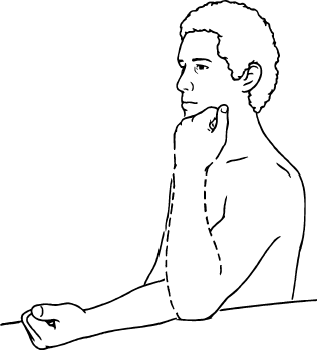
Ankle Range of motion exercise is a great way to improve the movement of the Ankle and It can be Active, Passive, or active assisted range of motion exercise.
The exercise mentioned here is meant to enhance the ankle joint range of motion. The arrangement of the bone surfaces inside a joint, the joint capsule, ligaments, tendons, and the muscles that work on the joint all have an impact on this movement.
There are three main types of exercises to improve ankle range of motion.
Passive range of motion
Active assisted range of motion
Active range of motion
How do we assess an ankle’s range of motion?
In order to measure an angle from the joint’s axis, both devices make use of a stationary arm, protractor, fulcrum, and movement arm. Additionally, the lumbar range of motion and other particular body areas can be measured with tape measures.
Normal range of the ankle joint
0 to 20 degrees of ankle dorsiflexion
0 to 50 degrees of ankle plantarflexion
0 to 20 degrees for ankle inversion
Ankle eversion is 0 to 10 degrees.
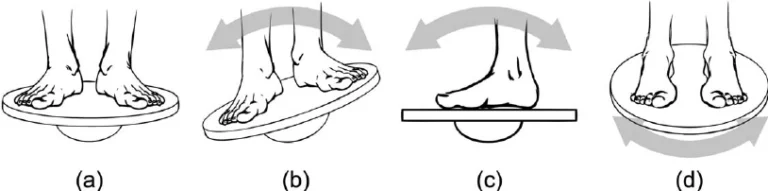
Passive Ankle range of motion exercise
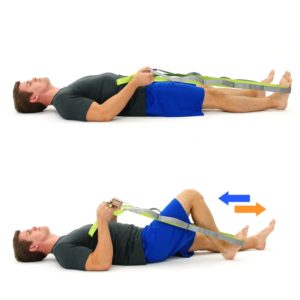
Using a stretched strap as a tool is one method of doing this. This will help the patient maintain a stretch for a longer amount of time, but practicing passive range-of-motion exercises with the help of a therapist is more beneficial. This kind of exercise aims to increase muscle flexibility by having a skilled practitioner both move and hold the body into the stretch.
This is better in a few ways. First of all, the therapist is aware of appropriate boundaries and knows when to go. The therapist is also aware of how long to hold the stretch. In order to attain maximum results, physical therapists are also educated to determine whether they are focusing on the right regions. Keeping that in consideration.
Exercises involving passive range of motion (PROM) are commonly employed in situations including paralysis, comatose patients, mending fractures, or pain that is triggered by active muscular contraction. Combating the negative consequences of immobility is one of the main objectives of ankle passive range of motion exercise (PROM), however, it’s crucial to keep in mind that PROM cannot stop muscle atrophy.
Advantages
In addition to supporting healthy joint functionality, this kind of exercise helps the patient by lowering pain, accelerating healing, preserving, and regaining range of motion (ROM) in some injured joints.
Passive range of motion exercises
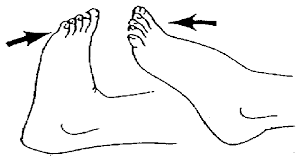
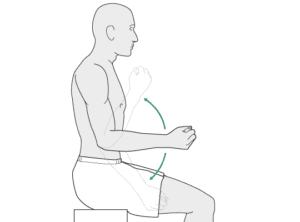
Passive plantarflexion
Passive plantarflexion
The patient should first be instructed by the therapist to assume a comfortable position, such as resting on the bed with a straight knee and their foot propped up off the bed. The physical therapist next uses a gentle pushdown to turn the foot such that the toes point outward from the body. Work out three times a day.
Passive inversion
Ask the patient to first assume a comfortable position, such as resting on the bed with their foot propped up and their knee straight. In one session, complete this exercise ten times. Work out for a period of time a day.
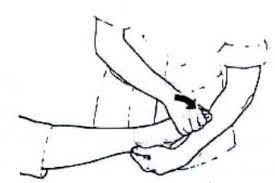
Passive eversion
Passive eversion
Initially, the patient should be instructed by the therapist to assume a comfortable position, such as resting on the bed with a straight knee and their foot elevated off the bed. Subsequently, the therapist slowly rotates the foot outward while preventing the leg from rotating. Ten times during the session, complete this exercise. Work out three times a day.
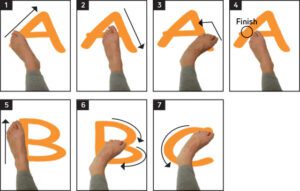
Alphabet
They should only move their foot and ankles. When performing this exercise, try not to move your knee or even your hip excessively.
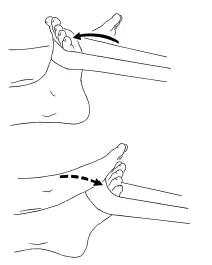
Passive ankle dorsiflexion
Passive ankle dorsiflexion
Next, slide the foot toward the face side by pulling back on the towel as the therapist holds each end in their hands.
Passive toe extension
The patient then places one hand on the heel and the other on the toes, moving the toes as far up towards the tibia’s shin as is comfortable.
Passive toe flexion
Passive toe flexion
The therapist instructs the patient to start by sitting in a chair and placing the foot that needs to be exercised across the knee of the opposite side. The patient next places one hand on each toe and the bottom of the heel, extending the toes as far as is comfortable towards the tibia’s shin.
Passive toe extension against the step
Next, slightly lean against the wall while applying pressure to the toes and pressing them back toward the tibia’s shin, but do not maintain this position. Do three sessions of this workout each day, ten times a session.
Active-assisted Ankle range of motion exercises
These exercises, as their name implies, entail the patient or the therapist providing some assistance. The majority of the action is performed by the patient, but in order to finish it correctly, some assistance is given.
The majority of the action is performed by the patient, but in order to finish it correctly, some assistance is given. The majority of the time, this limited range of motion is the time, this limited range of motion is the consequence of pain or weakness caused by bumps, bruises, falls, or even more serious injuries. When first practicing these exercises, the patient may experience severe pain and weakness. However, with time, there is a good chance that the patient’s range of motion around the ankle joint will gradually and permanently improve.
Advantages
Improve the ankle joint’s range of motion.
Increase the effectiveness of your movements.
Increase self-reliance.
Eases the pain in the ankles.
Enhance and preserve joint integrity.
Active-assisted range of motion exercises
Active-assisted dorsiflexion
First, instruct the patient to lie in a comfortable position, such as a straight kneeling position on the bed with their foot propped up off the bed. If the patient is unable to move their foot in between movements, the therapist will help them achieve full dorsiflexion. Do three sessions of this workout in a single day, or ten times in a single session.
Active-assisted plantarflexion
Ask the patient to get into a comfortable posture before starting, such as resting on the bed with their foot propped up and their knee straight. If the patient is unable to move their foot between movements, the physical therapist will help them attain their complete plantarflexion range. Do three sessions of this workout each day, ten times a session.
Active-assisted inversion
Active-assisted inversion
This can be as simple as lying on the bed with their foot propped up and their knee straight. Following that, the patient is instructed by the physical therapist to move their foot inward as far as they are able to. If the patient is unable to move their foot inward between movements, the therapist helps them achieve the complete range of inversion. Do three sessions of this workout each day, ten times a session.
Active-assisted eversion
Instruct the patient to lie down in a comfortable posture, such as on the bed with their foot propped up and their knee straight. The patient is then instructed by the therapist to extend their foot as far as they are able to. If the patient is unable to extend their foot during the action, the physical therapist helps them achieve their full range of eversion. Do three sessions in a day, ten repetitions of this exercise per session.
Active assisted toe flexion
Subsequently, the therapist lays one hand on the tips of the toes and the other on the bottom of the foot. If the patient is unable to bend their toes during this exercise, the therapist will help them achieve full toe flexion.
Active-assisted toe extension
Active-assisted toe extension
Ask the patient to first assume a comfortable position, such as resting on the bed with their foot propped up and their knee straight. Subsequently, the therapist directs the patient to move their toes upward, meaning as close to their face as possible. If the patient is unable to extend their toes between movements, the physical therapist assists the patient in achieving a complete range of toe extension.
Active Ankle range of motion exercises
Since the patient is fully capable of performing these exercises, the patient performs them most of the time. This can be painful, uncomfortable, or even hindering, but it is most helpful in cases of small injuries like an ankle sprain that do not significantly limit the ankle’s range of motion.
Active range of motion exercises
Toe extension
Toe extension
Plantar fasciitis, a condition that causes pain in the heel when walking and trouble lifting the toes, can be prevented or treated using toe extension exercises. The affected foot should then be placed on the healthy thigh. For 30 seconds, hold. Perform three rounds in a session.
Active dorsiflexion range of motion exercise
ankle dorsiflexion and plantar flexion exercises
Ask the patient to settle into a comfortable posture, such as reclining on the bed, before starting. The patient should next be instructed by the physical therapist to bend their foot toward their face, or upward, for as long as they are able to. The hold would not be taken at the terminus. Ten times a session, repeat. Work out three times a day. Increase the amount of repetitions from 10 to 15 or 20 in a single session as your muscles get stronger.
Active plantar flexion range of motion exercise
The patient should next be instructed by the therapist to move their foot away from their body, meaning that they should go as far as they can without being held at the end. Work out three times a day. Increase the amount of repetitions from ten to fifteen or twenty every session as your muscles get stronger.
Active ankle inversion range of motion exercise
First, instruct the patient to lie down on the bed or find a comfortable position. The patient should then be instructed by the physical therapist to move their foot inside for as long as they can, but at the conclusion, they shouldn’t be placed on hold. Work out three times a day. Increase the amount of repetitions from ten to fifteen to twenty every session as the muscles get stronger.
Active ankle eversion range of motion exercise
First, instruct the patient to lie down on the bed or find a comfortable position. The patient should then be instructed by the therapist to move their foot outside for as long as they can, but at the conclusion, they shouldn’t be put in hold. Ten repetitions per set, per session. Work out three times a day. Increase the amount of repetitions from 10 to 15 to 20 in a single session as your muscles get stronger.
Alphabet
Alphabet
Practice writing in both uppercase and lowercase letters, and remember to move from the ankle rather than the hip joint. Repeat ten times in a single session, but don’t stop at the finish. Perform three sessions per day.
FAQs
Which kind of support is ideal for weak ankles?
Ultimately switching to ankle support that is semi-rigid. The Aryse stability ankle system is a wonderful solution for preventing ankle sprains.
What illness results in ankle weakness?
Ankle weakness can also result from a few medical disorders. The most prevalent ones are osteoarthritis and diabetes. Lastly, wearing inappropriate footwear like high heels or unsupportive shoes is another factor.
What is the standard for ankle mobility?
Your ankle is flexible and has excellent dorsiflexion if you can back up five inches or more away from the wall. Work on ankle mobility if you are less than three inches, or if there’s a big discrepancy between the two sides.
How is the range of motion in the ankle measured?
As an alternative, the rater can measure ankle dorsiflexion range of motion (ROM) with an inclinometer by simply identifying the base of the fifth metatarsal in a non-weight-bearing posture or the tibial tuberosity for consistent inclinometer placement in a weight-bearing position1,6,8.
How is ankle mobility tested?
Dorsiflexion In The Ankle Forever and Ever Now, calculate the maximum distance the planted foot can travel from the wall without the rear heel coming off the ground.
What does limited ankle range of motion mean?
What is ankle equines, or ankle motion restriction? The ability to move the top of the foot toward the front of the leg is limited in people with ankle equines. You can have an equinus in one or both feet.
What degree of dorsiflexion is typical?
Dorsiflexion: Pain and range-of-motion workouts Dorsiflexion measuring more than 12.5 cm is regarded as typical functioning.
How may one become more dorsiflexed?
Ankle dorsiflexion can and will be improved by focusing on strengthening and toning the gastrocnemius and soleus muscles of the calf. Stretching, soft tissue massage, ultrasound, heat, cupping, and instrument-assisted soft tissue mobilization are a few of the often-used techniques for this.
What governs the movement of the ankle?
Ankle muscles Your ankle movements are controlled by the muscles in your legs and feet. Among them is the: Gastrocnemius muscle.
Is it possible to treat ankle weakness?
persistent instability in the ankle In addition, it results in edema, prolonged ankle pain, and a shaky ankle sensation. When nonsurgical measures fail to alleviate severe instability, surgery becomes the next best option.
What is an ankle’s normal range of motion?
For typical walking, one needs a range of 24° to 30° combined motion (dorsiflexion and plantar flexion), 37° for climbing stairs, and 55° for descending steps.
References
Prajapati, N. (2022a, May 3). Ankle Range of motion exercise: Active, Active assisted, Passive exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/ankle-range-of-motion-exercise/
Low-Level Laser Therapy (LLLT), also known as cold laser therapy or photobiomodulation, is a therapeutic technique that employs low-power lasers or light-emitting diodes (LEDs) to treat various conditions.
LLLT’s (low-level laser treatment) objectives are to decrease inflammation and speed healing by applying low-level lasers to the layers of skin or bruises. It is beneficial for disorders like lymphoedema and complicated wounds that don’t respond to conventional therapies.
An applicable wavelength of sunlight diminishes during minimally invasive light-based laser treatment (LLLT). It doesn’t generate any heat, vibration, or sound. Biological stimulation or photobiology are other names for it. The cells that make up connective tissue, known as fibroblasts, are thought to be affected by the activity of low-level laser therapy, which also has anti-inflammatory qualities and speeds up the healing process.
