Infraspinatus Muscle
What Is The Infraspinatus Muscle?
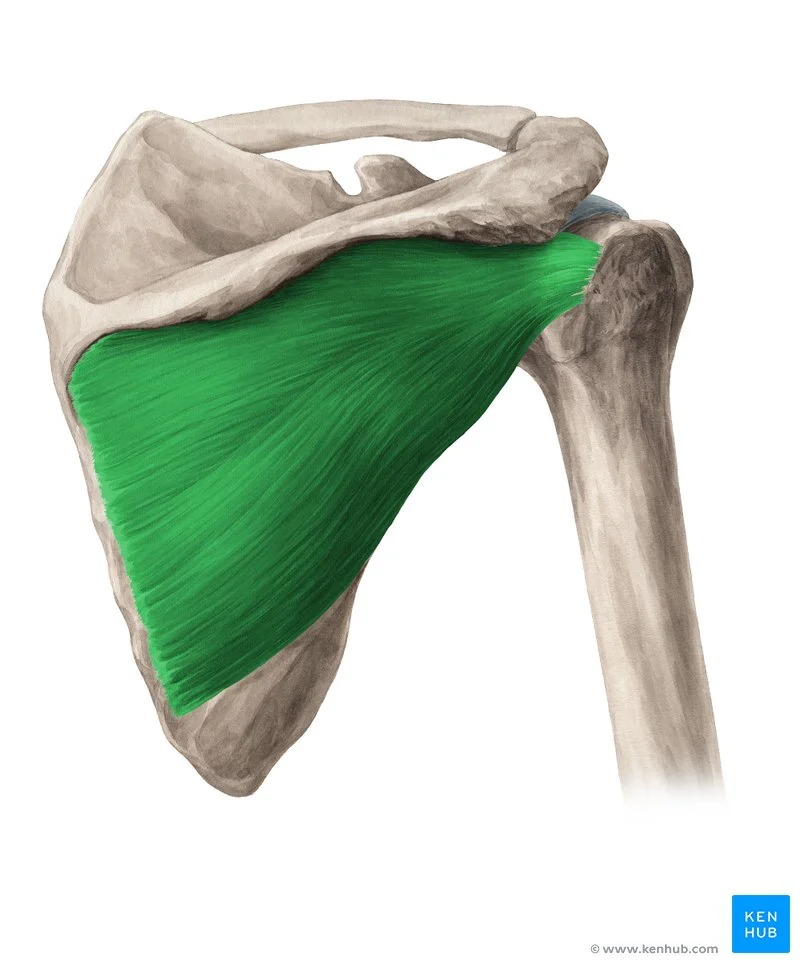
The infraspinatus muscle is a key anatomical structure located in the shoulder region of the human body. It is one of the four muscles that make up the rotator cuff, a group of muscles and their tendons that provide stability and facilitate various movements of the shoulder joint.
Thick, trapezoidal in shape, the infraspinatus muscle. This rotator cuff muscle serves as the mechanical connection between the anterior and posterosuperior regions of the rotator cuff.
The main portion of the infraspinatus fossa is occupied by the thick, triangular infraspinatus muscle in human anatomy.
The infraspinatus, one of the four rotator cuff muscles, is primarily responsible for stabilizing the shoulder joint and externally rotating the humerus.
This rotator cuff component is often recalled using the acronym “SITS” (supraspinatus, infraspinatus, teres minor, subscapularis).
The glenohumeral joint, which supports the stability and motion of the shoulder joint, is formed in part by these muscles. Despite being one of the most dynamic joints in the body, the shoulder joint is made stable by these muscles.
The primary muscles involved in scapulation, lateral humeral rotation, and external shoulder rotation are the infraspinatus.
Structure of the Infraspinatus Muscle
It connects laterally to the middle facet of the larger tubercle of the humerus and medially to the infraspinous fossa of the scapula.
The muscle is derived from the infraspinatous fascia that covers it and divides it from the teres major and minor. It also originates from fleshy fibers found in the medial two-thirds of the infraspinatous fossa and tendinous fibers found in the ridges on its surface.
