Supraspinatus Tendonitis
What is a Supraspinatus Tendonitis?
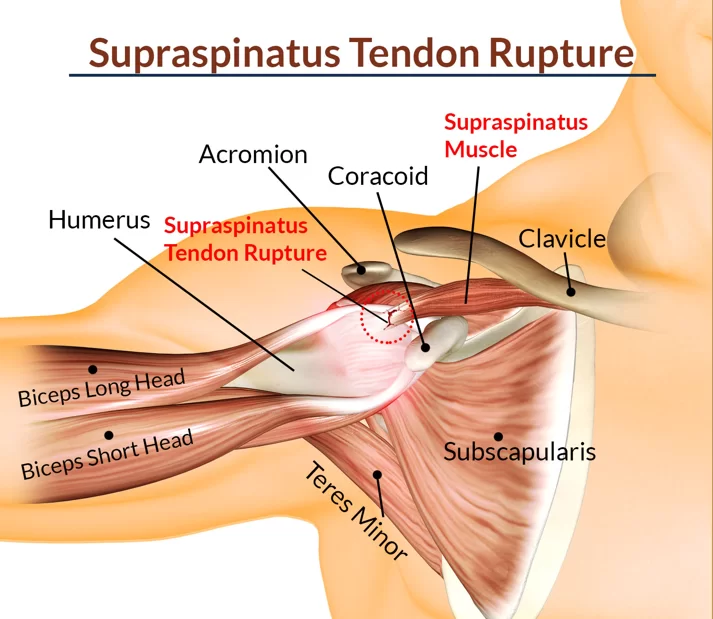
Supraspinatus tendonitis, also known as rotator cuff tendonitis, is a common cause of shoulder pain and dysfunction. It involves inflammation of the supraspinatus tendon, which is one of the four tendons that comprise the rotator cuff.
A common shoulder problem is supraspinatus tendonitis, which has been also referred to as “Shoulder Impingement Syndrome” or “Painful Arc Syndrome.”
One in five persons may have symptoms of shoulder impingement syndrome at some point in their lives, making it the most common condition. Supraspinatus symptoms might develop gradually over years without a clear reason, or they can appear quickly following an accident.
When rotating the arm between 60 and 120 degrees of abduction, the tendon gets compressed against the bone, causing a painful arc that is a common warning sign of supraspinatus tendonitis.
Painful arc syndrome usually first manifests as middle-aged symptoms, most often in the 45–65 age range.
Supraspinatus tendonitis is usually an overuse disease caused by repeated rubbing on the tendon; however, impingement, instability, or injuries to the shoulder can also cause it.
Anatomy
The posterior boundary of the rotator interval, which divides the supraspinatus from the rolled superior border of the subscapularis, defines the anterior margin of the supraspinatus. The expansion of the spine between the supraspinatus and infraspinatus around the scapular spine indicates the posterior margin of the supraspinatus. It has been demonstrated that the posterior part of the supraspinatus is short and thin, whereas the anterior portion is made up of a long, thick tendinous component.
An examination of the supraspinatus impression anatomic dissection showed that the tendon’s normal anterior-to-posterior dimension was 25 mm, and its normal thickness was 12 mm. The mean distance between the cartilage and the supraspinatus footprint was 1.5 mm at the mid-tendon.
1.5 centimeters in front of their insertions, the supraspinatus and infraspinatus tendons combine. Greater than 95% of the collagen in the supraspinatus tendons is type I collagen, with smaller levels of other collagens, such as type III,
The extracellular matrix composition of the supraspinatus is greatly affected by its anatomy, which can be divided into four growth zones. The proper tendon, which contains mostly type I collagen and tiny amounts of decorin, is the first zone. Types II and III collagen predominate in the second zone of fibrocartilage, with trace levels of types I, IX, and X collagen.
Type II collagen predominates in the third zone of mineralized fibrocartilage, which also contains significant amounts of type X and aggrecan. Bone makes up the fourth zone and is primarily composed of type I collagen with a high mineral concentration. The functional grading of mineral concentration and collagen fiber exposure results in this effective bone-tendon connection.
