Thorax Muscles
Introduction
The thorax muscles are a group of muscles located in the chest region that play a key role in respiration and upper body movement.
The thoracic wall comprises the subcostalis, transversus thoracis, innermost intercostal muscles, external intercostal muscles, and internal intercostal muscles. During breathing, these muscles are principally in charge of altering the thoracic cavity. The pectoralis major and minor, subclavius, and serratus anterior (anteriorly), as well as the primary costarum and serratus posterior superior and inferior (posteriorly), are additional muscles that connect to the thoracic wall but do not form it.
While the posterior thoracic muscles support the thoracic wall and aid in altering the thoracic volume during breathing, the anterior thoracic muscles allow arm and shoulder mobility. Another thoracic muscle that acts as the primary inspiration muscle is the diaphragm. Additionally, it separates the contents of the chest from those of the abdomen by forming the floor of the thorax. The sternocleidomastoid muscle and the scalene muscles are two other small accessory muscles that connect to the thorax and may also help in breathing to a little degree.
Structure
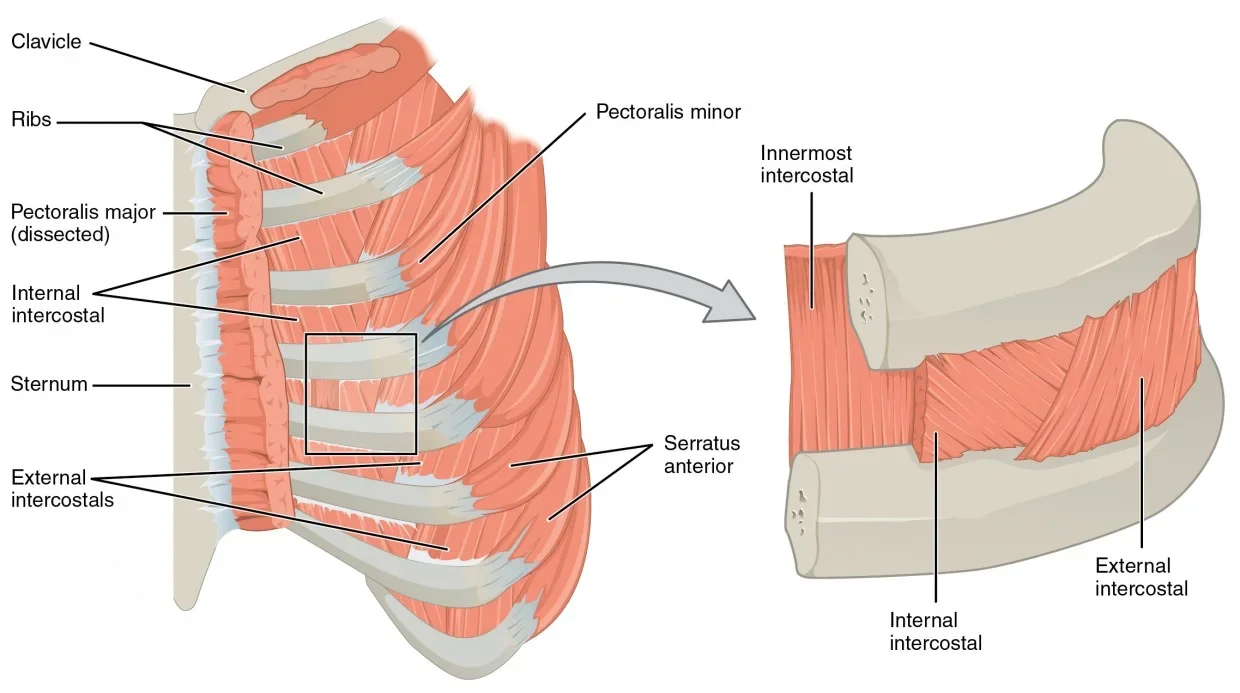
The subcostalis, transversus thoracis, and the three intercostal muscles (external, internal, and innermost) are the muscles that comprise the thoracic wall. Each intercostal gap has eleven pairs of intercostal muscles, numbered from superficial to deep. The external intercostal muscle is the most superficial layer; it attaches to the superior aspect of the rib below inferomedially after originate from the inferior side of the rib above. These muscles begin as thin connective tissue aponeuroses called the anterior (external) intercostal membrane, which stretch from the rib tubercle posteriorly and adhere to the costochondral junction anteriorly.
