Elbow Examination
What is an Elbow Examination?
The elbow examination is a systematic assessment used to evaluate the function, stability, and integrity of the elbow joint. It involves observation, palpation, range of motion testing, and specific maneuvers to assess the bones, ligaments, muscles, and neurovascular structures.
Key components include observing for deformities, swelling, or erythema, assessing active and passive movements (flexion, extension, pronation, supination), and performing special tests for conditions like lateral epicondylitis (e.g., Cozen’s test) and ligamentous stability.
A thorough elbow examination aids in diagnosing common conditions such as fractures, tendinopathies, arthritis, and nerve compressions.
Anatomy:
The elbow joint is a synovial joint situated between the forearm and the arm in the upper limb. The humerus of the arm, the radius, and the ulna of the forearm are the three bones that articulate there.
From the structural viewpoint, the elbow joint is categorized as a synovial joint. Because the joint has two articulations, it is also categorized structurally as a compound joint. Diarthrosis, another name for synovial joints, is a freely mobile joint. At these joints, a layer of hyaline cartilage separates the articular surfaces of the bones from one another. These joints are lubricated by a very viscous synovial fluid, which facilitates smooth movement.
The joint is enclosed by a fibrous capsule that has a synovial membrane lining the inside. Based on their function, synovial joints can be further classified. Since the elbow joint may only move in one plane (uniaxially), it functions as a hinge joint.
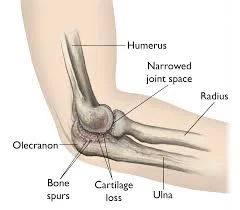
Elbow joint bones:
Your elbow joint is composed of three bones:
- The humerus is the upper arm bone.
- The longer bone in your forearm is called the ulna.
- The shorter forearm bone is called the radius.
Elbow joint cartilage:
Your joints are protected by cartilage, a strong, elastic substance. Hyaline cartilage lines the inside of your elbows.
The hyaline cartilage in your joints is smooth and slippery, making it easier for bones to move through each other. The surfaces of your humerus, ulna, and radius that come into contact with each other are lined with hyaline cartilage.
Ligaments of the elbow joint:
Bones are joined by ligaments, which look like cords.
Your elbows have three major ligaments.
- The ligament that joins your ulna to the inside edge of your humerus is called the medial collateral ligament.
- The ligament that joins your ulna to the outside edge of your humerus is called the lateral collateral ligament.
- Annular ligament: A ligament that attaches your ulna and humerus to the head (top) of your radius.
Elbow muscles:
Flexing your lower arm inside toward your body is made possible by muscles that regulate flexion. Among them are the
- Biceps Brachii
- Brachialis
- Brachioradialis
Your lower arm can be moved out and away from your body by using two extensor muscles:
- Triceps
- Anconeus
Supination-controlling muscles allow you to raise your palm:
- Supinator
You can move your palm down with the help of your biceps and flexor muscles:
- Pronator Teres
- Pronator quadratus
- Brachioradialis
Elbow nerves:
- Radial nerve.
- Ulnar nerve.
- Median nerve.
- Musculocutaneous nerve.
Elbow blood vessels:
The pathways that transport blood throughout your body are called blood vessels. Like a circuit, they create a closed loop that starts and finishes at your heart. Blood travels via three arteries to and from your elbow, including the
- Radial artery
- Ulnar artery
- Brachial artery
Commonly occurring problems or conditions that affect the elbows:
- Arthritis.
- Elbow bursitis.
- Nursemaid’s elbow.
- Tendinitis.
Sports-related elbow injuries are among the most common:
- Sprains.
- Lateral epicondylitis (tennis elbow).
- Medial epicondylitis, or golfer’s elbow.
- Elbow Dislocations
- Elbow fractures (broken elbows).
Typical signs of an elbow injury:
- Pain in the elbow, particularly when bending or flexing the arm.
- Swelling/Inflammation.
- Rigidity.
- Instability
- Bruising, Redness, or Discoloration.
- A sensation of heat or warmth.
Examination:
History:
The specific location where the pain is
Timeline: When do the patient’s symptoms feel to be the worst?
The injury’s mechanism: A mechanism of injury helps direct a diagnosis in the event of a traumatic incident. Certain symptoms may be very helpful in making the diagnosis of severe injuries. For example, ulnar neuropathy may be indicated if the patient feels tingling or numbness in the fifth digit.
- Appearance of tingling or numbness.
- Drugs
- Previous Medical History
- radiography, and diagnostic testing.
Warning Signs:
- Inflammation and Infection
- Cancer
- Dislocation or Fracture (Positive Elbow Extension Test)
- Rheumatoid arthritis
- Abnormal Vitals
- Unusual Neurological/Vascular Examination
- Heterotopic Ossification (Think About After Surgery)
- Inappropriate post-operative treatment progress.