Light may penetrate hard and soft tissues, especially the skin, between 660 and 905 nm.
Class III lasers are referred to as LLLTs, or low-power lasers, whereas class IV lasers in the USA are known as High Power Laser Therapies (HPLTs), lasers with an output power of 500 mW or higher. Heat is generated on the outermost layer of the skin by HPLTs because of their higher power density (the illumination). As LLLT therapy doesn’t result in a heating tactile sensation, they are commonly called “Cold Lasers.”
Mechanism of low-level laser therapy:
The mechanism underlying LLLT is still being studied. It appears that the effects of LLLT are restricted to a particular range of laser wavelengths and that LLLT administered below the dosage range is ineffective. Photosynthetic reactions are well-studied in biology, and light-loving plants (LLLTs) make use of the Grotthuss-Draper law, which stipulates that a chemical reaction cannot take place unless a chemical component absorbs light. Consensus holds that the respiratory enzyme cytochrome c oxidase, which is part of the chain of electron transportation in mitochondria, is the chemical substance implicated in low-level laser therapy.
The adverse effects of low-level laser therapy:
Notable benefits of low-level laser therapy for physiotherapy include the following, and this instrument can be used to enhance other therapies like therapeutic exercise:
The lowering of inflammation:
Within hours or days, it can occur.
Alleviation of pain:
Faster tissue Regenerating: LLLT stimulates the development of endothelium, keratinocyte, lymphocyte, and fibroblast cells.
Effectiveness for difficult wounds:
In comparison to standard therapy alone, LLLT has been demonstrated to accelerate ulcer healing and reduce the need for amputations in individuals with diabetes.
Efficacy in treating lymphedema:
Research has demonstrated that lymphoedema patients, especially those whose lymphoedema is associated with breast cancer, can greatly reduce their arm volume and circumference with LLLT. The total number of patients in the study, meanwhile, can occasionally reach an upper limit, and the results can vary.
low-level laser therapy for regenerating your skin:
Low-level laser therapy (LLLT) has been associated with skin tissue exposure to red and near-infrared (NIR) light, whereas typical laser treatments such as ablation and cutting require powerful light. The electron transport system is then activated by an increase in reactive oxygen species (ROS), adenosine triphosphate (ATP), nitric oxide generation, and the activation of many signaling pathways.
LLLT has been utilized more frequently in recent years to treat psoriasis, inflammatory acne, scars, and fine wrinkles. The stimulation of stem cells promotes tissue healing and repair. The main advantage of LLLT for the skin is the lack of side effects or the presence of very minor ones.
Paleness in specific body areas is a common sign of vitiligo, a disorder that changes the color of the skin. Patients experience skin that is patchy with white areas. Additionally, by preventing autoimmunity, this treatment also lessens depigmentation.
The use of LLLT to treat acne shows a lot of potential. Mechanistically, light—especially blue light—is absorbed by porphyrins made by Propionibacterium acnes as part of their regular metabolic process. This light consumption initiates several photochemical responses that have an antibacterial impact.
low-level laser treatment for hair growth:
On the epidermis, hair follicles (HF) are tunnel-shaped structures that go through repeated regenerative cycles. In this cycle, there are three phases here; anagen, catagen, and telogen. Rapid cell division characterizes the anagen stage. Apoptosis drives the telogen arrangement, sometimes referred to as the resting stage, which follows the catagen arrangement.
Through a change in the hair phase, LLLT reduces androgenetic alopecia (AGA) in both genders. Mechanically speaking, LLLT brings telogen HFs back into the anagen phase. By increasing the generation of antioxidants and reactive oxygen species, it could promote keratinocyte and fibroblast mitosis. The cytochrome c oxidase (COX) gene facilitates the previously listed processes and is in charge of absorbing low-intensity light.
Whenever LLLT and functioning anagen cycle HFs are connected, cell division grows faster and the stage of anagen widens. It is known that exposure to lasers restores the physiological regeneration of hair follicles (HFs) on the scalp. These HFs may have been affected by chemotherapy-induced cancer medicines that cause alopecia areata (AA), AGA, and hair misfortune.
The findings indicate that scalp hair loss was reduced and hair thickness and diameter were increased during the LLLT-modulated hair period. Furthermore, LLLT has been demonstrated in multiple studies to lower inflammation, which is what initiates hair growth.
In general, LLLT improves alopecia patients’ clinical condition. AGA can be safely and effectively treated with LLLT, as multiple clinical studies have demonstrated. Significantly, individuals with non-scarring alopecias and those who did not respond to conventional hair loss therapies were found to benefit from this treatment.
How might low-level laser therapy work in conjunction with gradual hair loss?
First off, LLLT makes use of a light source that emits a certain wavelength (usually between 630 and 670 nanometers) with a unique capacity to absorb the chemicals found in hair follicles. This kind of light permeates the scalp and activates the epidermal stem cells that are in charge of hair follicle regeneration. In summary, DHT accumulation in the follicles is inhibited by LLLT because it promotes the metabolic activities required for hair production.
afterwards Treatment
Depending on your health, the number of alternative therapies you are receiving, the extent of your hair loss, and other factors, the success of laser hair therapy varies widely from person to person. The first noticeable effects of LLLT hair loss treatment become apparent in the second month following treatment initiation.
The results of the therapies become clear after the first four to six discussions. The sessions are held once a week. There are twenty-four sessions in a whole therapy cycle. The outcomes of the LLLT can be sustained for a long time with home maintenance after the entire course of treatment is finished.
Potential Advantages of Low-Level Laser Therapy:
Research and clinical trials on low-level laser therapy point to several advantages, such as:
Promotes detoxification and eliminates fat that could encourage weight loss:
Low-level laser treatment causes the fat inside fat cells to soften and become damaged, which makes it easier for the body’s lymphatic drainage system to start removing the fat from those areas.
At Restoration Healthcare, an Irvine functional medicine center, we reset the body’s metabolism for long-term health advantages by using low-level laser therapy as part of a medically supervised detox, fat-reduction, and/or weight-loss plan.
Reduces pain (analgesic):
Below are several ways that low-level laser therapy reduces pain:
reduces the sensitivity of nerves
lessens inflammation
increases the brain’s and the adrenal glands’ synthesis of endorphins, enkephalins, and opioids, among other painkilling substances.
Non-invasively stimulates acupuncture and muscle trigger points to release tensed muscle fibers.
Reduces inflammation:
By widening blood vessels and stimulating the lymphatic system, low-level laser therapy helps swollen areas caused by inflammation or trauma to drain.
Accelerates tissue healing and cell proliferation:
Deep tissue penetration of low-intensity light increases cell energy availability and speeds up cell growth and reproduction. By raising the synthesis of adenosine triphosphate (ADP), it promotes cell nourishment and waste removal, which is particularly useful in the regeneration of tendons, ligaments, and muscles.
LLLT is particularly useful in healing burns and open wounds because it also promotes the growth of fibroblasts in injured tissue. Fibroblasts are the key proteins needed to replace old tissue or repair tissue injuries.
Improves vascular activity:
Two methods that low-level laser therapy lessens scarring and expedites the healing process are by:
promotes the formation of new capillaries in damaged tissue at a much faster pace and widens and dilates blood vessels to increase blood flow to those areas.
Boosts metabolic activity:
In addition to promoting the synthesis of particular pro-healing enzymes in blood cells, low-level laser therapy also enhances the transportation of nutrients and oxygen.
Reduces the production of scar tissue: Surgery, wounds, scratches, and burns all cause fibrous (scar) tissue to form less frequently when low-level laser therapy is used.
Promotes nerve function and regrowth:
Axon growth and nerve cell reunion are accelerated by low-level laser therapy.
Supports immune system function:
By increasing the synthesis of lymphocytes and immunoglobulins and by making it easier for white blood cells to enter injured tissue, low-level laser therapy directly influences immunological function.
Lessens dependency on drugs:
Low-level laser therapy is thought to be a secure, organic, and efficient substitute therapy that can assist in lowering or doing away with the need for opioids other analgesics, and anti-inflammatories, alongside other drugs having unfavorable side effects that could be dangerous.
Uses for Low-Level Laser Therapy:
There are several uses for low-level laser therapy, such as the following:
Detoxification, fat loss, and weight management: Low-level laser therapy, such as the protocol now offered at Restoration Healthcare, can help the body get rid of extra fat that may be causing dysfunction or long-term illness when used as a complementary component of an integrative plan of care.
Musculoskeletal injuries and pain: Tendonitis, bursitis, tennis elbow, neck discomfort, lower back pain, knee pain, muscular spasms, and joint swelling are examples of musculoskeletal ailments and pain.
swelling: Examples of swelling include dental swelling, carpal tunnel syndrome, and autoimmune swelling (from a condition known as rheumatoid arthritis, for instance).
Skin rejuvenation: it includes treating edema (swelling), dermatitis, vitiligo, burns, psoriasis, and rashes.
Wound healing: For injuries that don’t respond to therapy, such as diabetes-related injuries.
Acupuncture: For patients who are uncomfortable with needles, consider acupuncture.
The limitations of low-level laser therapy:
Eyes: Wear the proper safety glasses for everyone in the room, and avoid pointing laser beams directly into people’s eyes.
Cancer: Unless the patient is receiving chemotherapy and LLLT can be used to lessen side effects such as mucositis, do not treat over the site of any known primary carcinoma or subsequent metastasis.
Pregnancy: Avoid applying direct treatment to the growing fetus.
Epileptics: Be advised that individuals who are photosensitive and/or epileptic may experience seizures in response to low-frequency pulsed visible light (<30Hz). According to reports, patients who received placebo devices in trials had the same negative effects from LLLT.
Low-Level Laser Therapy’s minor side effects:
Abnormalities associated with LLLT are quite rare. Early on in the course of treatment, a few months after starting LaserComb, some patients had a transient case of telogen effluvium. However, after using LaserComb consistently, this issue went away.
There have been instances where LLLT in the skin developed a slight redness that disappeared on its own without further treatment. Some patients treated skin became somewhat pigmented, swollen, and itchy. Patients may have blisters, burns, or scars on the treated skin if laser treatments are not done properly.
Evidence
2017 saw the publication of a comprehensive study and meta-analysis that determined LLLT to be a successful therapeutic approach for reducing pain in adult muscular and skeletal disorders individuals. Likewise, it was established that implementing the correct dosage requirements provided by the World Association of Laser Therapy (WALT) strengthened productivity.
Inconsistent data about the effectiveness of laser therapy for treating acute or chronic neck pain or shoulder discomfort were discovered in a 2017 study titled “A systematic overview of current evidence addressing effective treatment options for musculoskeletal pain in primary care.” Low-level laser therapy may be used in conjunction with physical therapy and/or surgery to treat knee discomfort.
FAQs
What does low-level laser treatment aim to achieve?
In photobiomodulation therapy (PBMT), also known as low-level laser therapy (LLLT), red or near-infrared (NIR) light is utilized to regenerate, recover, and stimulate different biological systems as well as to fix effects caused by injury or illness.
What is the low-level laser therapy success rate?
Participants in a clinically controlled study reported a 39% increase in hair growth, leading the researchers to conclude that low-level laser therapy considerably increased the number of hairs. Numerous further studies have confirmed that the laser cap is a secure and reliable method for enhancing both men’s and women’s hair growth.
What drawbacks does LLLT have?
For treatments, patients frequently need to see their doctors two or four times a week at the latest. After treatments, old injuries may get worse for a few days, but for most patients, this feeling only lasts for a few days.
References
Low-level laser therapy. (2024, April 12). Wikipedia. https://en.wikipedia.org/wiki/Low-level_laser_therapy
Low-Level Light Therapy for Hair Growth and Skin Rejuvenation. (2024, January 31). News-Medical. https://www.news-medical.net/health/Low-Level-Light-Therapy-for-Hair-Growth-and-Skin-Rejuvenation.aspx
Low-level laser therapy (LLLT): What are the benefits? | Top Doctors. (2023, December 18). Top Doctors. https://www.topdoctors.co.uk/medical-articles/low-level-laser-therapy-lllt-what-are-the-benefits
Top 10 Health Benefits of Low-level Laser Therapy. (2024, May 28). Functional Medicine Doctor Irvine. https://rhealthc.com/low-level-laser-therapy/top-10-health-benefits-of-low-level-laser-therapy/
Best Low Light Laser Therapy in Chennai | Laser Therapy in Chennai | Laser Hair Removal in Chennai | Laser Hair Removal Treatment in Chennai | Skin Laser Treatment in Chennai | Skin Lightening Treatment in Chennai | Skin Lightening Treatment Cost in Chennai | Laser Treatment for Facial Hair Removal in Chennai. (n.d.). https://www.radianceskinandhaircare.com/home/low-light-laser-therapy.html
Rehabilitation is a comprehensive, multi-disciplinary approach designed to help individuals recover from physical injuries, illnesses, or surgeries and improve their functional abilities and quality of life.
There is a great deal of worry about rehabilitation worldwide. Additionally, according to current data, 2.41 billion people globally, or one in three people, require rehabilitation assistance throughout their condition or injury, live with circumstances that affect their activities in daily routine and would benefit from rehabilitation services.
In the next thirty years, the percentage of adults over 60 overall will double, and the majority of them will have chronic illnesses, especially non-communicable ones. These shifting health and demographic trends are contributing to the recent global increase in the number of individuals engaging in a reduction in daily functioning, which has led to a significant unmet need for rehabilitation. The most vulnerable and underprivileged individuals in low- and middle-income nations as well as areas affected by violence bear the brunt of these unmet needs, and they are typically ill-prepared to handle these enlivening wants for rehabilitative support.