What’s Happening in Supraspinatus Tendonitis?
Pain in the shoulder is frequently caused by supraspinatus tendonitis. The ball and socket joint that forms the shoulder is made up of the following:
- The rounded upper arm bone is Humerus’s head.
- Glenoid Fossa: the shallow socket on the shoulder blade’s lateral angle.
The body’s greatest range of motion is located in the shoulder joint. While the bone structure of other joints provides stability, the shoulder gives up bone stability in favor of mobility. Evaluate how much more range of motion your arms provide compared to your legs. However, because of its extensive range of motion, the shoulder is outlying more weak to injury.
The shoulder’s rotator cuff muscles are the subscapularis, supraspinatus, infraspinatus, and teres minor.
The primary dynamic stabilizing muscles of the shoulder, the supraspinatus, infraspinatus, teres minor, and subscapularis, work together as the rotator cuff to balance.
The acromion process, a bony projection at the top of the scapula that forms a joint with the clavicle, also known as the collarbone, forms an arch under which the rotator cuff muscles, which originate from the scapula, connect through their tendons to the head of the humerus.
The supraspinatus traverses the upper portion of the shoulder blade. The “subacromial space” is the little passage that the supraspinatus tendon uses to travel between the acromion and the head of the humerus.
The subacromial space has been packed with the following and is just 7–14 mm deep. The space in the shoulder between the acromion and the humerus head is known as the subacromial space. The supraspinatus tendon A fluid-filled sac called the subacromial bursa aids in lowering friction within the subacromial region.
Joint Capsule: the upper part of the sac that surrounds the joint Long Head of Biceps Tendon
When the arm is elevated to shoulder height, especially when internally rotated (thumb pointing down), the subacromial space narrows significantly. When the arm is raised higher and externally turned (thumb pointing up), the space is renewed.
Supraspinatus tendonitis: what causes it?
There are three primary reasons for supraspinatus tendinitis:
Repeated usage of the shoulder joint may result in inflammation of the supraspinatus tendon and other nearby rotator cuff tendons, including the biceps tendon.
Bad posture might cause your shoulders to extend forward, which may compress your supraspinatus tendon under the acromion, a bony protrusion. It then experiences continuous compression, which burns and inflames the area. Shoulder impingement syndrome, also known as subacromial supraspinatus impingement, is the clinical term for this condition.
The tendon may impinge in three different locations:
- Under the coracoacromial ligament,
- On the glenoid rim, or under the acromion.
- Between the acromion and the coracoid process is where the coracoacromial ligament is attached.
Direct blow: The supraspinatus tendon may become inflamed and damage shoulder function if you fall upon or strike your shoulder.
Ligament laxity: An unstable joint results from weak, hanging ligaments in the shoulder. Tendinitis may result from the rotator cuff tendons requiring more effort to stabilize them during movement
Repetitive rubbing on the tendon or repeated squashing or “impinging” of the tendon in the subacromial region can cause supraspinatus tendonitis. This causes inflammation and the tendon to gradually degenerate. Over time, the supraspinatus tendon may also support tears, which could result in a partial or total rotator cuff tear.
Some of the most common causes of painful arc syndrome:
- Repetitive overhead activities include sports like tennis and swimming as well as gardening tasks like pruning and wall trimming that require your arm to be raised repeatedly.
- Heavy Work: For example, workers and builders who frequently move large objects overhead
- Posture: a prolonged forward slump narrows the subacromial space.
- Genetic Propensity: genetic association
- Injury: such as a fall onto an extended hand
- Age: Because of wear and tear, the subacromial space tends to narrow with age.
- Primary Shoulder Impingement: The subacromial space is reduced by bone spurs or an unusual acromion position or form.
- Dynamic shoulder instability, or secondary impingement, is caused by rotator cuff weakness, which affects control and increases friction.
Above the Spine, While tendinitis can occur alone, it is frequently connected to additional shoulder issues like:
- Subacromial Bursitis
- Shoulder impingement Syndrome
- Biceps Tendinitis
- Rotator cuff tears
Many related injuries will have similar symptoms and treatments, but it is always important to learn more about them. Supraspinatus symptoms might develop gradually over years without a clear reason, or they can appear quickly following an accident.