The fibers come together to form a tendon, which is inserted into the middle impression on the larger tubercle of the humerus after gliding across the lateral border of the scapula’s spine and the posterior portion of the shoulder joint capsule.
The infraspinatus is involved in rotator cuff rips about as frequently as the supraspinatus because of its trapezoidal insertion onto the humerus, which is significantly greater than the analogous insertion of the supraspinatus.
The supraspinatus, infraspinatus, teres minor, and subscapularis comprise the infraspinatus, a part of the rotator cuff muscles. The glenohumeral joint is stabilized by these muscles.
These muscles have diverse, viscoelastic, nonlinear tendons. Collagen plays a significant role in these tendons by forming a matrix that allows for extensibility.
Four zones can be distinguished at the transition point from tendon to bone insertion: tendon mid-substance, fibrocartilage, calcified fibrocartilage, and bone.
Ligaments and connective tissues additionally stabilize the glenohumeral joint in addition to the rotator cuff muscles.
The dorsal portion of the scapula inferior to the scapular spine and the medial three-quarters of the infraspinous fossa are the origins of the infraspinatus.
On the rear scapula is the infraspinous fossa. The supraspinous and infraspinous fossae are formed by the division of the posterior portion of the scapula by the scapular spine.
Interestingly, the infraspinatus fossa is also the source of the teres minor muscle. The distal tendinous portion inserts on the middle facet of the larger tuberosity of the humerus after running along the lateral border of the scapular spine and over the posterior aspect of the shoulder joint.
The attachments of the supraspinatus and teres minor, located superiorly and inferiorly, respectively, enclose this attachment.
The muscle is covered by the infraspinous fascia, which also serves to differentiate it from the teres minor and major.
Function of the Infraspinatus Muscle
The primary mechanism by which the infraspinatus muscle acts on the shoulder is as a rotator cuff muscle that provides glenohumeral stability.
To stabilize the humeral head during shoulder abduction, the rotator cuff delivers compression to the head of the humerus.
The rotator cuff muscles produce opposing forces to maintain the balance of the shoulder’s movement. Because the subscapular produces the anterior force and the infraspinatus gives the posterior force, the infraspinatus is engaged in the anterior-posterior force balance.
The humeral head will partially elevate out of the glenoid fossa when the rotator cuff muscles are weak (due to a damaged infraspinatus tendon, for example), which will reduce the effectiveness of the deltoid muscles’ abduction motion.
The humerus’ head is the site of the infraspinatus’ activities. It can rotate externally or laterally thanks to the infraspinatus insertion at the glenoid tubercle’s middle facet.
Because it inserts on the inferior aspect of the glenoid tubercle, this force works in concert with the teres minor. Among the rotator cuff muscles, the infraspinatus has the second-largest anatomic imprint on the humerus. The subscapularis contains the largest.
The scapula is also affected by the infraspinatus. The infraspinatus permits the abduction of the scapula’s inferior angle, or scaption when the shoulder is kept in its anatomical position. Scaption increases scapular mobility, facilitating complete shoulder abduction with the help of other shoulder muscles.
Origin
The scapular infraspinatus fossa, which covers the muscle and divides it from the Teres Major and Teres Minor, is home to certain fibers that originate from the infraspinatous fascia.
Insertion
The shoulder joint capsule and the posterior side of the larger tuberosity of the humerus
Nerve Supply
C5 and C6 suprascapular nerves. It starts at the brachial plexus’ superior trunk.
It supplies both the supraspinatus and the infraspinatus by extending laterally across the lateral cervical area.
Blood Supply
The suprascapular and circumflex scapular arteries supply blood to the infraspinatus.
The subclavian artery or the thyrocervical trunk are the two sources of the suprascapular artery.
The artery crosses the clavicle posterolaterally and parallelly and proceeds inferolateral to the anterior scalene muscles, phrenic nerve, subclavian artery, and brachial plexus.
Next, it moves to the supraspinous fossa, passing over the transverse scapular ligament. To nourish the infraspinatus, it finally travels laterally to the scapular spine, passing deep into the acromion, and ending at the infraspinous fossa on the posterior surface of the scapula.
The circumflex scapular artery originates from the subscapular artery, which is a branch of the axillary artery’s third segment.