In other words, rehabilitation facilitates involvement in significant life responsibilities like family caregiving and helps a child, adult, or senior person be as independent as practicable in daily tasks. rehabilitation executes these activities through cooperating with the individual and their family to manage underlying medical issues and their symptoms, making adjustments to the environment to meet their needs better, utilizing assistive technology, providing education to improve self-management, and reworking tasks to be more safely and independently completed. When merged, these procedures should assist an individual in overpowering challenges related to assuming, noticing, listening, talking, swallowing, or moving.
Everyone must mandate rehabilitation at some point in their lives because of age-related lowering in functioning or as a significance of an injury, surgery, sickness, or illness.
What is Rehabilitation?
A set of interventions scheduled to accelerate functioning and underestimate disability among people with illnesses that appear in their environment” is the definition of rehabilitation.
The concept of rehabilitation is predicated on the premise that each person possesses the intrinsic ability and authorization to specialize in the medical field of their choice. This underlines the unequalness between acute care and restoration. Acute care is focused on a patient’s ability to survive. In contrast, rehabilitation teaches and trains patients to be capable of carrying out daily activities on their own, promoting self-care and active freedom.
Rehabilitation applied in a variety of ways depending on the situation. These include situations involving issues with human rights, evolution, disability, health, substance abuse, and security, to mention a few.
The WHO lists rehabilitation as one of the fundamental fitness methods, along with upgrading, deterrence, treatments, and restorative care. Rehabilitation is defined by the World Health Organization (WHO) as a class of phases that help patients who have disabilities or may develop them to reach and provide optimal functional activity to their specific circumstances.
Helping people heal, adapt, or reach their full potential on the physical, mental, and social levels is the aim of rehabilitation. It is an extensive procedure. It uses a multidisciplinary strategy incorporating supportive, therapeutic, and medical approaches. Health conditions can lead to injury, concussions, acute or chronic diseases, and other events including aging, stress, pregnancy, inborn defects, or inherited predispositions.
Rehabilitation may be necessary for anyone suffering from a medical condition that limits their ability to perform activities of daily living, such as their ability to see, move, or be alert. Therefore, applying the biopsychosocial approach to strategies addressing impairments, constraints on movement, and involvement concerning particular and environmental contextual elements, including assistive technology that impacts active functioning, adequately illustrates rehabilitation.
It is vital to recognize that rehabilitation is a therapy that is offered at every stage of the healthcare process. Many people who do not have long-term disabilities will eventually need aid with rehabilitation. Furthermore, Moreover, many individuals with chronic disability do not always need the benefits of rehabilitation. For instance, a person with a spinal cord injury (SCI) might need intensive rehabilitation in the months that follow their initial SCI. However, once their bodies have recovered enough to function at their best and have the assistive technology they need to enable them to resume performing well in their homes and communities, they might not need to access any further rehabilitation. Frequent rehabilitation must also be essential for certain individuals with long-term disabilities, such as those suffering from unhappiness or degenerative diseases.
Rehabilitation is a patient-centered health approach that manages the plans and purposes of the user as agreeably as the subsequent medical illness. At each phase of the fitness program, facts on functioning are necessary for finishing due to the purpose of rehabilitation is to maximize performance in the face of impairments, injuries, and acute and chronic illnesses:
Details on functioning principles, goal-setting, and product assessment at the user level throughout the primary, secondary, and tertiary stages of rehabilitative care, as well as in the therapeutic stages, User functional reports can be combined at the program level to improve clinical effect monitoring, service planning, and quality assurance. Gathering clinical data on functioning gives policymakers a foundation of evidence for allocating resources for fitness and rehabilitation and tracking their outcomes at the guideline level.
Rehabilitation arrives at every stage of life, from infancy to their golden years. It can occur before a health state (preventative “prehabilitation,” promotive), in acute care, post-acute care, and long-term care. A variety of health and non-health professionals, as well as individuals and their relatives, provide rehabilitation sessions.
Rehabilitative care puts the patient at the center of the course of action, enabling them to reach their full potential and engage in society more readily by reversing, restricting, or delaying neural, physical, intellectual, mental, cognitive, or social degradation. if rehabilitation is not done immediately it influences not just someone but also their relatives, residents, and the economy.
The rehabilitation stage comes after the preventive and curative stages of medical care.
Preventive medicine is the first phase where a disease is controlled from appearing by ignoring the relations between the agent, announcer, and environment. Curative medicine the second stage concentrates on trying to cure the disease. most doctors practice. curative medicine However there are numerous conditions like rheumatoid arthritis which has no cure and others like poliomyelitis in which the agent causing the disease has been removed from the person being treated, but side effects like paralysis exist; as a result, third phase rehabilitation is both medical and socially responsible is required.
Rehabilitation must be started by the earliest possible time to ensure the best upshot.it is administered in conjunction with specific medical or surgical treatment of the precipitating diseases.
Categories of Rehabilitation
Rehabilitation might be medical or socio-vocational. Medical rehabilitation is the process of using information from medical and paramedical to help rehabilitate a patient. diminish disability is the main objective of medical rehabilitation. Medical rehabilitation is followed by, or occasionally provided in conjunction with, socio-vocational rehabilitation. Socio-vocational rehabilitation’s goal is to reduce handicaps.
Medical Rehabilitation
Importance of physiatry
medical and socio-vocational rehabilitation is the responsibility of a team of professionals ruled by a physiatrist, the major person in the guidance of the rehabilitation program. These physiatrist experts work together and in teams to aid the disabled. the difference in the clinical evaluation by a physiatrist is that the physiatrist views the patient with experience in social and occupational areas in addition to a background in health He seeks to understand a person’s life as an illness has impacted it, what the person can no longer do, and how to overcome it.
A variety of healthcare professionals make up the rehabilitation workforce, such as occupational therapists, physiotherapists, speech therapists, audiologists, orthotists, prosthetists, clinical psychologists, physicians specializing in physical medicine and rehabilitation, and rehabilitation nurses. Countless other medical professionals, including general practitioners, surgeons, and community health workers, may also be crucial to a patient’s recovery.
The medical team members
Physiatrist
Physiatry also observed in some hospitals as physical remedy and rehabilitation has grown recently into a very wide and holistic area. There are very rare qualified physicians in the occupation of physiatry today. The physiatrist leads the rehabilitation team. The physiatrist’s duties include conducting a clinical assessment of the patient, making a functional diagnosis, and working with other team members to plan the patient’s course of treatment.
the physiatry or physical medicine expert is permitted in the observation of disability, prescription of physiotherapy, occupational therapy program, orthoses, and prostheses if needed. he often needs to involve the vocational counselor for vocational evaluation, counseling, training, job placement, or with the architect to design a barrier-free environment for the person with a disability. During his review, he would need to interact with his equivalents in another field like orthopedics or neurology. Academically, he has to focus on filling his area of expertise, producing some original work, coaching other team members, and taking notes whenever necessary.
The physiatrist is in the greatest position to help the patient and his family navigate the difficult recovery process. He considers his patient’s leftover ability. aligns them with his team’s expertise and lowers the patient’s ultimate disability.
the physiatrist must know sufficient enough in each of the paramedical, medical, and socio-vocational specialties relevant to rehabilitation to be able to provide the best possible course of therapy to the patient. he is seen as a friend, philosopher, and guide to his team members and patients. By qualities, a physiatry must be sympathetic, forgiving, and familiar. physiatrist must be capable of carrying out the best in his team and listen patiently to the individual thoughts.
Physical therapist
The physical therapist treats the patient with mobility rehabilitation. A vital member of the rehabilitation team is the physical therapist. He has to perform muscle strength evaluation quantification spasticity assessment, and measurement of the range of motion of a particular joint. the healing side he must execute exercises to maintain and accelerate a joint range of motion, train sitting and standing balance, or accelerate strength, endurance, and coordination for specific muscle groups or the complete body.
during treatment, the physical therapist must mix numerous therapy modalities such as heat and cold, as well as hydrotherapy techniques, electrical stimulation, traction, and massage for pain relief. For those confined to the home, he would visit them, and aid in-home evaluation to make the environment barrier-free and accessible. the use of various mobility aids including wheelchairs and their maintenance has to be taught to the patient. For those who are not ambulant, the physiotherapists do progressive gait training with or without ambulatory aids.
Occupational Therapist
An occupational therapist can assist you in setting objectives and overcoming obstacles on the social, mental, and physical levels. Along with providing you with the tools you need to feel comfortable and helped, they will collaborate with you to assist you in carrying out the tasks in your daily routine. The function of the occupational therapist is To optimize independence, it is his responsibility to assess the patient and provide training in self-care activities including consuming food, getting dressed, showering, and personal hygiene.
Throughout each stage of treatment, he would assist the patient in maintaining and improving their upper limb joint range of motion, muscle strength, endurance, and coordination. this aids the patient in exploring interests in hobbies and career abilities. Therefore, when a job change is anticipated, the occupational therapist and the vocational counselor must collaborate.
occupational therapists must offer comprehensive training in home management skills to people who are specified in their homes, utilizing basic self-help tools to reduce tiredness and preserve energy. The occupational therapist would assess the house, make recommendations for changes to create a barrier-free environment, and teach the patient compensatory skills to make up for sensory and perceptual deficiencies while taking cultural and social preferences into account. When appropriate, he would teach the patient how to use self-help aids, adaptive equipment, or orthoses. He would also instruct the patient’s family by demonstrating strategies meant to preserve the patient’s freedom and reduce overprotection.
in upper limb amputees and severely handicapped patients, he trains the functional use of a prosthesis or the environmental control system and collaborates with the physiotherapist in achieving set aims by utilizing activities instead of motion and with the orthotist in creating splints.
Prosthetist-orthotist
the creation, construction, and adjustment of the brace or orthosis are done by the prosthetist and orthotist, and prosthetic limbs made of plastic are utilized to replace lost limbs and to restore or provide function. A prosthetist makes them, and they are fitted specifically for each patient. The replacement must work and look as close to the original organ as manageable. to observe. the group member who uses a workshop to create the prosthetic called a prosthetist, upon the prescription by the physiatrist. Instructions on how to maintain the prosthesis are given to the patient and his family.
To determine the optimum appliance to be delivered, psychologists consult with the biomedical engineer, physiatrist, physiotherapist, and occupational therapist. Before delivering the appliance, he takes measurements, fabricates it, and makes sure it fits the patient making modifications and changes in design where required. When it’s completed, he aligns it both statically and dynamically with the patient and fixes it as necessary. He frequently collaborates with the biomedical engineer to ensure the detection of prosthesis shapes and layouts.
Rehabilitation Nurse
the rehabilitation nurse maintains the health of bedridden patients and helps them reach short and long-term goals She takes care of their nursing needs during hospitalization and in the rehabilitation ward In some cases she makes house visits and looks after the self-care activities of the hospital. She is responsible for:
Transfer to and from the bed, wheelchair, chair, couch
environmental elements like radiation, vibration, and sanitization, in addition to managing human hygiene and safety
the usage and care of adaptive tools mandated by the patient to communicate, eat, move, urine, dress, ambulate
exact preventative measures to underestimate the consequences of laziness and boost freedom
integrating various therapies into his daily activities
medication and followup
Speech Pathologist
When the patient is discussing and consuming, the speech pathologist provides support by:
evaluation and treatment of neurological communication problems
vocal reeducation
preoperative counseling before laryngectomy, glossectomy, and other procedures that will potentially influence communication abilities
Throat speech or using a prosthetic larynx are examples of laryngeal speech activity.
retraining speech inpatients with intra-oral defects
cognitive retraining
readying the patient in the usage of interaction devices
patient and family education
assessment of swallowing ability
treatment of dysphagia (trouble swallowing)
Psychologist and child development specialist
The psychologist provides training to the patient and their family members so they may completely participate in rehabilitation. psychologist conducts tests dealing with personality, and style, and studies the patient’s way of dealing with stress. The patient’s remembrance, cleverness, and problem-solving mastery should also estimated by the psychologist. Any psychiatrist or neurologist has interpreted the provisional diagnosis and therapy initiates. psychologists then initiate sessions in counseling. he would be needed to counsel adolescents to adjust to body changes as age advances, job aspirants to develop problem-solving skills, and alcoholics to get out of their habit. Empathy must be shown when it comes to marriage, sexual counseling, and managing the disability itself, which can lead to feelings of inadequacy or sorrow.
Horticultural therapist
trees and plants soothe the mind. Growing decorative plants, veggies, and flowers is said to offer therapeutic benefits for boosting self-esteem and confidence. horticultural therapists give mentally retarded as well as physically disabled children and adults, the opportunity to work with a variety of plants and thus promoting independence, motor skills, psychological well-being. Patients who exhibit ability and skill, those who are mobile, and those who may be in good physical health but have abnormal mental health are typically the ones chosen for treatment.
A music therapist
music must bring a person to the elevation of happiness.
The person with a handicap can act vocally or instrumentally as part of the music therapist’s action, or he may be assisted in appreciating music or going to performances. For adults or children with cerebral palsy or other paralyzing conditions, this is quite beneficial. While dancing or working out to music (a form of creative movement therapy) is a creative method to enhance gross motor milestones, performing an instrument like the violin or keyboard promotes fine motor skills. Music can be used to soothe, calm, or reduce discomfort or anxiety. For singers, it additionally assists with articulation training or rhythmic tone, which can enhance speech quality.
Certain patients are prepared for professions in music therapy through music therapy, including exceptionally gifted individuals and those whose disabilities increase their musical abilities, such as the visually impaired. Socialization skills, self-assurance, and self-esteem are enhanced by group music activities. It offers comforting care to patients and a much-needed vacation from their treatment.
