Spinal Accessory Nerve Palsy
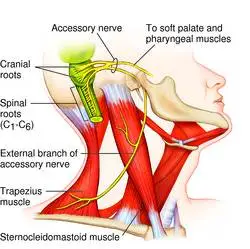
Spinal Accessory Nerve Palsy, also known as Accessory Nerve Palsy, is a neurological condition characterized by the dysfunction of the spinal accessory nerve (cranial nerve XI). This nerve is primarily responsible for innervating the sternocleidomastoid and trapezius muscles, which are essential for head rotation, shoulder elevation, and certain movements of the neck and scapula.
Damage to the spinal accessory nerve can lead to muscle weakness or paralysis, resulting in difficulties with shoulder movement and neck function.
Common causes of this palsy include surgical trauma, particularly during procedures involving the neck or upper back, as well as tumors, infections, or direct injuries. Early diagnosis and treatment are crucial to prevent long-term disability and to optimize recovery of muscle function.
What is the Spinal Accessory Nerve? Anatomy and its Function
- The accessory nerve supplies motor function (movement) to the larynx (voice box), various structures in the throat, and the two muscles necessary for movement of the neck and shoulders: the trapezius and the sternocleidomastoid (SCM). It is frequently called CN XI, the eleventh of the twelve cranial nerves.
- It has been classified as a cranial nerve, carrying messages from the brain to various regions of the body. It is divided into two sections. The brain is the source of one portion, and the spine is the source of the other. It is frequently referred to as the spinal accessory nerve because of this.
The spinal accessory nerve, or cranial nerve XI (eleven), regulates the sternocleidomastoid and trapezius muscles:
- The sternocleidomastoid muscle flexes your neck and aids in head rotation.
- The trapezius muscle controls shoulder movements like shrugging your shoulders. The trapezius muscle maintains the scapula, or shoulder blade, to provide a stable foundation for using your arm.
Anatomy
- The spinal accessory nerve (SAN), which is vital for preserving motor function, has a complicated anatomical course. It is divided into two sections: the cranial and the spinal. The spinal portion comes from the upper cervical segments (C1–C5/C6) of the spinal cord, whereas the cranial portion comes from the nucleus ambiguus in the medulla oblongata.
- After leaving the spinal cord, the nerve ascends via the foramen magnum and leaves the skull via the jugular foramen. The sternocleidomastoid muscles (SCM) and trapezius are then innervated by it.
Function
Since the accessory nerve only transmits motor signals, it only permits motion and not sensation.
Cranial Region
Some of the muscles in the pharynx, larynx, and soft palate can move because of the cranial component of the accessory nerve’s vagus nerve supply. Eating, speaking, and breathing are all facilitated by those head and throat structures.
Spinal Region
The spinal component of the auxiliary nerve innervates important muscles as well.
- Sternocleidomastoid (SCM)
- Trapezius
The range of motion in your upper body would be greatly restricted if your trapezius and SCM were not functioning. The trapezius muscle lifts and retracts the scapula and aids in shoulder abduction, whereas the SCM muscle rotates the head to the other side and flexes the neck.
What is the Spinal Accessory Nerve palsy?
- The disorder known as spinal accessory nerve palsy, or SAN palsy, results in weakening or paralysis in the neck and shoulder muscles. It happens when there is an injury to the spinal accessory nerve, which regulates these muscles.
- The most typical sign of spinal accessory nerve palsy is weakness or trouble raising the arm on the side that is affected. Persons who have spinal accessory nerve palsy may also experience neck or shoulder pain, as well as improper movement of their shoulder blades.
- Spinal accessory nerve palsy can be brought on by a variety of factors, including an infection, trauma, tumor, or surgery.
The underlying cause of spinal accessory nerve palsy affects the course of treatment. Physical therapy is the only treatment required in many cases. Increasing the range of motion and strengthening muscles are two benefits of physical therapy. Surgery can be required in certain cases to repair the injured nerve.
Causes of the Spinal Accessory Nerve Palsy
There are several causes of spinal accessory nerve palsy, such as:
- Inflammatory and Infectious Causes: Sarcoidosis, herpes zoster, and Lyme disease are a few illnesses that can harm a nerve.
