Scapular Dyskinesia
Introduction
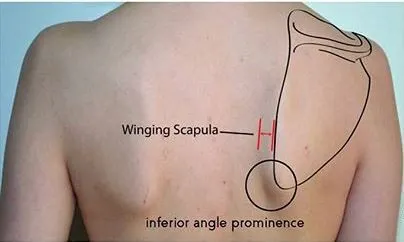
Scapular dyskinesis refers to an alteration in the normal movement or position of the shoulder blade (scapula) during shoulder motion. It can manifest as a variety of presentations, including scapular winging, where the medial border of the scapula protrudes from the rib cage, or as dysrhythmia, where the scapula moves prematurely or excessively during arm elevation.
Additionally, the shoulder blade, or scapula, provides a firm foundation for the activation and operation of the rotator cuff. Any injury to the soft tissues or bones surrounding the shoulder might change how the scapula functions both at rest and when moving.
In addition to healthy individuals, SD can be seen in overhead athletes and patients with shoulder pathologies such as rotator cuff dysfunction, glenohumeral instability, impingement syndrome, and labral tears. Reduced scapular external rotation, upward rotation, and posterior scapular tilting are symptoms of subacromial impingement syndrome.
It is uncertain and needs more research if shoulder pain causes SD or vice versa, although patients with shoulder pain have a greater frequency of SD. Despite the lack of symptoms at the moment, some study indicates that SD may be able to predict future shoulder pain.
Six factors may contribute to scapular dyskinesis:
- Damage to your nerves
- Loss of flexibility
- Damage to your muscles
- Weakness in your core, hips, or legs
- Weak bones or bone fractures
- Damage to your joints
Your scapula rotates in the following manner:
- External rotation
- Posterior tilt
- Upward rotation
- Medial translation
Damage could hinder a piece in this movement phase. Because dislocation injuries account for over 90% of unidirectional instances, participating in sports raises your risk of developing the illness. Scapular dyskinesis is most likely to occur in the following sports:
- Gymnastics
- Swimming
- Volleyball
- Baseball, primarily pitchers
The majority of men with scapular dyskinesis are between the ages of 18 and 25.
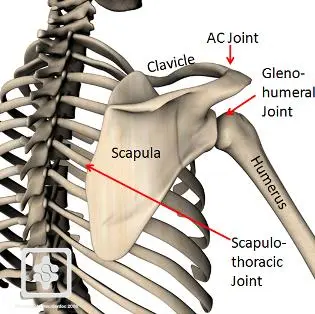
Scapular Biomechanics
The motions are:
- Upward/downward rotation
- Internal/ external rotation
- Anterior/posterior tilt
The translations are:
- Upward/downward sliding on the thorax.
- Slipping medially and laterally around the thoracic curvature.
Upward rotation and posterior tilt are the primary and secondary scapular movements during overhead upper extremity elevation, with internal/external rotation being minor until 100°.
According to an early study, the overall ratio of scapular upward rotation to glenohumeral elevation was 2:1. Another study discovered a regular sequence of clavicular elevation and retraction, posterior tilting, external rotation, and scapular upward rotation during the arm’s scapular plane elevation.
Increased scapular anterior tilt, increased scapular internal rotation, and altered scapular upward rotation are the altered mechanics in SD; these are covered in greater depth in the Classification section that follows.
Causes
Although there are numerous causes of SD, they can be divided into three categories:
- Muscle weakness or imbalance
- Poor overhead mechanics
- Overuse of the muscle
- Shoulder-related;
- Neck-related;
- Posture-related.
- Shoulder-related: Shoulder pathologies linked to SD include acromioclavicular instability, shoulder impingement, rotator cuff injuries, glenoid labrum injuries, clavicle fractures, stiffness of the posterior glenohumeral capsule, and inflexibility of the pectoralis minor and short head of the biceps. One theory regarding SD has been that it is caused by compensation through greater activation of the upper trapezius as a result of decreased activation and regulation of the lower, middle, or serratus anterior (SA).
- Neck-related: Cervical nerve root disorders and mechanical neck pain syndromes.
- Associated with posture: Athletes are more likely to exhibit excessive thoracic kyphosis and cervical lordosis, which are linked to SD.