Red Flags:
- Psychosocial components
- Passively coping
- Avoiding Fear Beliefs
Observation:
An upper quarter’s general posture: There are proximal factors that may put a patient at risk for elbow pain.
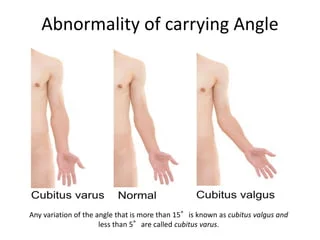
Carrying angle of elbow: The angle between the forearm and the upper arm when the arm is extended and the palm faces forward. It’s normally between 5 degrees and 15 degrees.
Triangle Signs, deformities, swelling, ecchymosis, and muscle atrophy.
Palpation:
- Lateral/medial epicondyle
- Olecranon fossa
- The radial head of the elbow
- Ulnar Collateral Ligament (UCL)
Functional Tests:
The asterisk sign’s identification: (What activity raises symptoms?)
Painless Grip Power
Push-off Test: The ability to support weight via the upper extremities can be measured with a push-off test. Finding functional or occupational constraints could be helpful.
A standardized physical examination is the Functional Impairment Test, Neck, and Shoulder Arm (FIT-HaNSA). Evaluates the gross movements of the upper limbs. Elbow joint conditions have not been fully validated.
Neurologic Assessment:
- C5-T1 Myotomes
- C5-T1 Dermatomes
- C5–C7 Reflexes
Movement Testing:
With or without overpressure, active range of motion (AROM) and passive range of motion (PROM)
- Elbow
- Flexion
- Extension
- Forearm pronation/supination
- The extension and flexion of the wrist
Testing for Resistance
- Bending and extending the elbow
- Pronation and supination of the forearms
- Bending and extending the wrists
- Strength of grasp without pain
- Fingers and Thumbs
Accessory motion testing
- Humeroulnar traction
- Humeroradial traction
- Distal/proximal radioulnar Glides from anterior to posterior and posterior to anterior
Special test:
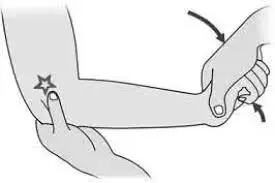
Elbow Flexion Test:

One neurological dysfunction test used to diagnose cubital tunnel syndrome (ulnar nerve) is the elbow flexion test.
Method
- Previous to doing anything further, the patient should be standing or even sitting.
- Next, ask the patient to perform 90-degree shoulder girdle abduction and depression, as well as actively fully bend their elbows while extending their wrist.
- After that, maintain the posture for a maximum of two to three minutes.
- A favorable indicator, therefore, suggests that the ulnar nerve root is distributed with numbness or tingling.
Tinel’s sign at elbow:

The general term for a test when the therapist uses a percussion or even tapping technique to identify the inflamed nerve is Tinel’s Sign. Tinel’s sign at an elbow denotes an inflamed Ulnar nerve.
Method
- The physical therapist locates the Ulnar nerve, which is situated in the gap between the medial epicondyle and the olecranon process. The physical therapist then repeatedly taps the Ulnar nerve with the index finger. The tingling sensation in an ulnar distribution of the hand and forearm distal to a tipping point indicates a positive sign.
Ulnar Nerve Compression Test:
A physician asks about symptoms, obtains medical history, and performs a thorough examination of the hand, elbow, and arm to determine whether a patient has ulnar nerve compression. Additionally, a physician might assess the arm for sensation and strength, as well as for indications of nerve injury or inflammation.
Approach
Initially, each test is primarily conducted on an asymptomatic or normal side. The elbow joint is typically positioned in the following order for an upper limb: shoulder, forearm, wrist, fingers, and elbow. Until the pain is triggered or the symptoms are replicated, each similar joint location component is added. The cervical spine’s side flexion may be included to increase the sensitivity of upper limb examinations. There is no need to apply more sensitizers if the pain is triggered at the initial position.
Mill’s Test :

The test mentioned aids in the diagnosis of “Tennis Elbow,” or Lateral Epicondylitis in the elbow.
Clinical signs
- The patients complain of pain radiating down their forearm from their lateral elbow. Additionally, patients frequently report having trouble lifting objects and having a weak grasp. Patients usually exhibit point discomfort both medially and distally to a lateral epicondyle upon physical examination.
Method
- The patient is seated, and the clinician uses one hand to palpate the patient’s lateral epicondyle while the patient’s forearm is pronated, their wrist is fully flexed, and their elbow is extended. A positive test result is produced in a region of insertion at a lateral epicondyle.