When rotating the arm between 60 and 120 degrees of abduction, the tendon gets compressed against the bone, causing a painful arc that is a common warning sign of supraspinatus tendonitis.
Symptoms of Supraspinatus Tendonitis
It is common for mild supraspinatus tendonitis to go undiagnosed, but shoulder and upper arm pain is usually what causes people to seek medical attention. Initially, only repetitive or prolonged overhead or reaching actions typically cause supraspinatus pain. As the disease improves over time, weakness, stiffness, and pain in the arms and shoulders at rest can start to affect function.
Symptoms of supraspinatus tendonitis can appear as:
- Suddenly: following a shoulder trauma
- Gradually: over some time without a clear-cut reason.
Among the typical signs of painful arc syndrome are:
- Shoulder Pain: A sharp, stabbing pain that may sometimes travel down the middle of the upper arm to the elbow, but is more often felt at the top and front of the shoulder and outer arm when at rest. Additionally, there might be sudden, severe pain when twisting or reaching up or out to the side of the arm.
- Supraspinatus Tendonitis, also known as Painful Arc Syndrome, often appears as a painful arc of movement during shoulder abduction.
- A painful arc appears when moving the arm out to the side, typically ranging from 80 to 120 degrees of shoulder abduction.
- Outside of this range, movement is sometimes pain-free, but inside it, lifting and lowering down are usually very painful. The term “Painful Arc Syndrome” comes from the fact that this is the typical sign of supraspinatus tendinitis.
- Shoulder and Arm Weakness: A full-thickness rotator cuff tear, also known as a supraspinatus tendon full-thickness tear, is indicated by serious weakness or weakness without pain.
- Functional Limitation: Pain and restriction may occur from any activity that is at or above shoulder height, such as reaching up to hang laundry or wash/brush your hair.
- Sleep disturbance: When lying on the affected side, at night pain is frequently experienced as a result of supraspinatus tendonitis.
- Complete PROM: While pain may prevent you from moving your shoulder actively, as long as there are no accompanying shoulder impingement issues, passive movement—moving your arm with another person while your muscles are relaxed—is usually full or almost full in cases of pure supraspinatus tendonitis.
Diagnosing Supraspinatus Injuries
Your doctor or physical therapist may typically diagnose supraspinatus tendonitis by asking you about your symptoms and doing a shoulder examination. An MRI or ultrasound scan may also be recommended if a partial or full-thickness tear of the supraspinatus tendon is thought to be present.
The following tests are commonly used to detect supraspinatus tendonitis:
- Hawkins Kennedy test for shoulder supraspinatus tendonitis
- Kennedy Hawkins Test Position: Elbow flexion and shoulder support in a 90-degree angle
- Test: Push your forearm down to internally rotate your shoulder. The test is repeated while the arm is moved into various adduction positions around the body.
Good Outcome: Shoulder pain
Jobe’s Test or Empty Can Test
Position: With thumbs pointing towards the sky, both arms are elevated to 90 degrees abduction and 30 degrees forward flexion.
Test: Rotate your arms till your thumbs point downward. The examiner presses down with forearms as the patient pushes back against the motion.
Positive Outcome: Shoulder pain
Supraspinatus tendonitis is probably not the issue if one of these tests indicates any pain.
Treating Supraspinatus Tendonitis
Pharmacology treatment
Drugs
When suffering from painful arc syndrome, painkillers, and anti-inflammatory tablets or gels can help reduce discomfort and inflammation.
Injections of Corticosteroids
When treating supraspinatus tendonitis, a steroid and local anesthetic injection can help reduce discomfort and inflammation and promote healing.
It is important to take it easy for a few days and withhold from doing any heavy lifting because steroid injections can temporarily weaken the tendon and increase shoulder pain. Three shoulder injections should be the maximum number you receive every year.