Creative activity therapist
Play therapy and dance therapy are used with mentally ill patients more frequently than with physically impaired individuals. The goal of a dance therapist, also known as a movement therapist to employ rhythmic bodily movement as a psychological and physical tool to:
enhance your gross motor skills
reduce stress and enhance bodily tension awareness, emotional expression, and communication particularly when verbal expression is limited.
accelerate one’s physical awareness and perceptions
categorize and explain motions of the body
enhance gathering exercise and competitiveness
Recreational therapist
Utilizing recreational activities, recreational therapists help patients develop and enhance their social and emotional conduct.
the first step is estimating in detail the patient’s interests, social capacity, cognitive and inspirational functioning, level of orientation, and awareness. Physical limitations and abilities, resources, and perceived barriers in his immediate environment, also will help plan out his recreational activities next, the therapist goes about educating patients in leisure activities, with specialized equipment, adapted sports and alternatives to existing lifestyle, acquiring new skills. this is particularly beneficial to kids who would much rather play a game of cricket than receive physical therapy.
recreational activities like outings, experience journeys, picnics, contests, and dramatics have numerous benefits. they help to increase attention span and concentration, maintain physical strength, and social skill motivation they assist in family and patient adjustment to disability and thus decrease unwanted behavior, similar to depression. More than one may anticipate from awareness lectures, the much-needed community integration is provided by a group of special youngsters performing the role. Consequently, recreational therapy supports other therapeutic modalities.
play and recreation enhance functioning levels and thus improve the quality of life after discharge from the rehabilitation center.
Biomedical engineer
The field of rehabilitation acts as a link between engineering and medicine. and now have more advanced, user-friendly environmental control units, communication aids, orthoses, and limbs thanks to technological advancements. Professionals in computerized and electrical engineering must design apiece of artificial limbs. The function of a biomedical engineer is to collaborate with physicists, orthopedic surgeons, and speech pathologists to develop devices that will benefit those with disabilities. The design will frequently need to be special or tailored. Voice-activated wheelchairs, carbon fiber prostheses, and environment control systems are a few examples of technology used for the disabled.
Sociovocational Rehabilitation
A collaborative effort, socio-vocational rehabilitation seeks to give the disabled a job, a home free of obstacles, and the ideal social setting to lessen their handicap. The idea of having the freedom to work, regarding employment as a source of human dignity and a means of subsistence rather than just a means of surviving is the cornerstone of vocational rehabilitation. Consequently, it gives him a way to express his ambition and boosts his confidence as a self-sufficient member of society.
People are empowered not only financially but also more deeply and fundamentally. It causes an individual to stand upright. this empowerment releases people rather than linking them to a job. Not every person with a disability can stand upright, literally or otherwise. A more practical strategy is required. It is only natural to wonder why the disabled need to work in a nation like ours where even the physically fit cannot find employment. But we must never lose sight of the fact that every person has a constitutional right to self-realization through social integration.
The social worker works to raise community awareness of disabilities and their limitations while also trying to offer the patient and his family members emotional support. Sociovocational rehabilitation is also responsible for placing the patient in a job and training him for it, making sure he receives proper compensation. Professionals like the vocational evaluator and trainer are part of this collaborative effort.
A well-paying job is another duty of socio-vocational rehabilitation. Professionals like the vocational evaluator and trainer are part of this collaborative effort.
Employers should be incentivized to use the services of individuals with disabilities by offering awards of tax benefits and social distinctions India passed the PWD (people with disabilities) Act in 1995 The importance of the community cannot be overstated. Awareness campaigns must be launched, and self-belief must be fostered. The focus these days is on community-based rehabilitation, where qualified staff ideally from within the community are made accessible, even in distant locations, and are connected to primary healthcare facilities. Adults can receive training for a job that fits their neighborhood and surroundings. People with disabilities are pleading with people throughout the world to accept them for who they are.
In the current socioeconomic structure, people with disabilities are viewed as equal and productive members of society, and they have made unparalleled contributions to the fields of politics, business, science, and the arts.
Socio-vocational team member
Social worker
In socio-vocational rehabilitation, the social worker is a crucial element. This is a result of the interactions he must have with the patient, family, and rehabilitation staff. He plays a significant part:
Patient’s condition or handicap on the patient’s family, money, lifestyle, and community resources. Should the living circumstances require modification, he would propose a substitute
To determine the patient’s course of study or career, the psychiatrist’s conclusions, along with the patient’s talent, scholarly performance, attitudes, hobbies, and interests, are merged.
to describe the patient’s condition to the family and the course of therapy that has been recommended by the psychiatrist or psychologist.
Plan group activities with the family members to educate them on the patient’s sickness and care, and assist the patient and family in figuring out how to make a better social adjustment.
To support improved medical and mental health treatment, it is best to combine community resources whenever manageable for the patient’s benefit in the form of material or financial assistance.
give knowledge regarding the rehabilitation of all the staff of medico para medicos engineers etc.
Community contacts: The social worker uses audiovisual techniques, radio, television, press, and articles in journals to stay in touch with the community as part of public education.
To keep case files, registries, files, and communications for reference and research purposes in the future. A well-kept record frequently aids in statistical analysis and reveals some important details from the perspective of social research. It is also beneficial for long-term follow-up. assisting the patient with a suitable life partner or helping them find a career following training.
Vocational counselor
A vital member of the socio-vocational team, the vocational counselor helps patients choose the appropriate career path, set of skills, or lifestyle. The client is trained in a certain profession by a knowledgeable trainer.
Placement officer
He finds a suitable job for the impaired person and pays him frequent visits to work. He routinely works in coordination with the candidate, the company, the social worker, and the counselor. placement officer might be employed by an NGO or a government employment exchange. He keeps a database of candidate criteria and a list of potential clients, matching the two lists.
Special educator
A teacher who works with special children and tries to identify the deficiencies in their functioning is known as a special educator. They develop compensatory teaching strategies that allow for the accurate identification of the child’s faculties and create individualized programs based on the child’s strengths. Bad learning patterns can be broken and psychological, social, and mental development can be accelerated with early intervention. Because the needs are different, there is a greater focus on real-world experiences and vocational training rather than academic achievement.
Organizations that are non-governmental (NGOs)
The community recognizes this need and believes that the government alone should be in charge of providing care for the disabled. A group of benefactors collaborate to establish organizations that address the rehabilitation needs of individuals with disabilities.
Financial institutions and financing sources
They assist by providing funding to worthy candidates in exchange for concessional interest or the disclaimer of specific conditions and restrictions so they can open dealerships and companies.
Epidemiology of Rehabilitation
The Greek term epidemios, which means among the people in the 20th century, is where the word epidemiology originates. Epidemiology is “the science which considers infectious diseases, their course, spreading, and prevention,” according to Stallybross. Studying the origins of disease and preventative or treatment methods is known as epidemiology. The second option is containment if thorough isolation or complete preventive measures are not manageable.
Epidemiology, according to WH Welch, is the study of the natural history of diseases.
According to Lillienfeld, it is the study of how certain diseases or conditions are distributed among a community and the variables that affect that distribution.
Elements of Rehabilitation
Preventative Rehabilitation
prevention of disability does not initiate at birth, At the onset of diseases, or after primary disability occurs. Sometimes it may be done even before the child is born, by expecting disability due to genetic defects or blood group incompatibility and be prevented utilizing genetic counseling. For example, in DMD it is possible to counsel the parents on having another child who may subsequently exhibit the illnesses’ symptoms.
current population growth, particularly of the aged, naturally would result in a sharp rise in people with disability shortly.it is a paradox that because of the tremendous steps that medical Science has made the number of people who are surviving potentially deadly brain injuries is much more. it therefore follows that with a fall in mortality level, there is a rise in morbidity levels. Rehabilitation is a great part of medical and paramedical professionals’ care for persons with disability, and this gap keeps widening.
in recent years, specialists in neurology, orthopedic surgery, and pediatrics are increasingly getting involved with and have a vital role in rehabilitation medicine. this phenomenon shows the recognition and significance of rehabilitative medicine that other fields are placing on it.
unless more effective methods of prevention are developed to protect the population from primary disability in the future, the newly detected person with a disability will face a critical situation. Due to the progressive lack of health workers, they will not be able to access rehabilitation programs, and other disabilities will make them entirely dependent on society. this will result not only in personal sorrow, but will cause families, communities, and the country to face endless financial difficulties.
in the modern family in which both the husband and the wife do jobs, having a business to set the future. the presence of a disabled child or senior member would adopt this family of all its happiness, leisure, and time available. a lot of personal sacrifices will be required by each one of its members to take care of the patient. In the same way that they are now prepared to avoid communicable diseases, the medical community must take action to prevent outbreaks of incapacity.
level of prevention
Preventive health care refers to any medical intervention that aims to stop a patient’s decline on the health status scale and any effort to move it upward towards the peak, optimum health is called therapeutic health care. The World Health Organization divides this entire spectrum into three degrees of prevention.
primary prevention
it is explained as a measure taken before the onset of any diseases, vaccination against diseases that affect children, or adding chlorine to drinking water. The objective of this program is to improve the general state of wellness. To raise knowledge of health issues before they arise, it includes health education.
secondary prevention
it is a measure taken to avoid the progression of diseases while it is still in the early asymptomatic stage of the diseases. It comprises prompt diagnosis and treatment, for example, ergonomic intervention to keep a patient with spondylosis from experiencing clinical symptoms.
Tertiary prevention
it is explained as a measure taken to minimize the consequences of diseases or injury once it has become clinically manifested. e.g. preventing pressure sores in a paraplegic patient by frequently rolling them over an air bed. Rehabilitative medicine includes tertiary prevention as a fundamental component that occurs soon following the start of new deficits or a new diagnosis.
The goal is to preserve a person’s degree of ability by offering information, counsel, and actions that stop or delay the onset of new impairments. In long-term illnesses like cancer, diabetes, chronic obstructive pulmonary disease (COPD), and other neurological disorders, this is a typical type of rehabilitation.
Restorative Rehabilitation
To achieve the greatest possible recovery of function, restorative rehabilitation targets interventions that enhance impairments such as physical strength, respiratory function, and memory loss. To maximize function following surgery, illness, or acute events like serious trauma or stroke, this is a typical form of rehabilitation.
Supportive Rehabilitation
By teaching people compensatory techniques or alternate means of executing tasks, as well as by offering self-help gadgets, supportive rehabilitation improves a person’s capacity for self-care and mobility. This could involve changing the surroundings or giving helpful technology. This is also known as adaptive rehabilitation at times
Palliative Rehabilitation
Palliative rehabilitation respects the desires of individuals with life-limiting illnesses while enabling them to live a physically, mentally, and socially fulfilling life. To maximize functional independence and promote comfort, dignity, and quality of life, it frequently focuses on symptom relief, including pain, dyspnea, and edema; preventing contractures; breathing help, psychological well-being, relaxing, or using assistive devices.
The Principles of Rehabilitation
Principles regulate the application of rehabilitation measures. The rehabilitation specialist follows these guidelines when creating the treatment plan for individuals undergoing rehabilitation. every member of the rehabilitation team needs to be familiar with the rehabilitation principles for the process to have a meaningful impact. The following guidelines govern rehabilitation.
Encourage Modification
The physical, social, and emotional obstacles that come with limitations and the inability to perform one’s job are often too much for the patient to handle. To achieve the intended outcomes in rehabilitation, it is therefore essential to recognize the entire extent of the patient’s illness. This knowledge must be applied to support, enhance, and develop dedication and resourcefulness. therapy professionals also need to understand that, for many patients, optimizing work may be more important than full recovery as a goal of therapy. They must therefore be aware that rehabilitation helps patients tolerate difficult medical conditions rather than just “retrieve” from them.
People frequently misinterpret the word “regain” as meaning anything different from what a medical professional may supposed to do. Therefore, the use of “adaptation” may provide patients with a more natural direction to enable them to manage and put together changes to alterations that have occurred underlying a health condition or serious diseases that need lifelong modifications. Rehabilitation undoubtedly results in a reduction in mobility and restrictions as well as an increase in social participation and reintegration; nonetheless, giving patients a sense of adaptation boosts their self-esteem and helps them accept who they are and adjust to roles that are underlying health issues.
Highlight Your Skills
Rehabilitation emphasizes a positive outlook for individuals who have encountered a range of health obstacles that have resulted in situations that have changed their lives. Rehabilitation, therefore, focuses on what may be saved and obtained through corresponding goal-setting between the individual and the rehabilitation specialist rather than what has been lost.
Attend to the Overall Person
A thorough strategy for treatment is a fundamental declaration of rehabilitation. At all times when a person is being treated, it must end, not the breakdown. As the rehabilitation team designs treatment plans, it is important to include an individual’s preferences, background, culture, religious views, social support, physical capabilities, developmental stages, and psychology.
Time
The impact of time on rehabilitation has been extensively studied, ranging from the ideal time to start rehabilitation to the time required for recovery to generate the greatest benefits. Rehab takes a significant amount of time. Early initiation of rehabilitation has been shown to improve motor function following stroke and spinal cord injury (SCI) and reduce the risk of readmission for some illnesses, such as chronic obstructive pulmonary disease (COPD).
Instruct
Rehabilitation isn’t a miracle treatment, and education plays a crucial role in every stage of the process by giving the patient and their support systems to a helpful grasp of what’s happening, setting realistic expectations, and creating SMART goals. Rehabilitation education encourages patient-centered care, assists individuals in taking ownership of their health, and permits the greatest level of mobility and involvement in rehabilitation ambitions.