Cozen’s Test:
Goal
Cozen’s test, often known as the “resisted wrist extension test” or even the “resistive tennis elbow test,” is used to show for “tennis elbow” or Lateral Epicondylitis.
The position of the patient
A patient may be sitting with their wrist radially abducted, their elbow extended, their forearm maximally pronated, and their hand in a fist.
A Role as an Examiner
With the opposite hand resting on the dorsum of a hand, a physical therapist may support an elbow while feeling the lateral epicondyle.
Method
- In the above-described position, a patient is urged to move their wrist to dorsal flexion while a physical therapist applies resistance to the action. If pain is felt on a lateral epicondyle, the test is considered positive.
Maudsley test:

Physical therapist mostly use Maudsley’s test to confirm a diagnosis of Lateral Epicondylitis, also known as “Tennis Elbow.”
Method
- When palpating a patient’s lateral epicondyle, the examiner resists extending the third digit of the hand, putting stress on the extensor digitorum muscle and tendon. A positive test result over the lateral epicondyle of the humerus is indicated by pain.
Elbow Varus Stress Test:
The primary goal of the elbow’s varus stress test is to assess the lateral collateral ligament’s integrity.
Method
- While the patient is upright, a physical therapist palpates the humeroulnar joint line by slightly flexing the patient’s elbow. The varus force is then applied to an elbow by a physical therapist. If a patient has pain or excessive laxity, as well as when compared to the contralateral side, the test mentioned above is considered positive.
Elbow Valgus Stress Test:
The primary purpose of an elbow valgus stress test is to evaluate the strength of the medial collateral ligament, commonly known as the ulnar collateral ligament.
Method
- The test can be administered to the patient standing, sitting, or in a supine posture. To palpate a medial joint line, stabilize a distal humerus with one hand and apply valgus stress to an elbow with another. A physical therapist positions the patient’s elbow in about 20 degrees of flexion. If a patient has pain or increased laxity relative to the contralateral side, the test is deemed positive. Similar to a varus stress test, the test can be repeated with the elbow extended to assess different medial collateral ligament (MCL) segments.
Chair push-up test:
The chair push-up test, sometimes known as the stand-up test or simply the chair sign, is used to assess the lateral collateral ligament and check for posterolateral rotatory instability (PLRI) of the elbow joint.
Method
- The patient is sitting in a chair with both hands resting on the arms of the chair or the sides of the seat. To get into the standing posture, a patient actively pushes up. Posterolateral rotatory instability (PLRI) and lateral collateral ligament insufficiency are indicated by pain, fear, clicking, or even locking during a transition.
Moving Valgus Stress Test:
One of the functions of a moving valgus stress test is to assess the strength of the elbow’s ulnar or medial collateral ligaments.
Method
- The patient may sit or maybe stand during the test mentioned. A patient’s shoulder is abducted to 90 degrees by a physical therapist. A physical therapist uses one hand to brace an elbow and the other to hold a distal forearm. After that, an examiner externally rotates a shoulder while maximally flexing the elbow and applying valgus stress on it. An examiner swiftly and smoothly extends an elbow to around 30 degrees once the shoulder reaches its end range of external rotation.
- A patient must 1) feel discomfort at the medial elbow and 2) have a maximum level of pain between 120 and 70 degrees of elbow flexion for the moving valgus stress test to be considered positive.
Neurodynamic Tests:
The Upper Limb Tension Test 1 (ULTT1) measures median nerve compression.
Signs:
- Radiating pain in the upper limb
- Sensations of tingling in the thumb, index finger, and middle finger
Actions taken:
- Shoulder depression
- Shoulder abduction110-degree 90-degree
- Elbow flexion 90-degree
- Shoulder external rotation
- Supination of the forearm
- Finger and wrist extension
- Elbow extension.
Differentiation in structure:
- Minimal symptoms: reduced wrist pain and finger extension
- Distal symptoms (provocation): Neck flexion in the opposite direction.
Upper Limb Tension 2A Test (ULTT2A), which measures median nerve compression:
Signs of this examination:
- Radiating pain in upper limb
- Instability, recent shoulder dislocation, and recent shoulder arthroplasty surgery.
The following movements were performed:
- Shoulder girdle depression, external rotation with the elbow at 90 degrees, and shoulder abduction at 100 degrees
- Supination of the forearm,
- Extension of the wrist, fingers, and elbows.
Differentiation in structure:
- Nearby symptoms: relieve the wrist and extend the fingers.
- Neck flexion in the opposite direction is one example of provocation, often known as distal symptoms.
Assessment of radial nerve entrapment using the Upper Limb Tension Test 2B (ULTT2B):
Signs:
- Upper limb radiating pain
- Cervical Radiculopathy
- De Quervain’s tenosynovitis
- Supinator tunnel syndrome
The following movements were made:
- Forearm pronation
- Shoulder girdle depression
- Shoulder abduction 20–30 degrees
- Shoulder internal rotation.