Symptoms
Both symptomatic and asymptomatic SD patients are possible. Among the symptoms of SD are one or more of the following:
- Anterior shoulder pain
- Posterosuperior scapular pain (may radiate into the ipsilateral paraspinal Cervical region or radicular/thoracic outlet-type symptoms in the affected Upper extremity can be found)
- Superior shoulder pain
- Proximal lateral arm pain
- Shoulder impingement syndrome
- Rotator cuff dysfunction
- Shoulder instability
- Neck pain
- Pain or soreness around the scapula may occur when using the arm overhead or when carrying heavy objects at the side.
- Feeling like something is popping or snapping around the scapula when the shoulder moves
- Weakness when using the arms and shoulders.
- Asymmetrical posture (affected side usually sits lower)
- Winging of the scapula
- Shoulder instability (feels like it shifts out of place)
Classification of Dyskinesia Types
In general, shoulder asymmetry is reliable to note. During arm motions, one of the three forms of dyskinesia can be identified based on visual inspection to establish whether SD is present:
- Type 1: The anterior tilt of the scapula or the prominence of the inferior angle
- Type 2: The medial boundary (scapular winging) is prominent.
- Type 3: Early scapular elevation or excessive/insufficient upward rotation during arm elevation
Manually Assisted Movements of the Scapula
Two tests that apply manual assistance to the scapula—the Scapular Assistance Test (SAT) and the Scapular Reposition (Retraction) Test (SRT)—are used to assess the involvement of the scapula position in shoulder pain.
The patient is asked to perform arm flexion or abduction during the SAT and use a numerical pain rating scale to indicate how much pain they are experiencing. The examiner repeats the process, pulling on the scapula’s upper side to create posterior tilt and pressing laterally and upward on the inferior angle to encourage upward rotation.
The test is considered successful if, following supported mobility, two or more pain spots subside. This implies that the patient’s pain may be influenced by scapula dyskinesia. The same effect of enhancing scapula kinematics can then be replicated using taping techniques.
When performing SRT, the patient flexes and rotates their shoulder 90 degrees while the examiner uses one hand to support the medial scapular border. The examiner next asks the patient to maintain the position while using the other hand to apply resistance. The test is considered successful if the patient has less pain or gains more strength with the help. To determine the impact of scapular retraction stabilization on improving supraspinatus strength deficiencies in SD patients.
Diagnosis
Physical Examination
Observation.
Your doctor may ask you to raise and lower your arms three to five times, sometimes while holding small weights, to check for scapular dyskinesis. This will typically show the aberrant motor patterns and any muscle weakening.
- Corrective maneuvers. Corrective maneuvers are used in certain tests to assist your doctor in better understanding your situation. Among these tests are:
- Scapular assistance test (SAT). As you raise your arm during this exam, the physician will gently press on your scapula to help it rise. Your muscles may not be strong enough to raise your arm if your symptoms subside and your range of motion increases.
- Scapular retraction test (SRT). To assess your strength, the physician will apply pressure on your extended arm during this exam. Your strength will then be assessed once more once the scapula has been manually retracted. Patients with scapular dyskinesis will have stronger muscles when their shoulder blades are retracted.
Assessment of Surrounding Structures
It is possible to evaluate the scapula’s surrounding tissues for muscle power, soft tissue laxity, pain, and loss of function.
It is necessary to evaluate the instability of the acromioclavicular (AC) and sternoclavicular (SC) joints. Rotating the acromion in an AP position while maintaining clavicle stability allows one to measure the anterior-posterior, also known as laxity of the AC joint. Manual muscle examinations for the rotator cuff and biceps are possible. When used to evaluate infraspinatus weakness caused by SD, the infraspinatus strength test shows good reliability.
Muscle Tests
When the scapula posture is broken and scapular movement occurs, the doctor looks for three specific muscle tests and takes into account the scapular muscle weakness:
- For the serratus anterior, manual resistance of the arm at 130° of flexion
- Manual arm resistance for the lower and middle trapezius at 130–150° of abduction
- Sideways arm extension (for the rhomboid)
Core Evaluation
To find out if hip and core strength aid in scapular mobility, perform the low row test. Behind the patient is the examiner. The patient is instructed to resist moving their arm into flexion while performing a small amount of arm extension. Gluteal muscle contraction is used to repeat the same motion. Strengthening of the core and lower extremities might be included in the treatment plan if the strength increases with gluteal contraction.
Physical Therapy management
Medication, ice, stretching, strengthening exercises, and a change in the activity that created the issue are all part of the first treatment. To give the shoulder time to rest following the diagnosis, some time off may be required. Referrals to athletic trainers or physical therapists are frequently advised.