Person-centered care
a method of providing care that consciously views patients, caregivers, families, and society as participants in and beneficiaries of tried-and-true health solutions that are organized following people’s overall needs rather than specific diseases and honor of significance. People-centered care even requires caretakers to be able to work as much as possible in a supportive work environment, and patients to have the knowledge and resources necessary to make decisions and take part in their monitoring. Compared to patient- and person-centered supervision, people-centered care is more all-encompassing, including clinical meetings as well as monitoring residents’ physical well-being and their significant influence on the development of health care and policy.
Who requires Rehabilitation?
People who have lost talents necessary for daily living are referred to rehabilitation. Among the most typical causes are:
Traumatic cases like motor vehicle accidents and injuries such as spinal cord damage from falls from vehicles and brain injury, fractures (broken bones) like segmental, spiral, transverse, and burns
a stroke
burns formation
poliomyelitis
muscular dystrophy and peripheral nerve injury
pulmonary and cardiac rehabilitation
severe infections
extensive surgery
adverse reactions to medical treatments, including cancer therapies
What happens during Rehabilitation?
During rehabilitation, you are frequently assisted by a multidisciplinary team of medical professionals. Together with each other you and your spouse will determine your needs, objectives, and treatment strategy. The following types of therapy are all possible to include in a treatment strategy:
The objects, tools, and equipment known as assistive devices help people with impairments move and do daily tasks.
Relearning or improving cognitive skills like remembering, reasoning, learning, scheduling, and making decisions can be helped by cognitive rehabilitation therapy.
counseling for mental health
Using art therapy or music to express your emotions, think better, and form social bonds
nutritional advice
vocational therapy should support the patient with everyday duties.
To increase strength, range of motion, and general health, consider getting physiotherapy.
enhancing mental health through recreational therapy that incorporates games, relaxation methods, arts and crafts, and animal-assisted therapy
Pain management
vocational rehabilitation to assist in acquiring the skills necessary for employment or education
Depending on your circumstances, you may receive therapy at a hospital, an inpatient rehabilitation center, or the providers’ offices. A provider might occasionally visit your house. You will require family members or friends to assist with your recovery if you receive care at home.
examples of rehabilitation
Following are a few examples of rehabilitation:
enhancing communication following a brain injury through language and voice instruction.
Regular exercise can help patients with Parkinson’s disease or stroke improve their muscle strength, voluntary motions, and balance.
altering an elderly person’s living space to increase their sense of safety, independence, and fall prevention.
teaching the patient with heart disease safe exercise techniques.
constructing, fitting, and adjusting a prosthetic device as well as preparing an amputee to utilize it.
post-burn surgery, arranging the body posture and splinting methods to support skin healing, minimize edema, and reform mobility.
giving prescription to a child with cerebral palsy to diminish their rigidity.
Rehabilitation is very person-centered, which means that every individual’s objectives and preferences are taken into consideration while choosing interventions. Rehabilitation services can be provided in a variety of locations, including community settings like a person’s home, place of employment, an academic setting, as well as outpatient or inpatient healthcare centers, physical therapy clinics, and occupational therapy offices.
Programs for rehabilitation address the following areas:
The patient must be capable of carrying out ADLs, activities of daily living, and other self-care tasks.
Services for Rehabilitation: Bathroom usage, clothing, consuming food, getting ready, showering, and sexual activities
Physical attention: requirements for nutrition, medicine, and skincare
Assistance for families: Help with discharge preparation, money worries, and lifestyle adjustments
counseling in psychology: recognizing defects with thinking, behavior, and emotions and coming up with solutions
Analgesic medicines: complementary techniques for pain control
Career education: Job-related talent
Socialization techniques: Having conversations with people at home and in the community
Mental abilities: Skills related to organization, problem-solving, memory, focus, and judgment
Communication abilities: Speaking, writing, and other forms of communication
respiratory treatment: If a ventilator is required, lung function-promoting breathing exercises and therapies
mobility abilities: Wheel walking, transfers, and self-propulsion
Education: Information on the disease, medical treatment, and adaptive strategies given to patients and their families
What are the types of Rehabilitation?
Musculoskeletal and Orthopaedic Rehabilitation
Knee pain: Restoring musculoskeletal restrictions and relieving pain from injury, illness, or surgery are the goals of this restorative healing approach.
Following the patient’s requirements, objectives, and capabilities, the physical therapist develops a personalized therapy program. Physiotherapists use a variety of techniques to support joint and muscle function to improve, maintain, or restore physical strength, awareness, and flexibility with the best possible results. Numerous research concluded that patient and group training, as well as aerobic and strengthening exercises, are sufficient for patients with osteoarthritis in the knee (OA).
Neurological Rehabilitation
Various common conditions, such as multiple sclerosis (MS), Parkinson’s disease, stroke, spinal cord injury (SCI), and muscle defects, can cause varying degrees of symptoms, such as spasticity, poor coordination and balance, difficulty speaking and eating, and muscular defects. People suffering from neurological illnesses can exhibit remarkable promise for recovery in the early and late phases of rehabilitation following an injury. To speed up the healing process, new rehabilitation techniques can be applied either by themselves or in combination with pharmaceutical intervention. Rehabilitating activity following a stroke. for instance, requires practice that is reproduced and applies learning and brain alterations.
Rehabilitation may aid a patient who is struggling to perform daily duties by helping them come up with different ways to complete the same tasks or by using assistive technology. Physical therapy and occupational therapy can assist patients in increasing their range of motion and flexibility in their daily lives.
The burden of everyday care, domestic duties, eating, dressing, and bathing may be lessened with the help of functional methods and assistive technology. Helping patients deal with balance issues is the aim of vestibular rehabilitation. A few instruments have been created to improve stability. Fall prevention measures including bars, security drills, and technology that assists can help. All things considered, exercise can maintain function for people with medium to severe impairments and improve overall health and function.
Cardiac Rehabilitation
Patients with cardiovascular disease or those undergoing a myocardial infarction (MI) can benefit from cardiac rehabilitation, a complex intervention that includes health education, risk reduction recommendations, physical activity recommendations, and methods for managing stress. cardiac rehabilitation regimens are planned to manage cardiac signs, diminish the risk of unexpected death or myocardial infarction, determine the physiological and psychological significance of myocardial infarction, stabilize or counteract the atherosclerotic procedure, and improve patients’ emotional and professional situations. In addition to improving exercise capacity, quality of life, and psychological well-being, cardiac rehabilitation lowers mortality, morbidity, and unpredictable hospital hospitalizations. Apart from these benefits, most rehabilitation regimens include upper limb exercises and teaching breathing techniques, which reduce dyspnea.
Respiratory Care
Pulmonary rehabilitation aims to promote long-term monitoring of health-promoting practices while also enhancing the physical and mental well-being of people with chronic respiratory disorders. It is based on a thorough examination of the patient and is monitored by patient-specific treatments that may include but are not limited to, exercise training, education, and behavior modification.
For patients who have experienced a recent worsening, specialist pulmonary rehabilitation is given to improve their quality of life, respiratory function, and ability to do everyday activities. It has been demonstrated to significantly improve exercise capacity and health-related quality of life in individuals with Chronic Respiratory Pulmonary Disease (COPD) in conjunction with routine therapy. Research suggests that it helps those with moderate to severe COPD. The benefits of pulmonary rehabilitation have been established by individuals with COPD having better quality of life and increased functional exercise capacity.
Geriatric Rehabilitation
A decline in overall physiologic performance, which is a sign of aging, leads to chronic illnesses and increased multimorbidity in older persons. Knowing the fundamentals of rehabilitation will help provide senior human beings with beneficial restorative effects, as this and other factors make rescuing more challenging for them.
Habitual physical activity has been found to decrease the physiological impacts of an essentially sedentary routine and enhance the amount of time spent actively by changing the development and course of chronic disorders and immobilizing diseases, even though there is no option to completely stop the aging process. There is even emerging evidence that regular exercise by older persons has significant positive psychological and mental effects. Regular physical activity can improve muscle function, such as strength and power, and reduce the risk of chronic illness. It can also lengthen life expectancy and increase productivity. Exercise using multiple modalities has been shown to reduce fall rates. Home-based exercise and diet strategies have a positive impact on defect score and physical performance in pre-unstable/unsteady older persons, according to a randomized control experiment.
Rehabilitation of the kidneys
Renal rehabilitation has been demonstrated to sustain and in many cases improve renal function even though there is currently little proof to imply physical therapy improves the vital prognosis or renal impact. patients improve activity toleration and significantly enhance the quality of life related to physical activity in people with chronic kidney illness, both pre-dialysis and dialysis patients. Patients with chronic renal disease who had inadequate cardiopulmonary procedures, reduced exercise tolerance, and poor ventilatory efficiency benefited from intradialytic exercise programs. A 12-week/24-session renal rehabilitation exercise regimen has been found to improve physical capacity and quality of life in patients with Stages 3 and 4 chronic kidney disease. However, further research is needed to determine whether these findings translate into lower death rates.
Chronic renal disease-related secondary sarcopenia is linked to an increased risk of falls, mobility impairments, malnourishment, and osteoporosis. It has been suggested that using directed physical therapy to treat secondary sarcopenia in people with chronic renal disease can improve their quality of life by strengthening their bones and improving their cardiovascular health.
Rehabilitation for Burns
Many positive outcomes of burn healing have been reported. Virtual reality through the use of an Xbox Kinect 3D interface game increased exercise duration and patient satisfaction in patients with minor upper limb burns. For those with severe burn injuries, robotics in the form of robot-assisted gait activity has been shown to improve gait.
Not only has music therapy been shown to significantly lessen the pain, anxiety, and muscle strain that come with burn treatment sessions, but mental behavioral treatment and hypnosis have also been shown to help those who have suffered burn injuries feel less discomfort and anxiety.
What are the Aims of Rehabilitation?
Regaining your capacities and independence is the major purpose of rehabilitation. However, each person has distinct objectives. They vary depending on what caused the issue, whether it is a temporary or persistent cause, the abilities you lost, and the severity of the issue. As an explanation,
It may require therapy for a stroke victim to be able to dress or take a shower on their own.
After a heart attack, an active person may undertake cardiac rehabilitation to resume their exercise regimen.
Pulmonary rehabilitation is a treatment option for those with lung diseases who want to enhance their breathing and overall quality of life
handicapped individuals have problems with
orientation: a person with cerebral palsy or a head injury would find it difficult to get around and carry out daily tasks like eating or using bathroom facilities.
Physical freedom: every person with a disability hopes to become less dependent on those who look after them.
mobility: poliomyelitis and paraplegia are conditions that severely restrict mobility and thus even day-to-day tasks like moving around in the house can become very challenging
occupation integration: training and placement in a suitable job
Sociological connection: Since no man is an island, efforts should be taken to include and not exclude those with disabilities from society.
Financial independence: the position must guarantee a source of income
The Methodologies and Techniques of Rehabilitation
Physiotherapy
Physiotherapy treats disorders mostly related to bodily processes by using the body’s natural transformation mechanisms. Among the treatments they provide are:
Hand treatment
Physiotherapeutic movement treatment
Physical therapy including electrotherapy, thermotherapy, ultrasound therapy, and cryotherapy
Taping Massages (both traditional and introspective)
Occupational Therapy
Occupational therapy aims to retrain and train abilities and tasks that have either never been done before or have been lost due to disease or trauma. It focuses on enhancing the patient’s capacity for daily mobility independently by:
carrying out daily tasks (ADLs), such as cleaning, cooking, clothing, and personal hygiene.
Upper extremity rehabilitation. concentrating on several motor and sensitive aspects, such as proprioception, strength, endurance, dexterity, coordination, and sensitivity.
consultation regarding technical assistance and reinforcement tools to improve living standards at home.
Thalassotherapy, or ocean hydrotherapy
Seawater’s mechanical and thermal qualities are utilized in simple baths, contrast baths, and hydro kinesiotherapy physical activities in an aquatic setting. thalasso treatment can be administered in groups or one-on-one with a therapy assistant. The objective is to improve balance, motor coordination, muscle strength, and perception of one’s own body.
Heliotherapy: Sun Radiation as Light Therapy
Sun exposure, in particular, and light therapy are effective treatments for psoriasis. By exposing the affected area to sunlight, the skin cells’ development is postponed, potentially leading to better skin formation.
The psoriasis sufferers have been designed to provide the highest level of privacy possible. heliotherapy makes psoriasis sufferers possible for the patients to feel comfortable as sunlight is directly spread to the affected area. To prevent sunburn, it is imperative that sun exposure happen gradually and that enough sunscreen be applied to the parts of the skin unaffected by psoriasis.
Speech-language dysfunction
Speech therapists plan to conserve and improve their patient’s capacity to communicate and their capacity to consume food. Observing an examination of your mastery, the speech therapist would create a plan of care. Through instruction from our speech therapist, patients can improve their voice, swallowing, and speaking. Training that patients can do at home will be taught to them.
Treatment in a Multisensory Setting: Snoezelen
This multisensorial therapy chamber, inspired by the Snoezelen concept, offers multiple therapeutic modalities. Snoezelen recommends chilling or sitting comfortably in a soothing, warm space while enjoying the lighting effects and being surrounded by soothing music. Snoezelen is employed to encourage a better perception of sensation and relaxation.
Fragrant perfumes can fill the Snoezelen section, bringing back memories and stimulating dreams. The patient and the physiotherapist can focus on specific goals and communicate more easily in this relaxing environment. Additionally, improving the patient’s autonomy and quality of life, as well as developing modified ways, are the objectives.
intense functional and physical exercise, if necessary combined with the use of belts to reduce body weight. The objective is to retrain gait training and strengthen intralesional musculature in individuals suffering from acquired brain injury, spinal cord injury (SCI), and other diseases.