As it enters the infraspinous fossa, the circumflex scapular artery circles the lateral margin of the scapula and anastomoses with the suprascapular artery to supply collateral circulation.
Lymphatics
The subscapular (posterior) nodes are mainly responsible for lymphatic drainage. Six or seven lymph nodes that are located along the posterior axillary fold make up the subscapular nodes. The subscapular blood arteries are traversed by these lymph nodes.
The central axillary nodes are the conduit for the efferent drainage of the subscapular, pectoral, and humeral nodes.
The three or four nodes that make up the central axillary nodes are situated close to the second half of the axilla, deep to the pectoralis minor.
The apical nodes, which are located at the apex of the axilla close to the medial side of the axillary vein and the first segment of the axillary artery, receive efferent drainage from these central nodes.
The apical nodes, which are located at the apex of the axilla close to the medial side of the axillary vein and the first segment of the axillary artery, receive efferent drainage from these central nodes.
The cervicoaxillary canal is crossed by efferent vessels that emerge from the apical group. The subclavian lymphatic trunk is formed by the union of these efferent veins.
The subclavian lymphatic trunk can enter the right venous angle directly or join the jugular and bronchomediastinal trunk to produce the right lymphatic duct.
Variation
It is common to fuse the teres minor with the infraspinatus.
Related Muscles
Since the subscapularis, supraspinatus, and teres minor all connect to ring the glenohumeral joint at the shoulder, the infraspinatus is most closely related to these muscles.
These muscles move and stabilize the glenohumeral joint. As the shoulder’s external rotators, the infraspinatus and teres minor work together harmoniously.
Action
The primary shoulder joint external rotator.
It facilitates the development of shoulder extension.
It abducts the scapula’s inferior angle when the arm is stationary.
Anatomical Variantions
The literature currently in the publication does not contain many variations of the infraspinatus muscle, yet in a few cases, the muscle has been identified as united with the teres minor.
At the humeral head’s supraspinatus and infraspinatus insertions, subchondral cysts can be discovered. These may be mistaken for degenerative changes or rotator cuff disease.
Usually asymptomatic, the cysts on the dorsal insertion sites are discovered. In cases when cystic alterations are found on the anterior part of the humerus, evaluation of a possible subscapularis lesion is necessary.
Diagnostics
Infraspinatus muscle contracture is often diagnosed through orthopedic and physical tests. To be sure there haven’t been any changes to the underlying bones or joints, your primary care veterinarian could advise x-rays.
To precisely evaluate the muscle or tendinous insertion, more sophisticated diagnostics like musculoskeletal ultrasonography or magnetic resonance imaging (MRI) might also be suggested.
Trigger Point
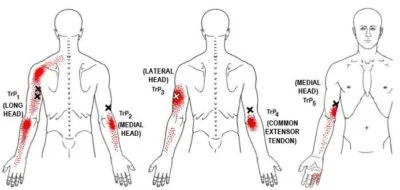
There are three typical sites for infraspinatus trigger points. Near the scapular spine are two. These refer to discomfort to the outside point of the shoulder, the ring, and little finger, the base of the head, and the entire arm.
Near the bottom, on the inside border of the scapula, is the third common trigger point. This point refers to discomfort that is sometimes misdiagnosed as supraspinatus, teres major, or rhomboid pain. It is felt along the scapula’s edge.
Surgical Considerations
The infraspinatus muscle, which is a component of the glenohumeral joint, is prone to rotator cuff injuries, which are typically brought on by anterior dislocations.
A Hill-Sachs lesion is frequently seen in cases of anterior shoulder dislocation. The humeral head’s translation back into the glenoid cavity is what caused the lesion on the posterior head of the humerus. The infraspinatus is used to fill in the defect in the healing of these kinds of injuries.
Conservative or surgical methods can be used to treat a rotator cuff repair. When symptoms are severe weakness or loss of function, the tear is larger than 3 cm, the injury is recent and acute, or the symptoms have persisted for 6 to 12 months, surgery is usually advised.
If surgery is chosen as a course of treatment, several methods such as open repair, arthroscopic repair, and mini-open repair can be employed.