Nonsurgical Treatment
Medication
Non-steroidal anti-inflammatory medications, such as ibuprofen, are commonly recommended. As prescribed by your doctor, take these. If you experience any bleeding, upset stomach, or symptoms of an allergic reaction, call your doctor right away.
Heat and Cold
- Inflammation is decreased, and pain is relieved with cold. After an accident, a cold should be applied for 15 to 20 minutes every two to three hours to reduce pain and inflammation. Use ice packs or massage yourself.
- Before engaging in the stretching and strengthening exercises that your doctor, physical therapist, or athletic trainer has recommended, you may apply heat.
The goal of treating SD is to restore external rotation, posterior tilt, and scapular retraction.
The following are specific scapular rehabilitation exercises:
Exercises for increasing flexibility include shoulder horizontal abduction at 90 and 150 degrees of elevation, pectoralis minor flexibility, and external rotation and posterior tilt of the scapula.
Stretching and strengthening activities for stabilization that maximize scapular kinematics, enhance muscle strength, and increase joint position sense: Push-ups, lawnmower exercises, and resisted scapular retraction are examples of both closed and open kinetic chain workouts.
To stabilize the scapula, the serratus anterior and trapezius muscles are essential. They serve as a force-coupling mechanism during upper extremity movements and are particularly important in the aforementioned posture. They should be given careful consideration during therapy because they are the primary muscles that produce dyskinesia. When performing push-ups on an unstable surface, the activation of the trapezius increases, and the activation of the serratus anterior decreases.
Exercises for the shrug enhance the upward rotation angle and contract the upper and lower trapezius. Therefore, patients with SD and the associated scapular downward rotation condition can benefit from them. However, this exercise can postpone the restoration of scapular muscle balance, thus, it should not be performed during the first four to six weeks of rehabilitation.
Surgical Treatment
Surgery is not necessary for the majority of patients with general dyskinesis brought on by muscular weakness or tightness.
Your doctor might, however, carry out surgery to rebuild or repair the damaged tissues if your shoulder joint injury is the source of your dyskinesis. Rehabilitation will come next to get the scapula moving normally again.
Home remedies
Simple at-home therapies for scapular dyskinesis can sometimes alleviate its symptoms. These include:
- Restoring good posture. Make an effort to sit and stand correctly while you go about your daily tasks. Pull your shoulder blades back together and bend your elbows back and down as though you were putting them in your back pockets to accomplish this.
- Balancing your exercise routine. Make sure your upper body strength training sessions are balanced if you’re following a regular exercise regimen. Each set of “presses” you execute should be followed by one set of “flies” and two sets of “rows.” Additionally, your program should incorporate shoulder joint rotation and stretching exercises for your front shoulder muscles.
- Heat therapy. Soaking in a hot bath or applying a heating pad might help relax tense shoulder muscles. It’s critical to get in touch with your physician if your symptoms continue. They can offer therapy alternatives and assist in identifying the precise cause of your dyskinesis.
Risk Factor
- Sports involving overhead activity
- Increase in throwing velocity.
- Loose joints
- Previous or repeat shoulder injuries
- Poor physical conditioning (strength and flexibility)
- Kyphosis (excess curvature in the upper back)
Complications
- An extended recovery period may occur if not properly cared for or given enough time to recover.
- Rotator cuff impingement or chronic inflammation that results in ongoing pain with movement that could develop into chronic pain (with or without exercise)
- Shoulder stiffness or loss of motion
- Rotator cuff tendon tear(s)
- Symptoms may return if activity is started too quickly, excessively, or with improper technique.
Prevention for Scapular Dyskinesis
Scapular dyskinesis can be avoided by:
- Warming up and stretching before throwing or performing any overhead tasks
- Observing age and league pitch count regulations if you participate in sports.
- Observing proper throwing technique is crucial, especially for kids participating in sports. Avoiding a range of motion when lifting, particularly when doing so overhead
FAQs
Why does scapula dyskinesia occur?
The muscles that regulate the scapula can become weak, unbalanced, tight, or (rarely) detached, which can result in scapular dyskinesis. Damage to the muscles’ supplying nerves. Damage to the shoulder joint or the bones supporting the scapula.
How should scapular dyskinesis be treated?
Using state-of-the-art equipment such as the Neuralgia System STM in conjunction with physical therapy exercises can significantly improve outcomes for individuals with scapular dyskinesis.