The intermediate layer is made up of the internal intercostal muscle. In a path perpendicular to the external intercostal muscles, these muscles attach to the superior side of the rib below from the lateral aspect of the costal groove of the rib above. Furthermore, these muscles continue as the posterior (internal) intercostal membrane from the rib cage posteriorly to the sternum anteriorly.
The innermost intercostal muscles comprise the deepest layer of the thoracic wall. They attach to the internal side of the rib below after emerging from the medial aspect of the costal groove of the rib above. The endothoracic fascia, which is only visible on the outside of the lungs’ parietal pleura, lines these muscles on the inside. During forced expiration, they are believed to work in conjunction with the internal intercostal muscle.
The thoracic wall is composed of the intercostal muscles as well as the subcostalis and transversus thoracis. The subcostalis muscle is abundant in the lower parts of the posterior thoracic wall and is located in the same layer as the innermost intercostal muscle. They attach to the inside of the second or third rib below after emerging from the inside of one of the lower ribs. The deepest intercostal muscle is also where the transversus thoracis is located. They start in the lower posterior sternum, move into the thoracic cage’s interior, and attach to ribs two through six.
The levatores costarum attaches to the rib below after emerging from the transverse processes of C7 to T11. Raising the ribs just slightly facilitates inspiration. While the serratus posterior inferior joins the vertebrae to ribs 8 through 12 and depresses them during forced expiration, the serratus posterior superior attaches to ribs 2 through 5 and lifts them during inspiration. Together with the thoracic wall muscles, these muscles support the thoracic wall overall and help change the thoracic volume during breathing.
The pectoralis major and minor, subclavius, and serratus anterior muscles are among the other thoracic muscles that are involved in upper limb movement. The pectoralis major attaches to the lateral lip intertubercular sulcus of the humerus after originating from the medial half of the clavicle, anterior sternum, first seven costal cartilages, and aponeurosis of the external oblique. Its purpose is to medially rotate, flex, and adduct the arm at the glenohumeral joint.
Its sternoclavicular head causes the flexed arm to extend, whereas its clavicular head causes the extended arm to flex. The deep fascia covering the associated intercostal gaps and the anterior surfaces of ribs three through five are the origins of the pectoralis minor muscle, which inserts on the scapula’s coracoid process. Its primary purpose is to protract the scapula and depress the shoulder point. As an auxiliary muscle, it may also support respiratory efforts by raising the third, fourth, and fifth ribs during inspiration. The subclavian groove of the clavicle is where the subclavius muscle enters, after starting at the first rib’s costochondral junction. It serves to keep the clavicle stable.
The serratus anterior muscle inserts along the superior angle, medial border, and inferior angle of the scapula after starting on the superolateral surfaces of the first to eighth or first to the ninth ribs at the thoracic lateral wall. Because of its primary role in protracting the scapula while punching, it is sometimes referred to as the “boxer’s muscle,” which aids in scapular rotation. When the shoulder girdle is stabilised, the serratus anterior may also help with inspiratory attempts by raising the ribs.
Function
In a bucket-handle action, the external intercostals flex during inspiration, raising the lateral portion of the ribs and expanding the thorax’s transverse width. Because of their configuration, they can compress the ribs during forced expiration, which lowers the thoracic volume. Furthermore, these muscles continue as the posterior (internal) intercostal membrane from the rib cage posteriorly to the sternum anteriorly.
During forced expiration, the transversus thoracis and subcostalis muscles help to compress the ribs. The transversus thoracis and the subcostalis Breathing may also be facilitated by muscles of the posterior thorax, including the serratus posterior superior and inferior and the levatores costarum.
