spinal nerve branching are shown to stay constant throughout development.
Clinical Importance
Injury to the lumbar plexus or nerves proximal and distal to it can cause a variety of diseases. Lumbar disc herniation can cause blockage of the intervertebral foramen, compressing lumbar spinal nerves at their entry to the lumbar plexus. This disorder can cause paraesthesia and weakness in places innervated by nerves of the lumbar plexus. Trauma commonly causes damage to peripheral nerves and the lumbar plexus.
The cremasteric reflex is an essential one to observe. The femoral section of the genitofemoral nerve and the ilioinguinal nerve supply the afferent fibers for this response. The genital branch of the genitofemoral nerve, which delivers motor innervation to the cremaster muscle, is in charge of the efferent. Stroking the medial thigh should produce contraction of the cremasteric muscle, resulting in a scrotal ascent. In cases of testicular torsion, the vaginal branch of the genitofemoral nerve becomes entrapped, and this response is absent.
A common and serious nerve compression condition can result from the lateral femoral cutaneous nerve, a branch of the lumbar plexus. This disease, known as meralgia paresthetica, is often caused by nerve entrapment when it travels under or through the inguinal ligaments. This illness might manifest as a painful syndrome affecting the anterolateral region of the thigh. Nonsteroidal anti-inflammatory medicines (NSAIDs), opioids, and anti-neuropathic pain medications can all be utilized to treat this disease; however, if the patient’s symptoms persist, surgical decompression may be considered.
Surgical Importance
The lumbar plexus and its ramifications must be considered while undergoing surgery. An anterior abdominal approach surgery might cause iatrogenic damage to superficial branches of the iliohypogastric, ilioinguinal, or genitofemoral nerves. These can be injured during surgery, causing paresthesias. The genitofemoral nerve is the most difficult to locate intraoperatively. Furthermore, iatrogenic injury to the lumbar plexus has been widely reported following a minimally invasive lateral retroperitoneal transposons procedure. This lumbar plexus injury is most typically associated with neuropraxia, which usually resolves within three months.
It is important to highlight that nerve blocks to the ilioinguinal, iliohypogastric, and genitofemoral nerves, as well as surgery, are options for managing treatment-resistant groin discomfort. In children who require inguinal hernia surgery, an ultrasound-guided erector spinae block outperforms an ultrasound-guided ilioinguinal/iliohypogastric block. An ilioinguinal transversus abdominal plane nerve block has been demonstrated to give more effective pain relief for individuals undergoing elective cesarean surgery.
Joint surgery on either the hip or the knee can cause proprioceptive dysfunction. Innervation of the muscle surrounding the joint, as well as innervation of the joint itself, is critical for transmitting proprioceptive information to the central nervous system. This feature of the joint should be considered when developing rehabilitation strategies for individuals who have had hip or knee arthroplasty.
FAQs
What are the six nerves in the lumbar plexus?
The nerves that originate from the lumbar plexus are iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, femoral nerve, obturator, and lumbosacral trunk.
How do the memorize lumbar plexus?
The nerves to remember are the iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, obturator, and femoral nerves. The catchphrase is ‘I (twice) get laid on Fridays’.
What causes lumbar plexus pain?
There are several causes of lumbosacral plexus injury. These include forceful impacts such as an accident, prolonged labor in childbirth, cancer, diabetes, and autoimmune diseases. Some cardiac procedures may also cause nerve damage.
References
- Lumbar plexus. (2023, October 30). Kenhub. https://www.kenhub.com/en/library/anatomy/lumbar-plexus
- Lumbar plexus.(2023, August 7). StatPearls.https://www.ncbi.nlm.nih.gov/books/NBK545137/