For shoulder arthroscopy, surgeons utilize the plane between the teres minor and infraspinatus as the posterior approach. Osteotomy and glenoid fracture repairs are also performed using this posterior technique.
Before an arthroscopic rotator cuff surgery, it is customary to start by identifying important landmarks such as the location of the portal and the acromion, clavicle, and coracoid process. The lateral acromion is situated distal and medial to the posterior portal.
The coracoid process and the acromioclavicular joint are separated by the anterior portal. The clavicle and the lateral portal are lined up.
The surgeon will examine the architecture of the shoulder, including the four rotator cuff muscles, throughout the procedure.
The surgeon may choose to do an acromioplasty or subacromial bursectomy during the procedure. Debridement will be done and the footprint prepped for anchor insertion before the tendon is repaired.
Clinical Importance
In the United States alone, rotator cuff-related diseases result in 40,000 surgical procedures and 4.5 million visits each year. It is estimated that 16 to 34% of the population suffers from rotator cuff disease, with the frequency rising with age.
Both acute and chronic injury patterns, such as trauma, repetitive motion, impingement, and degeneration, can result in rotator cuff pain. The preferred imaging method for examining rotator cuff disorders is magnetic resonance imaging (MRI). The best way to show off this muscle group is via a weighted T1 sagittal oblique section.
Compression of the suprascapular nerve near the scapular notch is typically present in conjunction with evidence of atrophy of the supraspinatus and infraspinatus muscles on physical examination.
Athletes who fling themselves overhead, like baseball or swimming players, may have compression due to rips in the superior labrum anterior and posterior (SLAP). Infraspinatus muscle atrophy or isolated weakness is typically accompanied by a compression of the spinoglenoid notch nerve.
Usually, ganglion cysts cause the compression of the nerve at the spinoglenoid notch. Chronic rotator cuff tears or tendinous ruptures larger than five cm may also be the cause of muscular atrophy.
Treatment
The good news about this impairment is that other muscles support and cause the shoulder joint to flex, not only the injured one. We advocate a surgical correction, taking advantage of the fact that dogs can function effectively without it.
Simply put, the infraspinatus muscle’s tendon is severed close to the point where it joins the humerus. To achieve the entire range of motion of the shoulder, more surrounding tissues are also freed.
This relieves the scarred muscle’s tension; occasionally, the release is rather dramatic, causing the joint to suddenly “pop” as it becomes free of constraint. The shoulder joint regains a complete range of motion right away after this simple surgical procedure.
The patients appear pain-free and fully functional with no enforced limits following the healing of the minor surgical site.
Exercise of Infraspinatus Muscle
Infraspinatus Muscle Stretching Exercise
Pendulum Stretches

- Exercisers who wish to complete a pendulum stretch should bend at the hips and back, with one arm supporting their torso on a table.
- The exerciser will then draw their arm backward before allowing it to swing forward, repeating this pendulum-like action with no input from the legs or other muscles other than the shoulders.
- They should leave the free arm hanging beneath their torso.
- After sufficiently warming up the shoulder structure, the exerciser will perform the same movement with the other arm.
External rotation stretch
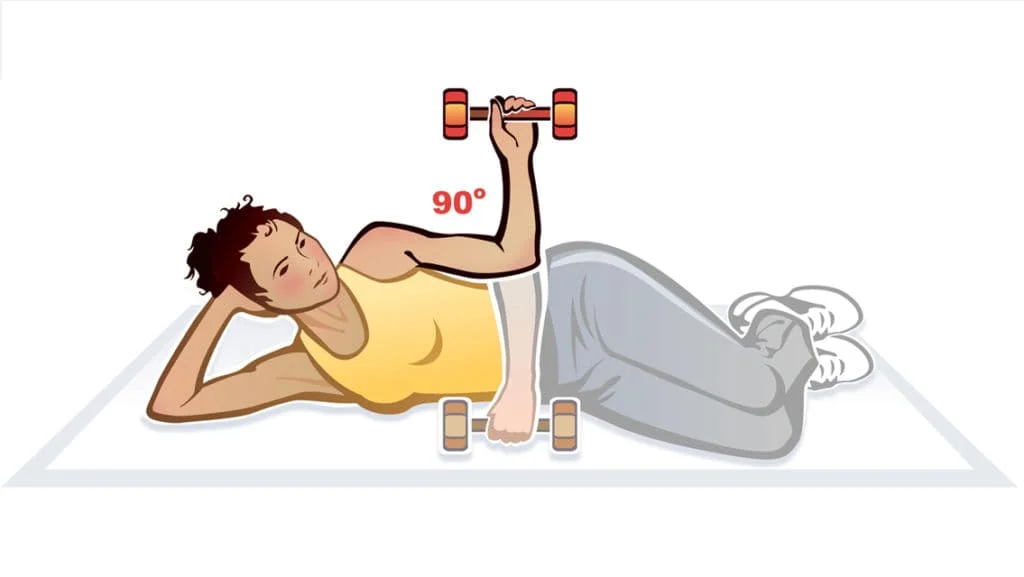
- Head resting on the left arm while lying on the left side.