However, the diaphragm is the main inspiration muscle. Peripherally, the diaphragm is connected to the lumbar vertebrae (lumbar component), the xiphoid process (sternal portion), the costal border of the thoracic wall, and the lower sixth ribs. The diaphragm is flattened during inspiration as the muscle contracts and pulls down its inferior central tendon. This movement raises the thorax’s vertical diameter and negative thoracic pressure, which eventually pushes air into the thoracic cavity.
The diaphragm relaxes and rises during expiration, causing the air in the lungs to leave the body. The sternocleidomastoid muscle, which helps raise the sternum, and the scalene muscles, which raise the first and second ribs, are other accessory muscles that support inspiration. In addition to helping with breathing, the diaphragm also helps in straining the abdomen and raises intra-abdominal pressure when it contracts during micturition, defecation, and even lifting weights.
Blood Supply
The muscles of the posterior thorax and thoracic wall are primarily supplied by the intercostal arteries. Three arteries (two anterior and one posterior) supply each intercostal gap. These arteries anastomose laterally between the innermost intercostal muscle and the interior intercostal muscle in the costal groove.
The superior (supreme) intercostal artery, which in turn emerges from the costocervical trunk of the subclavian artery, is the source of the posterior intercostal artery of the first two intercostal gaps. A pair of subcostal arteries and the remaining posterior intercostal arteries from the third to eleventh intercostal spaces emerge straight from the descending thoracic aorta.
Nerve Supply
The intercostal nerves, which mostly originate from the anterior rami of spinal nerves T1 to T11, innervate the muscles that make up the thoracic wall and the posterior thorax. Spinal nerve T12’s anterior ramus is a subcostal nerve. While their efferent fibers carry motor information to the muscles of inspiration, their afferent fibers supply sensory information to the skin that covers it. Notably, the lower trunk of the brachial plexus is formed by just a piece of the anterior ramus of spinal neurone T1, whereas the rest of the intercostal nerves do not create plexuses.
Several branches of the brachial plexus provide innervation to the muscles of the anterior thorax. Both the medial pectoral nerve, which innervates the sternocostal head, and the lateral pectoral nerve, which innervates the clavicular head, innervate the pectoralis major. The medial pectoral nerve supplies innervation to the pectoralis minor.
The brachial plexus’s lateral cord gives rise to the lateral pectoral nerve, whereas the medial cord gives rise to the medial pectoral nerve. The subclavius muscle, which emerges from the superior trunk of the C5 to C6 nerve roots, is innervated by the subclavius nerve. If it exists, the subclavius muscle may additionally receive motor innervation from the accessory phrenic nerve, which mostly contributes from C5. Finally, the long thoracic nerve, which emerges from the anterior rami of C5 to C7, innervates the serratus anterior.
Both the left and right phrenic nerves, which emerge from the anterior rami of C3 to C5, innervate the diaphragm. The phrenic nerve supplies the parietal pleura and peritoneum, which cover the central region of the diaphragm, with sensory innervation as well as the motor innervation necessary for the diaphragm to contract during inspiration. The diaphragm’s periphery receives sensory innervation provide the bottom six intercostal nerves.
Muscle Supply
The following are some of the thoracic muscles covered in this article:
Thoracic Wall
Intercostal muscles
- External intercostal muscle
- Internal intercostal muscle
- Innermost intercostal muscle
Subcostalis
Transversus thoracis
Posterior Thorax
- Levatores costarum
- Serratus posterior superior and inferior muscles
Anterior/Superficial Thorax
- Pectoralis major and minor muscles
- Subclavius
- Serratus anterior
Floor
- Diaphragm
Intercostals
The intercostal space between the ribs is home to the intercostal muscles. Three levels make up their organisation.
External Intercostals
Eleven pairs of external intercostal muscles are present. They are continuous with the external oblique of the abdomen and extend inferoanteriorly from the rib above to the rib below.