- Blunt or Penetrating Trauma: A straight hit to the shoulder or neck can cause nerve damage.
- Surgical Trauma: Accidental injury caused during surgical procedures, specifically neck dissections for tumors, carotid endarterectomy, or lymph node biopsies, is the most common cause of surgical trauma.
- Tumors: The nerve may be compressed by tumors in the base of the head or neck.
- Idiopathic means: The exact cause of certain cases is yet unknown.
Symptoms of the Spinal Accessory Nerve Palsy
The following are the most common symptoms of spinal accessory nerve injury:
- Pain and weakness in the shoulder resulting from the weakening of the trapezius muscle are the most typical signs of injury to the spinal accessory nerve.
- The prominent medial border of the scapula causes scapular winging because the trapezius muscle cannot stabilize the scapula.
- Atrophy and Weakness in the Trapezius and Sternomastoid Muscles.
- Restricted range of motion in the shoulders.
- Abduction and overhead activities are difficult.
- Asymmetry in shoulder height and a drooping shoulder.
- These symptoms might greatly impact the quality of life in general and everyday activities.
Diagnosis of the Spinal Accessory Nerve Palsy
A routine physical examination is the first step in the diagnosis of spinal accessory nerve palsy. Your physician may use neurological testing and imaging methods like electromyography (EMG).
- Physical Examination: A comprehensive physical examination and history are essential. Muscle atrophy, range of motion, and strength should be the main areas of assessment. The function of the trapezius muscle can be examined with the use of certain tests, such as the scapular flip test and shoulder shrug test.
- Imaging Studies: Tumours and inflammatory processes are examples of structural reasons that can be found using magnetic resonance imaging (MRI) and computed tomography (CT scans). An ultrasound can help assess muscle atrophy.
- Electrophysiological Tests: To verify the diagnosis and determine the extent of the nerve damage, electromyography (EMG) and nerve conduction studies (NCS) are required.
Treatment of the Spinal Accessory Nerve Palsy
The underlying cause, the extent of the nerve damage, and the length of the symptoms all influence how spinal accessory nerve palsy is treated. Among the available treatments are:
Conservative Treatment
- Many spinal accessory nerve palsy cases, especially those caused by idiopathic causes or slight trauma, may get better with conservative care.
- Corticosteroid injections or NSAIDs for pain control may also be helpful.
- Botulinum toxin is useful in treating pain and muscular imbalance, especially when compensatory muscles become hyperactive.
- Physical therapy is part of this to enhance shoulder function and strengthen the residual muscles.
- Occupational therapy: It can assist patients in adjusting to modifications in shoulder function while improving their capacity to carry out everyday tasks.
Surgical Treatment
Surgical examination and nerve repair may be required in cases of severe damage or during neck procedures where the nerve is accidentally wounded. Procedures include muscular tendon transfers, nerve grafting, and transfers of nerves. One such method is Eden-Lange surgery, which involves re-aligning the rhomboid and levator scapulae muscles to correct for dysfunction of the trapezius. Scapulothoracic fusion is a commonly performed surgical technique.
Scapulothoracic (ST) Fusion
A restoration technique called scapulothoracic (ST) fusion is used to stabilize the scapula on the thorax. It includes the union of the scapula’s medial edge with the three to five ribs underlying. The elevation and abduction of the shoulder are greatly impacted by the scapulothoracic (ST) motion. When tendon transfer is ineffective in treating long thoracic nerve palsy and spinal accessory nerve palsy, this treatment is advised. Scapulothoracic fusion is also a treatment option for brachial plexus, facioscapulohumeral dystrophy, and medial clavicular insufficiency.
Procedure
The following are the fundamental procedures in scapulothoracic fusion surgery:
- The patient gets positioned on the operating table and given general anesthesia.
- A cut is made along the scapula’s medial edge.
- The underlying three to five ribs are then visible, as is the inner edge of the scapula bone along its entire length.
- Next, the nearby ribs are linked to the scapula.
- To encourage fusion, a bone stimulator is implanted together with a bone transplant at the contact point.
- The incision has finally closed.
- The entire process typically takes three to four hours, and the patient may need to spend three to five days in the hospital.
Post-operative care
- Patients who have had scapulothoracic fusions are recommended to pay attention to the following basic instructions: For the first six weeks after surgery, wear a sling and avoid using the affected extremity.