Physical Therapy
The following therapies work best for supraspinatus tendonitis:
Deep transverse friction Massage (DTFM)
A particular kind of connective tissue massage called transverse friction is applied transversely across the tendon fibers. When performed properly, deep transverse friction massage speeds up the healing of the injured tendon reduces pain and inflammation associated with supraspinatus tendonitis, and improves function by:
- Hyperemia: An increase in the area’s local blood flow
- Increase in local temperature due to the Local Heat Effect
- Removing chemical Irritants: this reduces the sensitivity of nearby nociceptors, which in turn makes pain receptors less sensitive.
Reduce Local Oedema: reducing tendon swelling
- Mobilize Adhesive Scar Tissue: in the supraspinatus tendon, this facilitates the breakdown of abnormal cross-fibers and disliked scar tissue, thereby preventing the formation of adhesions. This increases tensile strength and aids in rearranging the damaged tendon fibers in their proper position.
- The analgesic effect is achieved by applying mild pressure across the supraspinatus tendon until the affected area becomes numb. The depth of pressure is now progressively increased without causing pain. The severity of the injury will determine how long and how often you receive treatment.
- A physical therapist or other qualified professional should be the only one performing transverse friction massages because their effectiveness depends on their understanding of the anatomy and structural organization of the tissue. They must be applied to the specific location of the supraspinatus tendonitis lesions, in the right direction, at the right depth, for the right amount of time, and frequently enough.
Sufficient Sleep
Avoiding activities that aggravate your shoulder pain is important if you have supraspinatus tendonitis because this will lessen the strain on the tendon and allow it to heal. Failure to do so raises the possibility of a full-thickness tear of the supraspinatus tendon developing.
Modify Sport Techniques
Seek professional guidance on how to strengthen your technique to reduce the strain through the rotator cuff to prevent further irritation and damage to the supraspinatus tendon if your painful arc syndrome is associated with sports.
Massage with Ice Cubes
For ten minutes, rubbing a moist ice cube over the tendon’s sensitive area can help reduce localized pain and inflammation.
Individuals experiencing painful arc syndrome must consult a physical therapist. They will perform a thorough evaluation of your shoulder and find any possible causes of the issue.
The course of physical therapy for supraspinatus tendonitis will depend on the results of the examination and could involve:
- Exercises to strengthen the muscles of the shoulder, rotator cuff, and shoulder blade
- Posture Work: to help expand the subacromial space and improve posture
- Stretching exercises: to relieve tense muscles in specific areas
- Ultrasound: to help realign tendon fibers and reduce inflammation
Exercise for supraspinatus Tendonitis
- Pendulum exercise

Your pain could decrease if you become more flexible. Your range of pain-free motion can also be increased with the aid of stretching exercises. Take regular breaths when working out. And make an effort to move easily and effectively.
Observe any particular guidance that you accept. Stop the workout if you experience pain. After the pain stops, give your physician a call.
- The directions for the pendulum exercise are as follows. If necessary, ask your physical therapist to walk you through the activity.
- Place your good arm on a table or chair and lean over. This workout can be done while sitting or standing. To find out which position is best for you, ask your physical therapist.
- Let the arm that is hurting hang down straight and relax.
- Start swinging the at-ease arm slowly. If you can, move it in a small circle while gradually enlarging it. Next, change the direction. After that, move it forward and backward. Lastly, give it a side-to-side swing.
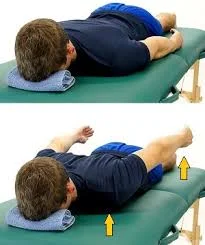
2. Isometric External Rotation of the Shoulder
Exercises that strengthen the infraspinatus and teres minor, two important rotator cuff muscles, include isometric shoulder external rotation.

To perform the exercise:
- Maintain your perpendicular position, about six inches away from a wall.
- The shoulder that you are working on should be the one nearest the wall.
- Making a fist and pressing the back of your hand against the wall as though you were twisting your arm outwards will cause you to bend your elbow to a 90-degree angle.
- If you need a little extra padding, use a small towel.
- Press into the wall gently for around five seconds.
- Release the wall’s pressure gradually.
- If you experience an increase in pain, stop exercising.
- After completing 10 to 15 reps, move on to the following isometric rotator cuff exercise.