Attachments: Originated at each rib’s lower edge and attaches to the rib’s superior edge below.
Actions: Maintain the ribs’ natural posture when breathing. raises the thoracic volume and elevates the ribs during forced inspiration.
Innervation: Intercostal nerves (T1-T11).
Internal Intercostals
About the external intercostals, the internal intercostals are deep. They extend inferoposteriorly, or in the opposite direction as the external intercostals, from the rib above to the one below.
They run parallel to the abdominal wall’s internal oblique muscle.
Attachments: Originated from the costal groove’s lateral edge and attaches to the rib’s superior surface below.
Actions: Maintain the ribs’ natural posture when breathing. reduces the thoracic volume and depresses the ribs during forced expiration.
Innervation: Intercostal nerves (T1-T11).
Innermost Intercostals
Similar in structure to the internal intercostals, the innermost intercostals are the deepest of the intercostal muscles.
The intercostal neurovascular bundle divides them from the internal intercostals. They are located in the intercostal spaces’ most lateral region.
Attachments: Insert into the superior surface of the rib below after emerging from the medial margin of the costal groove.
Actions: Stabilizes the position of the ribs during normal respiration. Depresses the ribs and decreases the thoracic volume during forced expiration.
Innervation: Intercostal nerves (T1-T11)
Transversus Thoracis
Situated on the inside of the thoracic wall, the transversus thoracis is inferiorly continuous with the transversus abdominis.
Attachments: originate from the lower ribs’ costal cartilage and the posterior aspect of the inferior sternum. The fibres climb up and adhere to the inside of costal cartilages 2–6.
Actions: weak depressor upon expiration.
Innervation: Intercostal nerves (T2-T6).
Subcostales
The inferior part of the thoracic wall has the most developed subcostal muscles. The fibres run in a similar way to the innermost intercostal muscles.
Attachments: originates on the lower ribs’ inferior surface. connects to the second or third rib’s superior border below.
Actions: Maintain the ribs’ natural posture when breathing. reduces the thoracic volume and depresses the ribs during forced expiration.
Innervation: Intercostal nerves.
Embryology
Mesoderm differentiates to become skeletal muscle. To create somites, the paraxial mesoderm groups together with the neural tube throughout the fourth to eighth weeks of human development. The dorsolateral dermomyotome and the ventromedial sclerotome are the two cell types that result from the differentiation of these somites. While the sclerotome develops the axial skeleton, the dermomyotome forms the skeletal muscle, including the thoracic muscles and the skin’s dermis.
Anatomical Variation
Numerous investigations have documented the presence of anatomical differences in the thoracic muscles, either as a result of congenital abnormalities or supernumerary muscles. Eight percent of people have the sternalis muscle, an uncommon supernumerary muscle type of the anterior thoracic wall that runs parallel to the right sternal edge and vertically between the superficial and pectoral fascia. Its dimensions are around 7.0 cm in length and 2.9 cm in breadth. The sternalis muscle is believed to serve an auxiliary function in the elevation of the lower chest wall or to be involved in shoulder joint movement.
It can manifest unilaterally (4.5%) or bilaterally (less than 1.7%). Its embryological genesis and innervation are still hotly debated. According to several studies, the intercostal nerves (43%), the external or internal thoracic nerves (55%), or both (2%), innervate the muscle. Furthermore, some research has hypothesised that it is a derivation of the dermomyotomes or hypaxial myotomes, which are the source of the ventral and lateral body wall muscles of the abdomen and thorax. However, additional research supports the idea that a failure in muscle patterning causes the muscle to grow from either the pectoralis major or the rectus abdominis sheath.
The sternalis muscle has never been associated with any clinical symptoms in cases; however, because of its parasternal location and relative unfamiliarity to radiologists, its presence may result in changes in the ECG or lead to incorrect diagnoses of breast masses (such as breast carcinoma or haematoma) on routine mammography. If not identified before surgery, it may cause complications and delay cardiothoracic and breast procedures. The sternalis muscle can be used as a muscular flap in reconstructive procedures for the breast, head and neck, and anterior chest wall if it is identified before surgery.