Extensive Extension
Exercises that stretch the muscles are especially beneficial for people with spasticity and immobility because they reduce the risk of injury and help regulate muscle shortening.
Training in a wheelchair: Strategy and health
Wheelchair users will improve their abilities and path with this group exercise. They train both inside and outside the clinic to learn how to navigate and overcome obstacles that arise in parks, homes, businesses, and other everyday settings. Wheelchair users will receive advice and recommendations from the therapist to help them become more independent and self-assured. To maintain health and increase strength, these programs also incorporate stretching and fitness exercises.
Seasonal Group Classes and Activities
The therapists in the team of the seasonal group have a wide range of educational and professional backgrounds. Every season they deliver special lessons where their patients can learn new skills that enable them to keep their minds and bodies engaged. In history, these contained:
MediYoga
Meditation
Creative Crafting
Afrodance
Health Education
These give their patients the chance to learn more about their conditions, get guidance, and talk about their experiences. These educational and social events allow patients to bring about new knowledge while staying corrected.
The Capacity and Scope of Rehabilitation
The vast majority of track patients are hidden by rehabilitation. It includes guidance on how to grasp basic communication skills, instruction on how to improve or maintain the highest possible standard of health, well-being, and career, and complex neurological rehabilitation after severe trauma or stroke. Depending on the patient’s need for modifications over their lifetime, rehabilitation may be appropriate at any age. Like, they might require resources to:
Learn New Skills: Children might require resources to learn new skills to overcome challenges brought on by developmental disorders and medical conditions and achieve the highest level of fitness and independence.
Healing from Serious Trauma: Reeducation and rehabilitation assist individuals in regaining and optimizing their abilities and self-sufficiency, including returning to work.
Manage Long-period Sickness: to help patients recover and optimize their freedom in activities of daily living, those with chronic or long-period illnesses who suddenly became unwell or worsened participate in rehabilitation sessions.
Manage oneself Conditions: Individuals with long-term or chronic conditions can take charge of their health and lower their chance of experiencing side effects that could negatively impact their mental or physical well-being. These side effects could include pain, anxiety, depression, contractures, loss of cardiovascular and strength fitness, and ulcers.
Allowed Advocating: As part of their rehabilitation sessions, those who are weak and in need of assistance, such as those with mental impairment and communication issues, are advised to participate in advocacy.
Maintain capabilities and Independence: Early diagnosis, evaluation, and rehabilitation intervention can help patients maintain their independence and abilities for as long as possible in the case of degenerative illnesses including dementia, motor neuron disease, and terminal cancer.
Improve Performance: After an injury or a period away from sports, rehabilitation will give athletes and sportspeople the chance to improve their performance.
Survival from Unexpected Conditions: These include heart attacks, pneumonia, anxiety, psychosis, urgent hospital admission after a stroke, surgery, and falls.
The Benefits of Rehabilitation
A wide range of medical conditions, including both acute and chronic illnesses, as well as damages, can be lessened with rehabilitation. It completes other health interventions, such as surgical and medical procedures, helping to promote recovery and get the best results possible. Rehabilitation can help regulate, lessen, or manage challenges related to a variety of medical conditions, such as spinal cord injury (SCI), stroke, or fractures.
Rehabilitation helps to mitigate or postpone the incapacitating effects of long-term medical conditions including diabetes, cancer, and cardiovascular disease by giving patients the tools they need to take care of themselves, manage their pain, and get the assistance they need. It thereby promotes aging healthfully.
Rehabilitation is a purchase that generates financial returns for the community and its residents. Reduction of hospital stay duration, avoidance of costly hospitalization, and management of re-admissions may be beneficial. Rehabilitation undervalues the need for financial or guardian assets because it makes it easier for people to participate in, return to, or remain apart from their jobs at home.
There are some major Proportions of Attention in the Rehabilitation Approach:
managing comorbid illnesses and medical problems through identification, control, and treatment.
scheduling for the most elevated level of space.
encouraging the patient’s and their family member’s best psychosocial coping and change.
preventing secondary disabilities by promoting reintegration into society, which includes maintaining ties to family, friends, leisure activities, and professional training.
enhancing the standard of living for those with residual disabilities.
preventing situations from recurring.
Physical Advantages
Boost Physical Abilities and Alleviate Pain
builds muscle
enhances equilibrium
lowers the chance of falls
make better flexibility and joint gestures and make better coordination
stop deformities and problems with the limbs
posture and gait are improved
Elimination of needless complexities
Psychological Benefits
increases self-assurance and capacity to handle illness or injury psychologically. gives you more autonomy and helps you regain your cognitive health level before the injury.
Lifestyle Advantages
Enhanced Involvement
Reduced dependence
the higher standard of living
Returning to work sooner can reduce financial difficulties and increase social interaction.
Encourages you to resume your sport or exercise so that your health and wellness awareness can benefit. When you can resume your sport or training at your previous level, you also improve your overall fitness.
Financial Gains
Within the framework of health and social care, rehabilitation interventions can offer protection in several ways. For example, it can
enable a patient to go back to work, find employment, and maintain employment while lowering the cost of nursing, residential, and social care
lessen the likelihood of falls
diminish the payments related to mental health illness and financially not sound
cut down on the price of diabetes care
lower the expense of staying longer
Results of Rehabilitation
The benefits and changes in a patient’s functioning over time that may be linked to a particular effort or set of criteria are known as rehabilitation outcomes.
There is also strong evidence that the benefits of rehabilitation can contribute to long-term cost savings as well as value and sameness across the healthcare process. They might include:
Reduction and Deterrence of Health Care Need
Including out-of-hospital treatment can shorten hospital stays and prevent unplanned admissions
Reduced Readmissions or Hospital Admissions
Reduced Duration of Stay
Greater autonomy and improved conditional self-management
The lessened amount of care required
Go back to a job or role that is appropriate for your age, gender, and situation (e.g. home care, school, work)
a higher standard of living
False Beliefs Regarding Rehabilitation
Rehabilitation is not limited to those with long-term, physical limitations or disabilities. Rather, rehabilitation should be available to everyone who needs it. since it is a vital health service for everyone who has an acute or chronic sickness, disability, or injury and chooses to work.
Rehabilitation is not an unnecessary medical service that is reserved for the wealthy. Additionally, trying to control or repair a health problem only after other options have failed is not voluntary aid. Rehab interventions that are prompt, high-quality, and affordable should be available to everyone to fully realize the benefits of rehabilitation on a social, economic, and health level. For people in general, this means continuing to offer rehabilitation in addition to other treatments from the moment a medical issue is reported.
Approximately 2.4 billion people on the planet today suffer from a medical condition that could benefit from rehabilitation. Population and demographic shifts are expected to result in a much greater desire for rehabilitation in the years to come. Individuals are living longer, and by 2050, it’s expected that there will be twice as many individuals over 60 as there are now. Additionally, more people are tortured with chronic illnesses like diabetes, strokes, and cancer. Concurrently, there is still a persistent rate of damage and developmental disorders in children (such as cerebral palsy). Rehabilitation may be helpful for these health issues because they are associated with higher levels of disability and can affect an individual’s functioning.
In multiple regions worldwide, the accelerated demand for rehabilitation is vastly unsatisfied. In a variety of low- and middle-income nations, about half of the population in need of rehabilitative therapy does not obtain it. Global rehabilitation demands are unfulfilled for several reasons, such as:
A shortage of national rehabilitation policies, and funding.
plans, and protracted wait periods for services related to rehabilitation outside of the cities.
high out-of-pocket costs and insufficient funding sources.
a shortage of qualified In many low- and middle-income settings.
there are fewer than 10 rehabilitation experts per million individuals, and there are also insufficient resources, such as equipment, consumables, and assistive technologies.
The requirement for additional rehabilitation-related data and research, as well as inadequate and underutilized referral routes to rehabilitation.
Rehabilitation in troubles
Hazards that are caused by humans, such as terrorism, industrial accidents, or natural disasters like earthquakes or disease outbreaks, can result in severe rehabilitation demands due to illness or injury. In addition, they concurrently cause disruptions to the current services and mostly affect the most vulnerable populations and the most breakable health systems.
Although clinical and humanitarian standards acknowledge the critical role that rehabilitation plays in disasters, rehabilitation is rarely taken into account when it comes to early detection and preparedness of the health system. As a result, individuals who are directly impacted run the risk of developing greater impairment and disability, pre-existing restrictions in rehabilitation services are exacerbated, and health service delivery is rendered less effectively
Conclusion
A crucial component of fitness that enhances independence and productivity is rehabilitation. Before arriving at its current approach, the health domain had multiple stages of development. This model comprises biological, sociological, and contextual components that impact the health and function of individuals experiencing various health conditions.
Getting the most out of function is the ultimate objective of rehabilitation, and it is vital to a patient’s health no matter the root cause of the medical condition, the replacement, the provider, or the environment in which it is conducted. Through the restoration, management, or postponing of functional decline in sensory, physical, intellectual, mental, cognitive, or social domains, rehabilitation prioritizes the patient and facilitates their attainment of maximum potential and community participation. As a result, it has an impact on families, communities, and economies in addition to the individuals themselves.
FAQs
When should one begin their rehabilitation?
Following an accident, the rehabilitation process has to begin as soon as possible and serve as an ongoing continuity alongside further therapeutic interventions. When an injury necessitates surgery, it can also begin before or right after surgery.
What is the rehabilitation’s shared objective?
A series of activities intended to maximize functionality and lessen handicaps in people with health issues during their interactions with their surroundings is known as rehabilitation.
What elements influence recovery?
The circumstances surrounding rehabilitation, from the situation before, during, and after the event allowing to a loss in function, are essential variables to keep in mind throughout the rehabilitation process because we know that the environment has a significant impact on treatment generally.
What constitutes the primary element of rehabilitation?
Every element of the rehabilitation regimen is designed to control and alleviate pain. Relieving or reducing physical pain and discomfort can significantly improve a person’s overall health and quality of life. elevating the quality of life for an incapable is the dream of rehabilitation.
Which patients mandate rehabilitation?
Individuals with degenerative diseases or depression, for example, may also require episodic rehabilitation therapies despite having long-term disabilities. Rehabilitation is a very person-centered approach to healthcare in which the user’s goals and preferences are taken into account in addition to the underlying medical issues.
How much time does healing from rehabilitation take?
phases involved in recovery. Depending on the severity of the injury, recovery time varies, for example, a moderate sprain or strain may heal in as little as one week, whereas a full ligament tear may require several months.
What does rehabilitation represent?
In India, rehabilitation science encompasses the following areas: Rehabilitation and physical medicine. This area of study addresses problems about the neurological, cardiovascular, and musculoskeletal systems in terms of prevention, diagnosis, and treatment.
What is the rehabilitation issue?
Rehabilitation problems are any number of obstacles or difficulties that people may run into whether they are recovering from an illness, accident, or surgery. Typical issues with rehabilitation include the following: Physical Restraints, Regaining physical strength, mobility, or coordination can be difficult.
What forms a foundation for rehabilitation?
The Fundamentals of Rehabilitation. The picture that each person is valuable and has the right to be in charge of their health is the cornerstone of rehabilitation. This theory leads to each person’s perspective as being a comprehensive, holistic, modern entity
Why is it necessary to have a rehab plan?
It’s critical to realize that adhering to an exercise regimen will help injuries heal better and more quickly. Rehabilitation programs strengthen and activate weakened or inactive muscle groups to support your body and assist prevent injuries and discomfort.
What possible disadvantages might rehabilitation have?
During recovery, the number of new medical issues decreased over time and was independent of the amount of time since the injury. accelerated tone, agitation/aggression, urinary tract infection, and sleep disturbance were the most often reported issues.
What comes last in the process of rehabilitation?
Regaining function unique to one’s sport and returning to play constitute the final stage of rehabilitation. Restoring balance and coordination, enhancing quickness and agility, and developing sport-specific abilities are all possible during this stage of injury recovery.
How are injuries rehabilitated?
Modalities including heat or cold therapy, electrical stimulation, ultrasound, or manual therapy methods like massage or joint mobilization can all be used in the rehabilitation process for injuries. These techniques are employed by physical therapists to control pain, lessen inflammation, and enhance tissue repair.
References
Rehabilitation. (2024b, April 22). https://www.who.int/news-room/fact-sheets/detail/rehabilitation
All three types of elbow joint range of motion movements are included in exercises that concentrate on passive, active, and active-assisted range of motion.
Types of elbow joint range-of-motion exercises
Passive range of motion exercise: The first type of exercise involves passive range-of-motion, wherein the elbow joint can only be manipulated by the user, by other people, or by a passive motion machine.
Active-assisted range of motion exercise
Active range of motion exercise
Movements of the elbow joint
Because it enables the hand to be moved into nearly any position, the elbow is crucial for performing a variety of tasks.
Flexion
Extension
Supination: Turning one’s hand and forearm such that the palm faces upward or forward
Pronation
Placement for the goniometer
Axis location: The lateral epicondyle
Stationary arm: positioned parallel to the humerus
Movement arm: in line with the radius
First, the patient should be instructed to straighten their elbow from its maximum flexion position. After that, the patient should be given a little pressure to check the elbow extension’s passive range of motion.
Exercise your elbow’s passive range of motion.
This is helpful for the elbow joint that has become immobile due to damage or even a paralysis attack of any kind. gently stretching the muscles and retraining the patient on how to move correctly. Here, a therapist stretches the elbow’s soft tissue to release tension and relax the nearby muscles. Exercises including passive range of motion for the elbow also help to reduce stiffness and rigidity in the immobilized elbow joint.