3. Scapular retraction.
The purpose of the standing scapular retraction, also known as the waste squeeze, is to strengthen the muscles that run between your shoulder blades, improving posture and reducing stress on your thoracic spine, shoulders, and neck.
Set up
Step into a relaxed standing stance and place your feet hip-width apart. With your shoulders resting on your hips, you should be standing with appropriate alignment. See yourself as having your spine lengthened by an opening pulling you upward.
Motion
Put pressure on your shoulder blades. Keep your posture for five seconds. You can imagine that you are trying to hold a pencil in the space created by your shoulder blades.
Advice
Verify that the muscles in your shoulder blades are the cause of the movement.
Surgery on the Shoulders
Subacromial decompression surgery for supraspinatus tendinitis
Even in cases where a full-thickness tear occurs in the tendon, less than 25% of patients with supraspinatus tendonitis will need surgery. However, shoulder surgery might be advised if, despite three to six months of conservative treatment, the symptoms of supraspinatus tendonitis have not improved.
This usually occurs when combined with other conditions such as subacromial bursitis, bone spurs, and/or rotator cuff tears in addition to supraspinatus tendonitis.
The most popular procedure to create more subacromial space is subacromial decompression surgery, which is often paired with rotator cuff repair in cases where the supraspinatus tendon is torn.
Different Diagnosis
While supraspinatus tendonitis is one of the most common shoulder complaints, painful arc syndrome can also be caused by other conditions that present similarly. Among them are:
- Acromio clavicular Joint Injury
- Bicipital Tendinopathy
- Brachial Plexus injury
- Cervical Disc Injuries
- Cervical Discogenic Pain Syndrome
- Cervical Radiculopathy
- Cervical Spine Strains and Sprains injury
- Clavicular Injuries
- Degenerative factors such as osteoarthritic glenohumeral joint Infraspinatus Syndrome, cervical spine radiculopathy, and rotator cuff tears
- Infectious factors such as osteomyelitis and acute pyogenic arthritis
- Inflammatory conditions such as calcific tendinopathy, adhesive capsulitis, frozen shoulder, and gouty arthritis
- Sports Myofascial Pain
- Neoplastic causes Tumor metastasis
- Dislocation of the Shoulders
- Subacromial impingement
- Superior Labrum Lesions
- Traumatic fractures and dislocations of the swimmer’s shoulder
- Shoulder Impingement Syndrome
- Adhesive Subacromial Buritis
- Rotator Cuff Tear
- OA of the glenohumeral joint
- AC Calcific tendonitis and arthritis
These shoulder disorders may develop alone or combined with supraspinatus tendonitis.
Additional thorough tests, including MRIs and radionuclide imaging, can help narrow down the differential diagnoses. These tests could involve checking blood for inflammatory markers and abnormal blood biochemistry, as well as counting white blood cells.
Thickened, comparable rotator cuff tendons with elevated signal intensity on all pulse sequences are the hallmarks of rotator cuff tendinopathy on MRI. Partial-thickness tears can be identified on MRI by changes in fluid intensity filling an incomplete gap in the tendon on fat-suppressed T2-weighted sequences. Complete disruption of the tendon is shown by a region of high signal intensity on all pulse sequences on MRI.
What More Is Possible to Help?
Finding the ideal balance between resting to allow the tendon to heal and exercising to increase shoulder muscle strength and flexibility is important when dealing with supraspinatus tendonitis. The following are the most effective exercises for supraspinatus tendonitis:
- Exercises for Scapular Stabilization: improves scapular control
- Rotator cuff Exercises: strengthens the shoulders
- Stretches for the shoulders: reduce muscle tension
- Stretches for the upper back: reduce stiffness and pain
- Additionally, good posture can have an important effect.
Two of the most common signs of supraspinatus tendonitis are tenderness when applying pressure to the tendon and a painful arc caused by shoulder abduction. If these symptoms are absent, supraspinatus tendonitis is unlikely to be the cause. For assistance with diagnosing the cause of your shoulder pain, see the section on diagnosis.
Risk factors
- Age: Because the tendons naturally decrease and weaken with age, there is an increased risk of supraspinatus tendonitis.