Different degrees of congenital abnormalities can also result in anatomical differences of the thoracic muscles. The loss of the pectoralis major muscle’s sternocostal head, changes in the pectoralis minor muscle’s hypoplasia or absence, and even digital abnormalities are the hallmarks of Poland syndrome. Excavatum deformities, rib aplasia, and the absence or hypoplasia of the ipsilateral breast are further abnormalities linked to Poland syndrome.
Although certain investigations have shown the uncommon occurrence of bilateral symptoms, these anomalies are usually unilateral and located on the right side. From modest hypoplasia of the pectoralis major muscle to severe hypoplasia of the thoracic wall, there are several variants of the disease that have been reported.
Clinical Importance
The use of accessory respiratory muscles to support respiratory efforts can be a normal finding during periods of high physiologic demand, such as exercise or even singing, but their presence in patients at rest may indicate a pathological cause, such as an asthma attack, which calls for additional assessment, medical management, and treatment. Examples of accessory respiratory muscles include the muscles of the abdomen, latissimus dorsi, internal intercostals, transversus thoracis, pectoralis major and minor muscles, serratus anterior, serratus posterior superior and inferior, latissimus dorsi, and trapezius.
Surgical Importance
Surgical procedures that involve the thorax muscles often entail chest tube installation and needle treatment for either decompression or anaesthetic.
To remove pathological air or fluid from the pleural cavity, a tube thoracostomy is done. To reduce the chance of harming the blood vessels and nerves that run on the inferior part of each rib, a chest tube is often positioned at the level of the fourth or fifth intercostal gap above the rib, between the mid- to anterior axillary line. The parietal pleura will be reached when the incision is done and the tube is introduced. It will pass through the skin, superficial fascia, serratus anterior muscle, external intercostal muscle, internal intercostal muscle, and innermost intercostal muscle.
Similar to tube thoracostomy, needle thoracostomy is another decompressive treatment that is commonly used in situations with tension pneumothorax. The second intercostal space at the midclavicular line or the fourth and fifth intercostal spaces at the anterior axillary line above the rib are the two possible locations for the needle.
The purpose of an intercostal nerve block is typically to relieve pain from rib fractures or even herpes zoster. The needle is placed beneath the rib and passes through the superficial fascia, serratus anterior muscle, external intercostal muscle, internal intercostal muscle, and layers of skin before reaching the intercostal nerve for anaesthesia. Because of the presence of nerve collaterals and significant overlap of contiguous dermatomes, the surgeon must also anaesthetise the adjacent intercostal nerve to accomplish pain relief.
FAQs
What are the 4 main structures of the thorax?
Organs, blood arteries, nerves, and other vital bodily parts are all located in the thoracic cavity, a region in the chest. The mediastinum, left pleural cavity, and right pleural cavity are its three primary sections. Your heart, lungs, esophagus, trachea, and thymus are the five organs that make up your thoracic cavity.
Is the diaphragm a muscle?
The main respiratory muscle is the diaphragm, which is situated beneath the lungs. It is a big, dome-shaped muscle that contracts continuously and regularly, usually without conscious thought. The diaphragm flattens and contracts during inhalation while the chest cavity expands.
Which three purposes does the bony thorax serve?
The pleural cavity walls and the breathing diaphragm are supported by the bony thorax. Because of the way the thorax is built, the volume of the thoracic cavity may change when breathing. The lungs and heart are likewise shielded by the thorax.
What are the two types of intercostal muscles?
The Intercostal Muscles
The internal and external intercostals are the two types of these muscles that are located between the ribs.
References
- Tang, A., & Bordoni, B. (2023, July 24). Anatomy, thorax, muscles. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK538321/
- TeachMeAnatomy. (2024f, November 9). Thoracic Muscles – Attachments – Actions – TeachMeAnatomy. https://teachmeanatomy.info/thorax/muscles/thoracic-cage/