- Observe your therapist’s recommendations for exercise and activities during the healing period. The shoulder’s complete recovery could take six months or maybe a year.
Risk and Complication
While scapulothoracic fusion is a safe treatment, there are several dangers and problems to be aware of. These include:
- Metalwork malfunction
- Adhesive Capsulitis
- Bone nonunion
- Pneumothorax
- Pleural effusion
- Thoracic outlet syndrome
- Pneumonia
- Fracture of the scapula
- Deep Venous thrombosis
Physical Therapy for Spinal Accessory Nerve Palsy
Physical therapy plays an important role in the recovery from spinal accessory nerve palsy. A personalized rehabilitation plan with a focus on:
- Strengthening Exercises: To improve shoulder stability, focus on the deltoid and other compensating muscles.
- Range of Motion Exercises: To keep your body flexible and prevent stiffness.
- Postural training: To deal with compensatory alterations in posture that may result from weak muscles.
- Functional Training: The goal of functional training is to improve your daily function.
- A physical therapist must closely observe the patient to modify the rehabilitation program as needed.
Prognosis of the Spinal Accessory Nerve Palsy
The degree and cause of the damage decide the prognosis for spinal accessory nerve palsy. Persons with minor wounds or those who receive immediate medical attention typically have a good prognosis that improves progressively with time. Even with surgery, severe injuries especially those involving full nerve transection may leave a patient permanently impaired.
Summary
Spinal Accessory Nerve Palsy is a disorder with various causes and significant functional implications. spinal nerve palsy can cause paralysis or dysfunction. Early diagnosis and proper treatment are crucial for optimizing results. Therefore, you should visit a medical center for a checkup and diagnosis as soon as you feel you may have a sickness. You’ll regain better motor function if you receive treatment early.
FAQs
What occurs if there is injury to the accessory nerve?
A spinal accessory nerve injury may result in trapezius dysfunction. The trapezius is a primary stabilizer of the scapula and consists of three parts. Scapula elevation, rotation, and retraction help in scapulothoracic rhythm.
What is the eleventh cranial nerve?
The eleventh paired cranial nerve is the accessory nerve. It innervates the muscles of the sternocleidomastoid and trapezius, and it is a mainly motor function.
How are spinal accessory nerves tested?
Two muscles are examined while examining the accessory nerve: the sternocleidomastoid and trapezius. Request that the patient shrug their shoulders before applying resistance to test the trapezius. Weakness in the accessory nerve will show up as little to no resistance to your downward force.
How is spinal accessory nerve palsy treated?
A of treatments involving conservative care, physical combination therapy, and surgical restoration is used to treat spinal accessory nerve (SAN) damage and dysfunction of the trapezius muscle.
Which symptoms would you link to spinal accessory nerve damage?
The most frequent presenting symptom of spinal accessory nerve (SAN) injury is shoulder discomfort, whereas the most common sign is restricted or lack of sustained abduction of the shoulder.
References
- Dellwo, A. (2023, July 17). The anatomy of the accessory nerve. Verywell Health. https://www.verywellhealth.com/accessory-nerve-anatomy-4783765
- Cance- Resources from OncoLink, Treatment, Research, Coping, Clinical Trials, & Prevention. (n.d.). Spinal Accessory Nerve Palsy | OncoLink. University of Pennsylvania – OncoLink. https://www.oncolink.org/cancers/head-and-neck/side-effect-management-support-resources/spinal-accessory-nerve-palsy
- Spinal Accessory Nerve Palsy (SANP)-Treatment New Orleans LA. (n.d.). https://www.mistysurimd.com/patient-info/conditions-procedures/shoulder/spinal-accessory-nerve-palsy/
- What is spinal accessory nerve palsy (SAN)? (n.d.). Vinmec. https://www.vinmec.com/en/oncology-radiotherapy/medicine-information/what-is-spinal-accessory-nerve-palsy-san/
- Machens, A., Schmid, K. W., & Dralle, H. (2020). Advances in the diagnosis & surgical management of medullary thyroid carcinomas. In Elsevier eBooks (pp. 11–25). https://doi.org/10.1016/b978-0-323-66195-9.00002-9