- Your right elbow should be in the air, your hand should be on the ground, and your right arm should be running across your belly while you flex the arm that is not lying at a 90-degree angle.
- Rotate your arm slowly while moving your right elbow by your side.
- Turn until your hand is in the air and the rotation is 90 degrees bent.
- Rotate the right arm back down slowly.
- Execute two sets of ten.
- On the left side, repeat.
Broom-Stick-Assisted Stretch
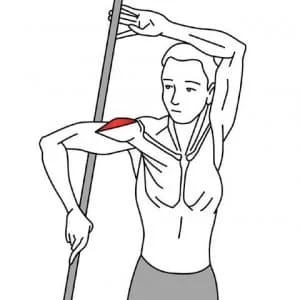
- A prop is necessary, like a broom. Keep your back to the wall.
- Taking a stick in your left hand, raise it above your head in the manner of a flag.
- Allow the stick to point downward toward the floor behind you to the right by bending your left arm at the elbow.
- Reach back and grab the other end of the stick with your right hand.
- Raise your right elbow to shoulder level.
- Rotate your shoulder inside out by pressing the stick against your right shoulder with your left hand.
- For 30 seconds, hold the stretch.
- On the other side, repeat.
Cross-Arm Stretch

- The infraspinatus is drawn horizontally and somewhat upwards by the cross-arm stretch.
- This may be done anywhere, whether you’re sitting, standing, or lying down.
- Reach over your left arm to your chest.
- Now take your right hand and hold your left elbow.
- Push your left arm gently in your direction.
- Hold it for 20 to 30 seconds, then let go.
- Carry it out from the right side.
- Do this two or three times.
Seated Bent-Over Stretch
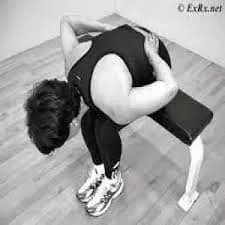
- Settle down on the chair’s edge.
- Currently, position your hands behind your lower back.
- You ought to be pointing your elbow outward.
- Exhale slowly while bending forward as much as you can.
- Take a few seconds to hold the stretch.
- Do this two or three times.
Infraspinatus Muscle Strengthening Exercise
Y-Raises

- The exerciser will stand straight, with arms at their sides, and feet in a balanced yet prepared stance to complete Y-raises.
- The exerciser will then raise their arms upward while maintaining a neutral bend at the elbows and wrists while grasping the source of resistance with both hands (or just clenching the hands into fists).
- The exercise gets its name because the torso forms the letter “Y” at the top of the repetition.
- The exerciser will then gradually bring their hands back to the beginning position to finish the repetition after reaching this point.
Reverse Dumbbell Flyes

- The exerciser will grasp a pair of lightweight dumbbells in both hands and bend at the hips and knees to perform reverse dumbbell flies.
- The ideal angle of resistance is achieved by maintaining the torso nearly parallel to the floor.
- The exerciser may also use a bench if they are having problems staying in this position for the duration of the exercise.
- The exerciser will first let the arms hang below the torso in front of them.
- Then, they will contract their deltoids and scapula, pulling the dumbbells up and outwards as though using their upper body to make the letter “T.”