- Flexion of the wrist, fingers, and thumb
- Extension of the elbow.
Differentiation in structure:
- Reduce the bending of the fingers and wrists as proximal symptoms
- Distal symptoms, often known as provocation, include the contralateral flexion of the neck
Ulnar nerve compression in the third upper limb tension test (ULTT3):
Signs :
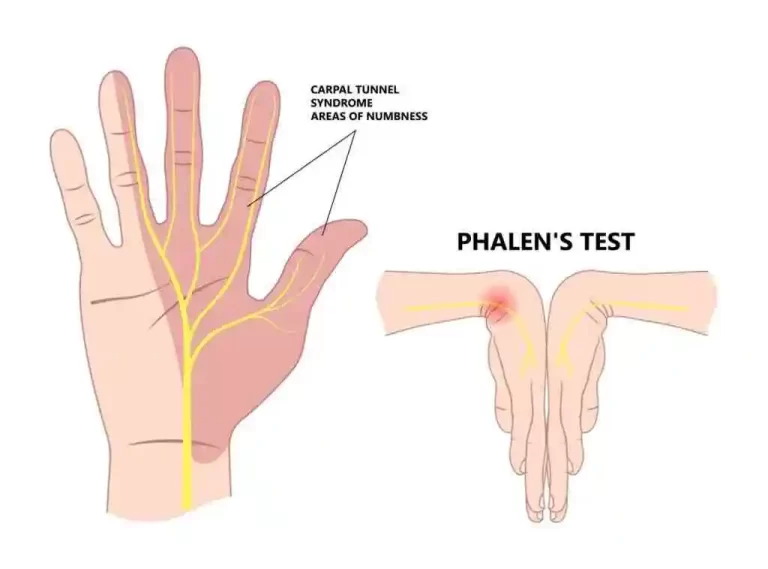
- Carpal tunnel syndrome
- Thoracic outlet syndrome
- Pain radiates to the fourth and fifth fingers.
The following movements were performed:
- forearm pronation
- Wrist and finger extension
- Elbow flexion
- Shoulder girdle depression
- Shoulder abduction 110 degrees
- Shoulder external rotation
Differentiation in Structure:
- Reduce the proximal symptoms of wrist and finger extension.
- One of the distal symptoms (provocation) is the opposite direction of neck flexion.
FAQs
Which three elbow joints are there?
Three joints make up the elbow:
Movement between the ulna and humerus is made possible by the ulnohumeral joint.
Movement between the radius and humerus is made possible via the radiohumeral joint.
Movement between the radius and ulna is made possible via the proximal radioulnar joint.
What is the term for elbow joint pain?
Regarding elbow discomfort
Tennis elbow is the most prevalent form of elbow pain. Another less frequent but comparable overuse injury is golfer’s elbow.
Which four elbow movements are there?
The radius and humerus create the humeroradial joint, which permits flexion, extension, supination, and pronation.
How is the elbow examined?
During a physical examination, the biceps muscular belly should move normally like a piston when the elbow is flexed to 90 degrees and the forearm is passively supinated and pronated. A complete tear is indicated by the absence of this motion. Pain deep in the antecubital fossa is usually recreated by resisting supination.
What is the elbow’s unique test?
Mill’s sign, Maudsley’s sign, the elbow plica impingement test, the pressure provocation test, Cozen’s test, and the golfer’s elbow test are some of the unique tests for the elbow.
Reference:
- Professional, C. C. M. (2024, August 6). Elbow joint. Cleveland Clinic. https://my.clevelandclinic.org/health/body/elbow-joint
- TeachMeAnatomy. (2023, November 2). The elbow Joint – Structure – Movement – TeachMeAnatomy. https://teachmeanatomy.info/upper-limb/joints/elbow-joint/
- Elbow joint. (2023, September 11). Kenhub. https://www.kenhub.com/en/library/anatomy/elbow-joint
- Savoie, F. H. “., III MD. (n.d.). Elbow Anatomy & Biomechanics – Shoulder & Elbow – Orthobullets. https://www.orthobullets.com/shoulder-and-elbow/3078/elbow-anatomy-and-biomechanics
- Orthopedics, B. S. M. V. (n.d.). Elbow Physical exam – Shoulder & elbow – orthobullets. https://www.orthobullets.com/shoulder-and-elbow/322131/elbow-physical-exam
- Examination of the elbow joint – TeachMeSurgery. (2023, June 23). TeachMeSurgery. https://teachmesurgery.com/examinations/orthopaedic/examination-of-the-elbow-joint/