Elbow stretches that involve a passive range of motion are more effective when performed with a therapist nearby to help with the stretch. In order to increase muscle flexibility, the skilled practitioner does this kind of exercise by both moving and holding the upper arm in a stretched position. This is better in a few ways. First of all, the therapist is aware of appropriate boundaries and knows when to stop. Finally, in order to maximize benefits, a physical therapist is trained to determine whether they are targeting the right location. Keep it in consideration.
When a patient is unconscious, has a mending fracture, experiences an attack of paralysis, or experiences pain during an active muscular contraction, passive range of motion (PROM) exercises are usually employed for the elbow joint. However, it’s crucial to keep in mind that PROM exercises are unable to stop muscle atrophy.
Benefits the passive range of motionExercises
Exercises that promote the passive range of motion not only help the patient maintain healthy joint functionality but also reduce pain, speed up healing, restore and maintain range of motion in injured joints, increase muscle mass, improve blood flow, and raise oxygen levels.
A few suggestions for an elbow passive range of motion exercise
Maintain constant support for an arm’s weight.
Continue moving smoothly and slowly.
The physical therapist ought to limit their movements to what the elbow joint or muscle will allow.
Passive range of motion exercise
Passive elbow flexion in full supination
Passive elbow flexion in full supination
Subsequently, the therapist must gently slant their elbow and, if feasible, place their hand on the elbow. Ten times during a session, do it. Work out three times a day.
Passive elbow flexion in mid-pronation position
Next, if it is feasible, the physical therapist should gently bend from the elbow and make contact with the elbow with their hand. Repeat ten times in a single session. Work out three times a day.
Passive elbow flexion in full pronation position
A patient should be instructed to begin by a therapist once they have assumed a comfortable position, such as supine with their hands fully pronated. The next step for a physician is to gently bend from the elbow and, if at all feasible, have the hand touch the elbow. Ten times during a session, do it. Work out three times a day.
Passive elbow extension
Next, if it is feasible, a therapist should have the hand touch the elbow while gradually straightening the elbow.
Passive elbow supination
Passive elbow supination
The therapist should next take hold of the hand and shake it. Then, perform this drill ten times in a session. Work out three times a day.
Passive elbow pronation
The hand is then moved by the therapist into pronation, which is a supination position with the palm toward the floor.
The patient flexes their elbow passively
The patient flexes their elbow passively
The patient should be instructed to lie down in a comfortable position, such as supine, before beginning. Next, the patient should slowly bend from the elbow, if at all possible, letting the hand touch the elbow. Make an effort to flex your elbow to its maximum range of motion.
passive elbow extension on the other hand.
Subsequently, the patient has to gradually extend their elbow and, if feasible, make contact with it with their hand. Make an effort to extend your elbow to its maximum range of motion. Ten times during a session, do it. Work out three times a day.
Passive supination by the patient’s other hand
Passive supination by the patient’s other hand
Subsequently, the patient is instructed to gradually rotate their forearm outward or upward, ensuring that their hand is fully pronated from their elbow and touching it if feasible. Ten times during a session, do it. Work out three times a day.
Passive pronation by the patient’s other hand
The patient should next gradually rotate their forearm inward or downward so that their hand is facing the floor, fully supinated from the elbow, and, if at all feasible, touching the elbow.
Active-assisted range of motion exercise
As the name implies, the patient or the therapist may provide some assistance throughout these exercises. While the patient undertakes most of the work, little assistance is provided to ensure that the elbow motion is performed appropriately.
Most often, weakness or pain from falls, bruises, accidents, or even more serious injuries is the reason for this restricted elbow movement. When first practicing these exercises, a patient may experience severe pain and weakness, but with time, there is a good chance that their range of motion around the elbow joint will gradually and permanently improve.
Exercises for elbow active-assisted range of motion have several advantages.
improves the elbow joint’s range of motion.
Improve the effectiveness of motion.
Improve self-reliance.
lessen suffering.
Active-assisted range of motion exercise
Active-assisted elbow flexion
The patient should then be instructed to move their forearm to the face side, or behind their elbow, but once they stop, the therapist should aid them in completing the full range of elbow flexion. In one session, perform ten repetitions.
Active-assisted elbow flexion in mid pronation
The patient’s elbow or upper arm should then be supported by a therapist using one hand, while the other strong hand should be used to grasp the patient’s wrist or forearm. Once the patient has stopped doing this, the physician should assist the patient in completing the full range of elbow flexion. Ten reps should be done each session. Perform three sessions per day.
Active-assisted elbow flexion in the pronation position
Active-assisted elbow flexion in the pronation position
A patient should first be instructed by a physical therapist to assume a comfortable position, like sitting on a chair with their back supported. The patient’s elbow or upper arm should then be supported by a therapist using one hand, while the other strong hand should be used to grasp the patient’s wrist or forearm.
Subsequently, a physical therapist should instruct a patient to bend their elbow by moving their forearm towards their face; however, once the patient ceases the movement. Perform ten rounds in a session. Work out three times a day.
Active-assisted elbow extension
The patient should first be instructed by the physical therapist to settle into a comfortable chair with their elbows bent and their back supported. Next, a physical therapy professional should instruct a patient to straighten their elbow by moving their forearm from the face side to the floor side. Perform ten rounds in a session. Work out three times a day.
Active-assisted forearm supination
Initially, a physical therapist should instruct a patient to assume a comfortable posture, such as sitting on a chair with their back supported and their elbow fully extended to 90 degrees. Next, the medical professional should use one strong hand to support the patient’s elbow or upper arm and another strong hand to grip the patient’s wrist or forearm.
The patient should next be instructed to rotate their forearm outward such that their palm faces the ceiling. However, once the patient ceases this motion, the physical therapist should assist them in completing the full range of forearm supination. Perform ten rounds in a session.
Active-assisted forearm pronation
Active-assisted forearm pronation
Before beginning, the therapist should instruct the patient to assume a comfortable position, such as sitting with their back supported and their elbow fully supinated at a 90-degree angle. However, once the patient ceases this action, the therapist should aid them in completing the full range of forearm pronation. In one session, perform ten repetitions.
Actively assisting elbow flexion with the stick
Actively assisting elbow flexion
A patient should be instructed by a physical therapist to first assume a comfortable position, such as sitting with their back supported on a chair or table. The therapist should next instruct the patient to grip the stick’s end with both hands while supporting the patient’s elbow or upper arm with one hand and holding. Perform ten rounds in a session. Work out three times a day.
Elbow extension helped actively with a stick
The patient should first be instructed by the therapist to assume a relaxed position, such as sitting on a chair or even a table with their backs supported and their elbows fully extended. Next, a physical therapist should instruct a patient to grip the stick’s end with both hands while supporting the patient’s elbow or upper arm with one hand and holding their wrist or forearm with the other. The patient is then instructed by the doctor to straighten their elbow in order to move their forearm away from their face, using both a hand and a healthy elbow. In one session, perform ten repetitions.
Using one hand to actively help in forearm supination
Using one hand to actively help in forearm supination
The patient should first be instructed by the therapist to get into a comfortable position, like sitting, with their elbow fully extended and 90 degrees flexed. They should then grab the affected hand with their healthy hand. Work out three times a day.
using a different hand to actively assist forearm pronation
To begin, a physical therapist should instruct a patient to assume a comfortable position, such as sitting, with their elbow fully extended and supinated, and to hold their damaged hand with their uninjured hand. When the patient stops executing this action, the physical therapist assists in completing the full range of forearm pronation. Ten times during a session, do it. Work out three times a day.
Active range of motion exercises
Goals:
Increase your strength
Maintain or improve endurance
Promote circulation
Maintain or increase range of motion (ROM)
Active range of motion exercise
Active elbow flexion
First, instruct the patient to get into a comfortable position, such as sitting or standing. Perform ten rounds in a session. Work out three times a day.
Active elbow flexion in mid-supination position
First, instruct the patient to choose a comfortable position, preferably standing or sitting. Perform ten iterations in a single session.
Active elbow flexion in pronation
Active elbow flexion in pronation
Tell the patient to settle into a comfortable position before starting, like sitting or standing. Next, instruct the patient to move their forearm toward their face by bending their elbow, but do not keep this posture until the desired outcome has been achieved. In one session, perform ten repetitions.
Active elbow extension
First, instruct the patient to get into a comfortable position, such as sitting or standing. Subsequently, the therapist ought to instruct the patient to straighten their elbow, which entails moving their forearm away from their face, without holding them at the endpoint. In one session, perform ten repetitions. Work out three times a day.
Active forearm supination
Active forearm supination
First, instruct the patient to assume a comfortable posture, such as sitting or standing with their elbow slightly bent at a 90-degree angle. Ten times a session, do it. Work out three times a day.
Active forearm pronation
The therapist should first instruct the patient to settle into a comfortable position, such as sitting or standing with their elbows bent to a 90-degree angle. The patient should next be instructed by a therapist to turn their forearm inside so that their palm faces the floor.
FAQs
How can I extend the range of motion in my elbow?
Extension of the Elbow Goal: straighten elbow completely. After five to ten seconds, relax your elbow and repeat this stretch.
What does elbow extension mean?
For any task that demands raising the arm above the horizontal, as well as to attain a stable hold, elbow extension is essential.
What is a limited elbow range of motion?
Loss of elasticity in muscles, ligaments, tendons, or skin results in a contracture. There will be less room for you to bend or extend your elbow.
What does elbow ROM function for?
More elbow flexion and pronation are needed for modern tasks like typing and using a cell phone than for the functional motion arc.
How can I rotate my elbow more effectively?
Exercises for Pronation and Supination Active Supination and Pronation: Rotate your palm up and then slowly turn it down as far as it is comfortable to do so while keeping your elbow at your side and bent at a 90-degree angle.
How may elbow stiffness be decreased?
In certain cases, when conservative approaches prove ineffective or inappropriate, surgical relaxation of the stiff elbow may be the next step.
What is the elbow joint’s normal range of motion?
When it comes to elbow flexion-extension motion, healthy arms typically range from 6° to 11° for maximum extension and from 130° to 154° for maximum flexion.
Which four elbow motions are there?
We are able to do daily tasks because of the powerful muscles that span the elbow joint, which causes flexion, extension, supination, and pronation.
What is the elbow’s functional range of motion?
Elbow range of motion can be used for most daily activities, ranging from 75 to 120 flexion.
How can I get my elbow back to its full range of motion?
Here are a few elbow range-of-motion exercises that are frequently recommended: Elbow Extension and Flexion: To begin, take a seat or stand with your arm relaxed by your side. After a few seconds of holding this posture, progressively extend your arm.
References
Prajapati, N. (2022b, May 13). Elbow range of motion exercise -Active, Passive & Active assisted exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/elbow-range-of-motion-exercise/
The greatest flexibility exercise you can do at home to increase upper arm flexibility is the triceps stretch. Practicing at home is simple and should be done regularly with other flexibility exercises like the biceps stretch.
What is a Triceps stretch?
The triceps brachii muscles on the back of your arms are the focus of the triceps stretch. Stretching your triceps right can help you recover more quickly from a workout and ready your upper arm muscles for weightlifting and aerobic activities.
The advantages of doing triceps stretching:
Improve your flexibility and extend your arm’s range of motion.
Stretching your triceps can improve blood flow to your arm and lessen pain.
The health of your arms and shoulders is improved by doing triceps stretches.
A rotator cuff injury can be prevented by stretching your triceps muscles before performing upper body exercises.
It can stop connective tissue from becoming loose and muscles from becoming tight.
Triceps muscle stretching techniques:
Typical muscle stretching techniques include the following;
Overhead triceps stretch
You can do this stretch while sitting or while standing. This is the triceps muscles self-stretching.
Your shoulders should be raised to your ears and then pushed down and away from you.
Reach up to the ceiling with your left arm, then flex your elbow so that your left palm rests on the middle of your back.
Using your right hand, strongly press your elbow down and toward the center.
Hold this position for a few seconds.
Then return to your neutral position.
Then relax.
Repeat this process 3 to 5 times.
Overhead triceps stretch
Triceps towel stretch
You could use a towel or a strap, for example. Stretching should be done by opening your chest and using your core muscles.
It is initially necessary to start from standing.
With your left hand, grasp a towel now.
Reach up with your right hand to grasp the end of the towel, keeping the back of it against your back, while pushing your right elbow down on your side body.
Your hands should be spread apart at the palms.
Hold this position for a few seconds.
Then return to your neutral position.
Then relax.
Repeat this process 3 to 5 times.
Towel-stretch
Horizontal stretch
Flexibility is increased by this stretch. Both sitting and standing are suitable ways of doing it.
Using the hand opposite to your elbow, take one arm above your elbow and pull it across your body toward your chest until your shoulder stretches.
Remember to maintain your elbow below shoulder level.
Hold this position for a few seconds.
Then return to your neutral position.
Then relax.
Repeat this process 3 to 5 times.
triceps horizontal stretch
Leaning stretch
You’ll need a chair, couch, bench, or anything stable, to complete this stretch.
This item must be leaned against.
As much as you can, get on your knees away from the chair so that your body is parallel to the floor and you can lean forward without resting your head on it.
Take a seat with your elbows resting over your head.
Your lower back is not strained when you bend your elbows to support yourself.
Take a line of sight from your head, neck, and back to the ground.
Make sure that only your elbow touches the chair.
Put your hands on the back of your neck and move your forearms toward your neck.
Let go of the breath as you pull your upper body toward the floor.
After a few seconds of holding this stretch, turn around and go back to your kneeling position
Then relax.
Repeat this process 3 to 5 times.
triceps Leaning stretch
Triceps pull-down
When standing straight your feet should be shoulder-width apart.
The resistance band should be held in one end by your left hand.