- Activities involving repeated overhead motions: Individuals who perform repetitive overhead motions, like painters, athletes who throw the ball overhead (e.g., baseball pitchers, tennis players), and construction workers, are more at risk.
- Weakness in the muscles: The tendons are at greater injury risk when the rotator cuff muscles are weak.
- Bad posture: Crouching over or slouching can cause the tendons in your shoulder to become compressed.
- Past shoulder injury: A dislocation or fracture in the past can raise the possibility of developing tendonitis in the future.
- Some medical conditions: Rheumatoid arthritis and diabetes, for example, can weaken tendons and increase their reactivity to inflammation.
Precaution
- Maintain good posture: This helps to keep your shoulder joint aligned and reduces stress on the tendons.
- Warm up before exercising: Spend some time doing light cardio and gentle stretches to stretch up your shoulder muscles before beginning any exercise that requires overhead motions.
- Strengthen your rotator cuff muscles: Develop the muscles related to your shoulder joint by doing regular rotator cuff exercises. This will help to maintain the tendons and improve stability.
- Use proper form: To prevent placing excessive pressure on your shoulders, use proper form when engaging in activities like weightlifting or throwing that require overhead motions. You can learn proper techniques with the help of a qualified trainer or physical therapist.
- Take breaks: Take frequent breaks to stretch and rest your shoulders if you perform repetitive overhead motions at work.
- Posture Work: to help expand the subacromial space and improve posture
- Pay attention to your body. If you feel any shoulder pain, stop what you’re doing and take some time to relax. Ignoring pain might result in more harm.
Complication
While supraspinatus tendonitis only poses no threat to life, delaying treatment can result in complications that can greatly affect daily living and shoulder function. If supraspinatus tendonitis is left untreated, the following adverse effects could arise:
- Rotator cuff tear: The tendon may become inflamed and degenerate over time, resulting in a tear. This may result in severe shoulder pain, weakness, and trouble moving the shoulder.
- Adhesive capsulitis (frozen shoulder): The condition known as adhesive capsulitis, or frozen shoulder, causes the capsule that surrounds the shoulder joint to thicken and tighten, thereby limiting the range of motion. It can be destroying and extremely painful.
- Bursitis: Inflammation of the bursa, a fluid-filled sac that cushions the tendons near the shoulder joint, can occur alongside tendonitis. This may make the discomfort and pain more serious.
- Loss of function: If tendonitis remains untreated, the shoulder’s strength and range of motion may gradually decrease, making it more difficult to perform everyday activities.
Conclusion
While supraspinatus tendonitis is not life-threatening, if left untreated, it can have a major adverse effect on your day-to-day activities. A common cause of shoulder pain in athletes who play overhead sports (baseball, handball, volleyball, tennis) is supraspinatus tendinopathy. The supraspinatus tendon affects the acromion as it travels between the acromion and the humeral head, which is the most common cause of this tendinopathy. The primary symptoms associated with this injury are pain and a reduction in strength, functioning, and range of motion; these should be addressed during physical therapy. There is sufficient data for conclusions that physical interventions, including extracorporeal shock wave therapy, cryotherapy, transcutaneous electrical nerve stimulation, ultrasound, and heat, are helpful in the recovery process for supraspinatus tendinopathy. However, it’s important to keep in mind that these techniques should only be used in addition to physical therapy (i.e., ROM expansion, rotator cuff strength training, and other shoulder stabilizers).
- Effective diagnosis and treatment are important to achieving a complete recovery and preventing possible complications.
- The likelihood of developing the condition can be decreased by being aware of the risk factors and by following preventive measures like strengthening exercises and good posture.
- Seek immediate medical attention from an experienced professional for a diagnosis and suitable treatment if you suffer from any shoulder pain, especially when performing overhead activities.
FAQs
How long does the healing process take for supraspinatus tendinosis?
It could take anything from a few weeks to four weeks for the condition to fully heal and recover; until then, it is not recommended to resume regular activities. If you perform severe overhead tasks at work or participate in sports, it can take an additional two weeks.