- The exerciser will let the dumbbells drop back to their starting position beneath the chest after elevating them as high as they are capable of going to complete the repetition.
Dumbbell Standing External Rotation
- The exerciser will grasp a pair of lightweight dumbbells in both hands and bend at the hips and knees to perform reverse dumbbell flies.
- The ideal angle of resistance is achieved by maintaining the torso nearly parallel to the floor.
- The exerciser may also use a bench if they are having problems staying in this position for the duration of the exercise.
- The exerciser will first let the arms hang below the torso in front of them.
- Then, they will contract their deltoids and scapula, pulling the dumbbells up and outwards as though using their upper body to make the letter “T.”
- The exerciser will let the dumbbells drop back to their starting position beneath the chest after elevating them as high as they are capable of going to complete the repetition.
Summary
We looked into how four external rotation exercises affected the activation of the posterior deltoid, middle trapezius, and infraspinatus muscles. SWE was found to produce more infraspinatus muscle activity than the other exercises.
Compared to the PER and STER, the SWE produced less activity in the posterior deltoid muscle and less activity in the middle trapezius muscle.
Our findings imply that the SWE is a new and useful exercise because it minimizes the involvement of the middle trapezius and posterior deltoid muscles while specifically activating the infraspinatus muscle.
Clinicians may find these data useful in creating efficient workout regimens.
FAQ
What is the main action of infraspinatus?
Despite being one of the most dynamic joints in the body, the shoulder joint is made stable by these muscles. The primary muscles involved in scapulation, lateral humeral rotation, and external shoulder rotation are the infraspinatus.
What is the daily use of infraspinatus?
During arm movements, the infraspinatus muscle helps to stabilize the humerus head and aids in the external rotation of the arm. TrPs in the infraspinatus muscle may be one of the most overlooked reasons for shoulder and/or arm pain, according to Simons et al. (1999).
Is the infraspinatus muscle weak?
Compression of the suprascapular nerve in the spinoglenoid notch can cause isolated weakness or atrophy in the infraspinatus muscle; however, ganglion cysts are typically the cause of compression of the nerve in the spinoglenoid notch.
How do you test infraspinatus strength?
The patient asks to rotate both forearms externally, but the examiner declines. When there is discomfort or weakness during external rotation, the test is considered positive. Since infraspinatus tears typically don’t hurt, external rotation weakness is a significant indicator of one.
How do you relax infraspinatus?
Maintain a straight and tall posture.
Lower your shoulder blades and relax.
Fold your arms across in front of you.
Take hold of the elbow of the extended arm and gently drag it across your body.
Gently press the forearm of the side you are stretching with your opposing (upper) arm.
The sensation is the pull on your shoulder blade.
Is the infraspinatus a push or pull?
The infraspinatus is more useful as an external rotator at lower shoulder abduction angles because of its line of pull, which keeps the arm closer to the side of the body. The amount of external rotation force is reduced when the abduction angle increases because the infraspinatus moment arm is shortened.
What is the gym’s use of infraspinatus?
You may strengthen your rotator cuff muscles and lower your risk of injury by including infraspinatus workouts in your training regimen. Targeting the infraspinatus muscle throughout your workouts is vital since it plays a critical role in shoulder stability and mobility.
What are the facts about infraspinatus?
The main portion of the infraspinatus fossa is occupied by the thick, triangular infraspinatus muscle in human anatomy. The infraspinatus, one of the four rotator cuff muscles, is primarily responsible for stabilizing the shoulder joint and externally rotating the humerus.
What causes infraspinatus tightness?
It aids in the rotation of your arm to the side and connects the top of your humerus, the upper bone in your arm, to your shoulder. The most common cause of pain in the infraspinatus is probably shoulder repetitive motion. It is more common in swimmers, tennis players, painters, and carpenters.
How do you heal infraspinatus muscle?
Give up on sports or other pursuits for a while. Put it in the freezer: For fifteen to twenty minutes, place some ice in a towel and place it over your shoulder. Exercises for stretching: You can start doing some light stretches and exercises to strengthen your muscles and rotator cuff if your symptoms become better.


2 Comments