Why does the scapula injured?
Shoulder blade pain, or scapula pain, can be caused by several things, from strained muscles and bad posture to more serious disorders, including heart problems or rotator cuff injury. In addition to more serious causes, including spinal disorders, fractures, or referred pain from internal organs like the lungs or gallbladder, frequent causes include muscle strains and bad posture.
How is scapular dyskinesis tested for?
The Scapular Dyskinesis Test (SDT), which involves watching the scapula shift during arm flexion and abduction with weights, can be used to evaluate scapular dyskinesis. The test detects aberrant movement patterns, such as winging (scapula sliding away from the back) or dysrhythmia (premature or excessive elevation/protraction).
A scapular weakness: what is it?
Scapular dyskinesis is a shoulder condition that can occur when your shoulder blades are unstable. Your shoulder blades’ typical range of motion is one of their defining characteristics. It is sometimes a condition unto itself. In other cases, scapular dyskinesis is a sign of another injury or illness.
How serious is scapular dyskinesia?
It is called scapular dyskinesis or dysfunction when the scapula (shoulder blade) moves or functions abnormally. This is usually not the patient’s main complaint and is frequently a very modest anomaly. Nonetheless, it might be the root cause of the shoulder ache that is currently present.
Is there a cure for scapular dyskinesis?
Rehabilitation exercises, frequently performed with the assistance of an athletic trainer or physical therapist, can address the majority of irregularities in the scapular mobility or position. Depending on the extent of the injury, rehabilitation might often last four to eight weeks.
Can chest pain be a symptom of scapular dyskinesis?
A condition known as ST dyskinesis affects the bones and muscles of the chest and shoulders. It may result in pain, trouble breathing, and other issues. It’s crucial to consult a physician for a diagnosis and therapy if you suspect scapulothoracic dyskinesis.
What is the duration of scapular dyskinesis?
It can take several months of physical treatment to get your shoulder back to its natural alignment and range of motion. Particularly if the scapular winging occurs following an accident, some people experience symptoms for several years.
Which nerve is responsible for scapular dyskinesis?
A rare condition known as scapular winging is typically caused by injury to the long thoracic nerve, spinal accessory nerve, or, less frequently, the dorsal scapular nerve. Scapular dyskinesis, an aberrant scapulohumeral contact during kinetic motion, is the outcome of this damage.
What is the sensation of scapular dyskinesia?
These are the most common symptoms of scapular dyskinesis: The area around the scapula, especially the top and medial (inside) border, may be tender or painful. Arm weakness: When you try to use the affected arm actively, it may feel “dead” or exhausted. Exhaustion from repetitive tasks, particularly those involving overhead motions.
Reference
- Scapular dyskinesis. (n.d.). https://www.nationwidechildrens.org/specialties/sports-medicine/sports-medicine-articles/scapular-dyskinesis
- Panagiotopoulos, A. C., & Crowther, I. M. (2019). Scapular Dyskinesia, the forgotten culprit of shoulder pain, and how to rehabilitate. SICOT-J, 5, 29. https://doi.org/10.1051/sicotj/2019029
- Scapular (Shoulder blade) Disorders – OrthoInfo – AAOS. (n.d.). https://orthoinfo.aaos.org/en/diseases–conditions/scapular-shoulder-blade-disorders
- What is scapular dyskinesis? (2023, May 29). WebMD. https://www.webmd.com/a-to-z-guides/what-is-scapular-dyskinesis
- Scapular dyskinesis. (n.d.-b). Stanford Health Care. https://stanfordhealthcare.org/medical-conditions/bones-joints-and-muscles/scapular-dyskinesis.html
- Scapular dyskinesis. (n.d.-c). Stanford Health Care. https://stanfordhealthcare.org/medical-conditions/bones-joints-and-muscles/scapular-dyskinesis.html
- Panagiotopoulos, A. C., & Crowther, I. M. (2019b). Scapular Dyskinesia, the forgotten culprit of shoulder pain, and how to rehabilitate. SICOT-J, 5, 29. https://doi.org/10.1051/sicotj/2019029
- Kibler, B. W., Sciascia, A., & Wilkes, T. (2012). Scapular dyskinesis and its relation to shoulder injury. Journal of the American Academy of Orthopaedic Surgeons, 20(6), 364–372. https://doi.org/10.5435/jaaos-20-06-364