Tardieu Scale/Modified Tardieu Scale
Introduction
The Tardieu Scale is a clinical tool used to assess muscle spasticity, particularly in individuals with neurological conditions such as cerebral palsy or after stroke. In 1954, Tardieu and colleagues created the Tardieu Scale. It was changed in 1969 by Held and Pierrot-Deseilligny, and then in 1999 Boyd and Graham made more changes.
Purpose
By measuring the muscle’s reaction to various stretch velocities and figuring out the spasticity angle, these scales aim to measure spasticity.
Tardieu scale has been applied in the following populations: stroke, spinal cord injury, multiple sclerosis, cerebral palsy, traumatic brain injury, young hypertonia, and central nervous system lesions.
Technique
R2 and R1 will be measured using a conventional goniometer. Additionally, the stretching velocity of V3 will be used to measure the quality of muscle response. The measure of the dynamic component of spasticity will be the difference between R2 and R1.
Scoring
Quality of Muscle Reaction
- 0- No resistance at all during the static phase
- 1- Mild resistance the entire time, lacking a distinct catch at a specific angle
- 2- Clear catch at an exact angle, then release
- 3- Possibly Clonus within a given time frame (less than 10 seconds)Fatiguable clonus (less than 10 seconds) at a specific angle
- 4- Identifiable Clonus (> 10 seconds) at a specific angle
- 5- Joint immobilised
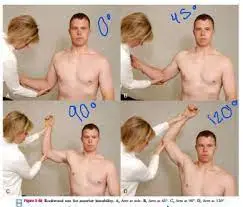
Velocity to Stretch
- V1: Most slowly possible
- V2: The limb segment’s falling speed (against gravity)
- V3: very rapidly (>gravitational pull)
Evidence
Reliability:
- No research has been done to investigate the Modified Tardieu Scale’s internal consistency in stroke patients. There is great test-retest reliability using inertial sensors and goniometry. The intra-rater dependability was investigated in two investigations. R1 measurements, as opposed to spasticity angle or subjective assessments of spasticity, are the most reliable basis for repeated Modified Tardieu Scale evaluations of spasticity.
- It is commonly known that the observed angles exhibit significant variations in size. Consequently, conclusions on the validity of the Modified Tardieu Scale. cannot be made due to the lack of consistency between studies, muscle groups, and GMFCS levels.
- It is thought that an experienced clinician with sufficient training and experience can obtain a measure that is the best. Having a single rater complete the measurements in a regulated test setting is another method to get the most dependable measurements.
Validity:
- The content was not previously studied. Not enough study has been done to determine whether this scale is a reliable indicator of spasticity. Nonetheless, it is thought to be congruent with the accepted definition of spasticity and is the only clinical assessment now in use that measures the location in the muscle’s range where spasticity is happening.
Responsiveness:
- Researchers have shown that repeated measures over time for hip adductors and hamstrings with various raters can vary by 10-18°, and with the same rater by 4-19°. There was no specific research on responsiveness to change after interventions that could be located.
FAQs
What is the assessment using the modified Tardieu scale?
The Modified Tardieu Scale is used to assess a person’s muscle response to movement and whether or not they have spasticity. Which treatment interventions are taken into consideration to help lessen this condition can be determined by the outcomes.
What differentiates Tardieu from modified Ashworth?
In order to address this, the Tardieu Scale is the only tool that includes passive muscle stretches at three distinct speeds. This allows for a more thorough evaluation of spasticity. The Ashworth Scale, on the other hand, gauges passive resistance to movement at a single speed.
What is the stroke Tardieu scale?
Exaggerated deep tendon reflexes that impair speech, mobility, gait, and muscle activity are its defining features. After a stroke, spasticity may rise at first and then decrease.
What differentiates Tardieu scale members R1 and R2 from one another?
During a quick passive stretch, the angle of catch, or R1, is where a sudden increase in muscular resistance is sensed.
In the Tardieu scale, what differentiates spasticity from contracture?
A little score for R2-R1 implies contracture, whereas a big value denotes spasticity. The X score describes forms of muscle resistance when passive stretches are given during the evaluation (grade 0–5).
References
- Tardieu Scale/Modified Tardieu Scale. (2016, March 1). Shirley Ryan AbilityLab. https://www.sralab.org/rehabilitation-measures/tardieu-scalemodified-tardieu-scale
- Cerebral Palsy Alliance Australia. (2024, August 5). Modified Tardieu Scale | Cerebral Palsy Alliance. Cerebral Palsy Alliance. https://cerebralpalsy.org.au/cerebral-palsy/assessments-outcome-measures/modified-tardieu-scale/