Is tendinopathy of supraspinatus serious?
Tendinosis may result in a rotator cuff tear. Partial or total tendon failure may be caused by internal tendon injury and a gradual weakening of the tendon fibers. This is uncommon before the age of forty years old, but as people age, it becomes more typical.
What specific test is required for tendinitis of the supraspinatus?
The supraspinatus can be isolated using the empty can test, also known as the Jobe test, by having the patient rotate the upper body so that their thumbs point to the floor. Next, in order to replicate emptying a can, resistance is given when the arms are in a 30° forward flexion and 90° abduction posture.
When you have supraspinatus tendinitis, which workouts should you avoid?
Pressing or overhead motions should be avoided in the beginning for those who have shoulder diseases. Forget about exercises like ball throwing or gym-specific weight training like pulldowns and overhead presses.
Where does discomfort from supraspinatus occur?
discomfort in the front and top of your shoulder that gets worse when you lift something heavy. At first, the discomfort only occurs when you’re doing anything, but eventually, it will also hurt when you’re resting your shoulder.
Is the tendoninosis supraspinatus a tear?
The rotator cuff tendon that suffers injuries most frequently is the supraspinatus. A supraspinatus tear, also known as supraspinatus tendinitis, may be present if you have: Shoulder pain that develops from repetitive shoulder motion and becomes obvious when the shoulder is at rest.
Does massage help with tears in the supraspinatus?
The rotator cuff’s muscles and tendons receive more oxygen and nutrients when the area is better circulated, which is another benefit of massage therapy. Massage not only improves circulation and reduces inflammation, but it also reduces muscle tension in surrounding areas of the injured area.
When you have supraspinatus tendonitis, how do you sleep?
Your wounded shoulder won’t be compressed or forced into an uncomfortable posture if you lie on your back. When the symptoms are at their worst, during the first few days or weeks, try sleeping in a chair or on a wedge pillow. You can prevent rolling over onto your side or stomach when you sleep by sleeping on a small incline.
When you have supraspinatus tendinitis, what is the ideal sleeping position?
The Best Sleeping Positions to Reduce Shoulder Pain
Having a back sleep
This provides proper anatomical support and reduces the strain on the bursae, muscles, ligaments, and joint structures by raising the ball and socket joint of the shoulder. According to recent research, adopting this sleeping position can help reduce shoulder pain and encourage deeper, more peaceful sleep
What is the quickest way for shoulder tendonitis to heal?
Many people discover that these straightforward, nonsurgical remedies greatly enhance their function and pain:
Changes in activity.
anti-inflammatory drugs.
injection of corticosteroids into the shoulder joint.
providing heat or ice to the shoulder joint.
Physical therapy and range-of-motion exercises
For the supraspinatus, what is poor posture?
How Does Shoulder Impingement Occur Due to Poor Posture? The subacromial space, located near the top of the shoulder bone, is where the supraspinatus tendon passes. When you slouch, curve your shoulders, or hunch over, this gap gets smaller, making less room for the supraspinatus tendon.
How is mild supraspinatus tendinopathy treated?
Tendinopathies are a very common issue in the field of musculoskeletal medicine. The passive modalities of rest, cryotherapy, nonsteroidal anti-inflammatory medications, and bracing make up conventional conservative therapies.
References
- Supraspinatus Tendonitis: Causes, Symptoms & Treatment. (n.d.). Shoulder-Pain-Explained.com. https://www.shoulder-pain-explained.com/supraspinatus-tendonitis.html
- Supraspinatus Tendonitis – Causes & Best Treatment Options in 2024. (2023, December 16). ProHealth Prolotherapy Clinic. https://prohealthclinic.co.uk/blog/supraspinatus-tendonitis/
- Exercises for Shoulder Flexibility: Pendulum Exercise. (n.d.). Saint Luke’s Health System. https://www.saintlukeskc.org/health-library/exercises-shoulder-flexibility-pendulum-exercise
- Pt, B. S. (2023, January 16). Isometric Shoulder Exercises. Verywell Health. https://www.verywellhealth.com/isometric-shoulder-exercises-2696516





One Comment