Grasp the resistance band securely with your left hand, just below your shoulders.
Hold the opposing end of the resistance band in your right hand.
Raise this hand to your hip level.
Take a breath and keep your left hand pressed against your chest the entire time.
Push the band toward the floor with your right hand as you breathe in, extending your right arm to its maximum length.
Maintain your position while pulling the band as far as you can without jerking back.
After you release the pressure caused by the resistance band, slowly raise your right arm back to hip level.
Then relax.
Repeat this process 3 to 5 times.
Triceps pull-down
Overhead Triceps Wall Stretch
Lining up with a wall squarely.
As near to the wall as you can manage, push your elbow.
You will get more of a stretch the higher you go.
The elbow should be bent back and down, with the palm facing away from you.
Press down with the other hand on the outward-facing palm.
Feel the stretch by pressing your weight through your elbow into the wall.
Hold this position for a few seconds.
Then return to your neutral position.
Then relax.
Repeat this process 3 to 5 times.
Overhead Triceps Wall Stretch
Typical mistakes that you should stay away from when doing triceps stretch:
You’re not going low enough
Your arms won’t contract correctly if you’re not lowering yourself down to your body in the correct position. so be careful to properly lower yourself without touching the ground.
Maintaining an excessively wide elbow distance
Try to maintain elbow distances equal to shoulders. An injury may happen if it is closer or wider than that.
Using your legs to move yourself upward
The exercise uses your legs to target your upper body, which causes you to delay your results.
Exercise too quickly
Give your muscles time to rest.
There is improper arm locking
There’s less muscle stretching because your arms aren’t locking correctly.
Excessive weight addition
When doing triceps dips, some people weigh their legs. In case you’re a beginner, you should exercise care or refrain from using weight.
Lack to maintain proper foot alignment
Stretching requires you to maintain your balance.
Summary:
Spend some time stretching your triceps to improve your range of motion, strength, and flexibility. These quick and easy stretches are something you may add to your daily routine at any time.
Before starting an exercise regimen, especially if you have any health conditions that may be affected, speak with your doctor. Always stay within your limits and increase gradually. Both your daily life and athletic performance will get better over time.
FAQs
What is the target of the triceps stretch?
The triceps brachii muscles on the backs of your arms are the focus of triceps stretches, a type of arm stretch technique. Triceps stretches, when performed correctly, can help after your workout muscle recovery and prime your upper arm muscles for weightlifting and aerobic activities.
Triceps are good, but why?
Acting as an extensor of the elbow and shoulder, these muscles support and stabilize your shoulder joint. Strength and stability in your shoulders and elbows also increase with the strength and size of your triceps.
What are the advantages of triceps stretches for health?
Arm exercises that target the large muscles at the rear of your upper arms are called triceps exercises. Among other advantages, stretching regularly can help avoid injuries, improve range of motion, and avoid tight triceps. Along with stabilizing the shoulder, the triceps muscles help extend the elbow.
How do you use your triceps?
Your triceps play a major role in upper body movements. Stabilizing your shoulders and allowing you to push and pull is their important function. You contract your triceps each time you push a shopping cart, pull open a door, or lift a grocery bag.
Is it easy to train the triceps?
Building up your triceps doesn’t have to be difficult if you focus on progressive overload and select the best exercises. It’s necessary to pick triceps exercises that stretch the muscle’s long head and engage every angle of the strength curve.
Do sore triceps need to be stretched?
It can hurt to perform serious triceps exercises the day after an intense arm workout. As the soreness develops, it may become uncomfortable even for simple tasks like opening the refrigerator or getting out of a chair. One of the best things you can do for relaxing your aching triceps is to dedicate some time to triceps stretches.
References:
N. P. (2022, February 11) physiotherapist. Stretching your triceps: Type, Benefits to Health, How to Stretch? A mobile physical therapy clinic. Mobile Clinic for Physiotherapy. The benefits of triceps stretching exercises can be found at https://mobilephysiotherapyclinic.in/
2023a, July 20; Cronkleton, E . Eleven shoulder stretches that can help ease tightness. The website Healthline provides information on tight shoulders.
On December 20, 2022, CSCS, C. R. Four triceps stretches were demonstrated by a physical therapist to maintain a loose arm position. male health. Tricep stretches can be found at https://www.menshealth.com/fitness/a42287997
Image 3, April 23, 2023b; Colletta, M. How to Stretch Your Triceps Best Before and After a Workout. Additions of Steel. These are the best triceps stretches to do before and after working out, according to Steel Supplements’ blog.
Image 4, P. Fryer (2022b), May 30. wiki How Fitness offers 5 methods for stretching your triceps. Visit https://www.wikihow.fitness/Stretch-Your-Tecs.
Ilioinguinal neuralgia is a chronic pain condition that affects the ilioinguinal nerve, which runs from the lower abdomen through the groin. This nerve can become irritated or damaged due to various causes, such as surgery, trauma, or infection.
This nerve feels the lower abdomen and upper thighs by running across them. It can cause a burning, stabbing, or shooting pain in the groin, thigh, abdomen, or genital areas when it is squeezed, irritated, or injured.
Although not often recognized, this illness seriously negatively affects a person’s quality of life. Continue reading this article to learn more about ilioinguinal neuralgia’s symptoms, causes, and treatments.
What is an Ilioinguinal Nerve? Anatomy and its Function
The first lumbar nerve, which runs around the lower back, is the source of the ilioinguinal nerve. It branches out through the second and third abdominal muscles and communicates with the iliohypogastric nerve, which is mostly in charge of controlling the diaphragm, a breathing muscle, and the surrounding tissues.
The ilioinguinal nerve communicates with the upper thigh, pelvis, and anterior abdominal wall. It sends motor branches to the abdominal wall and aids in the sensory innervation of the genitalia and anteromedial thigh.
Anatomy
The ilioinguinal nerve arises from the lumbar plexus in the posterior abdomen. It is formed by the L1 spinal nerve’s anterior ramus, or division.
Following its origin, the nerve emerges from the lateral border of the psoas major muscle. Later, it travels inferolaterally and penetrates the abdominal wall around the anterior superior iliac spine.
The internal oblique and transversus abdominus receive motor branches from the ilioinguinal nerve, which travels through the anterior lateral abdominal wall.
Once it passes through the superficial inguinal ring and into the intestinal canal, it innervates the skin of the genitalia and anteromedial thigh.
Function
Motor Function
The ilioinguinal nerve supplies the transverse abdominus and internal oblique muscles of the anterior lateral abdominal wall.
These muscles can be contracted unilaterally to rotate the torso ipsilaterally, or bilaterally to compress the contents of the abdomen.
Sensory Function
The skin of the superior anteromedial thigh, which covers the medial portion of the femoral triangle, is innervated by the ilioinguinal nerve. It also has a role in genital sensation:
The male anterior scrotal skin.
The skin of the labia majora and mons pubis in women.
What is Ilioinguinal Neuralgia?
A medical condition known as ilioinguinal neuralgia is represented by compression or irritation of the ilioinguinal nerve, which results in pain and discomfort in the groin and lower abdomen. A person’s quality of life may be greatly impacted by this illness, which can cause persistent discomfort, restrictions on everyday activities, and occasionally anxiety or depression.
What causes the Ilioinguinal Neuralgia?
For ileoinguinal neuralgia, there is frequently no identifiable cause. However, a few things may be involved in ilioinguinal nerve irritation:
Compressed Nerve: Trauma from abdominal surgery, injuries, or inflammation in the surrounding area can cause the thin ilioinguinal nerve to become compressed. The nerve may be pinched by scar tissue or a hematoma from surgeries such as appendectomy, hernia surgery, or delivery.
Nerve Damage: The ilioinguinal nerve can sustain damage from blunt trauma, laceration wounds, or illnesses that affect the nerves. Nerve damage is linked to some conditions, including diabetes.
Referred Pain: Occasionally, pain comes from a different location, such as the pelvis or lower back. However, the pain pattern appears along the ilioinguinal nerve’s course.
Neuropathy: Nerves affected by generalized nerve illnesses such as neuropathy are more sensitive to defective signals, which can cause discomfort.
Chronic discomfort Conditions: Neuralgia is more common in people who have endometriosis, fibromyalgia, or persistent pelvic discomfort. The entire mechanism is unclear.
Infection: The ilioinguinal nerve may become inflamed in rare instances due to shingles, HIV, and syphilis.
What are the Symptoms of the Ilioinguinal Neuralgia?
The primary sign of ilioinguinal neuralgia is intense, intermittent pain that is primarily felt in the groin, thigh, and lower abdomen. It frequently happens on its own during unexpected episodes or may be caused by actions like bending, walking, or ascending stairs.
The upper thigh or the genitalia may experience radiating pain. Individuals suffering from ilioinguinal neuralgia characterize their pain as burning, piercing, or shooting. It might feel like an electrical surge of electricity.
The main symptom of ilioinguinal neuralgia is severe, sporadic pain, mainly in the lower abdomen, thigh, and groin. It often occurs spontaneously during unplanned episodes or may be caused by movements such as walking, bending, or climbing stairs.
Radiating pain may be felt in the genitalia or upper thigh. Individuals who suffer from ilioinguinal neuralgia characterize their pain as burning, piercing, or shooting. The feeling might have been like receiving an electrical shock.
What are the risk factors for Ilioinguinal Neuralgia?
Before getting a surgical procedure on the abdomen is the main risk factor. Procedures that injure or compress the ilioinguinal nerve include hernia repair, appendectomy, C-section, and hysterectomy.
The ilioinguinal nerve can also be harmed by abdominal trauma resulting from a fall, accident, or sports injury.
An increased risk of nerve damage, particularly injury to the ilioinguinal nerve, is associated with chronic disorders such as diabetes, shingles, and HIV.
The ilioinguinal nerve may get irritated due to the pregnancy’s tension on the abdominal wall. Over time, repetitive activities like riding a horse or cycling can irritate the ilioinguinal nerve.
Increased tension on the abdomen wall due to obesity may raise the possibility of nerve compression.
What are the Differential Diagnoses for Ilioinguinal Neuralgia?
Several medical conditions, such as an inguinal hernia, tumor, varicocele, hydrocele, spermatocele, temporary testicular or ovarian torsion, and myofascial damage, can cause pain in the groin area that resembles ilioinguinal entrapment.
What are the Diagnoses for Ilioinguinal Neuralgia?
Because ilioinguinal neuralgia’s symptoms might overlap with the symptoms of other illnesses, diagnosing it can be difficult. It is necessary to rule out alternative causes using clinical examination, imaging, and occasionally diagnostic nerve blocks to reach an appropriate diagnosis.
In your case, staying in constant contact with your physician aids in identifying the cause of the issue. Among the diagnostic tests that could be performed are:
Pain Locating: The process of identifying the source and characteristics of pain is called “pain locating.”
Imaging: Magnetic resonance imaging (MRI) or ultrasound to view the internal structure and rule out other possible reasons for the discomfort.
Nerve Blocks: Anesthetic is injected close to the ilioinguinal nerve to relieve momentary pain.
What are the treatments for Ilioinguinal Neuralgia?
Without appropriate care and management, ileoinguinal neuralgia will not go away. The goal is to alleviate nerve irritation that causes pain signals. When it comes to treatment, particularly conservative methods are always chosen first:
Medication: In many situations, medications like carbamazepine or gabapentin relieve nerve pain. An additional choice is to use tricyclic antidepressants. Analgesics available over the counter offer moderate relief.
Nerve Blocks: By numbing the inflamed nerve, anesthetic nerve blocks can provide significant, temporary relief. But as the benefits wear off, the pain frequently returns.
Physical therapy: To help relax the muscles and increase blood flow, the affected thigh and abdomen can be treated using TENS units, massages, stretches, and ultrasounds.
Lifestyle Adjustments: Avoiding activities that aggravate the groin and thigh, taking warm showers, and wearing loose clothing can all help reduce everyday discomfort. Take time to relax and rest to relieve stress.
Acupuncture: Thin needles are inserted into the body at particular locations in this ancient Chinese medicine practice. Acupuncture may help modify pain signals and improve healing, but the specific mechanism is still unclear.
Alternative Therapies: Complementary pain alleviation may be obtained through techniques like cognitive behavioral therapy and meditation.
Prognosis:
The prognosis for ileioinguinal neuralgia varies according to the intensity of symptoms, treatment response, and underlying cause. Conservative therapy results in significant improvement for many patients. Chronic patients may need constant management to control symptoms and prevent recurrence.
What is the physical therapy for Ilioinguinal Neuralgia?
What a physical therapist might include in your treatment plan is as described below:
Massage and myofascial release: By targeting the tight muscles and fascia surrounding the belly and groin, massage and trigger point therapy may relieve nerve compression and enhance blood flow.
Ultrasound therapy promotes tissue healing and pain relief by using sound waves to create heat while improving blood flow to the injured area.
Exercises for strengthening and stretching: A physical therapist will create a customized plan to release tight muscles that may be causing compression of the nerves. Enhancing general stability and support through the strengthening of the hip and core muscles may lessen the strain on the ilioinguinal nerve.
What are the prevention for Ilioinguinal Neuralgia?
Keep your weight within a reasonable range. Being overweight might put a strain on the abdominal wall.
Maintain good posture. Good posture will lessen the strain on your spine and core, which may minimize the chance of nerve compression.
Stretch and warm up your muscles before engaging in any physical activity to help them become ready and to lower your chance of injury.
Make sure your workspace and chair are at the right height if you work at a desk to prevent bad postures that put strain on your back and abdomen.
Steer clear of repetitive activities that could aggravate the ilioinguinal nerve. If your work requires these kinds of motions, stretch and take regular breaks.
Stronger core muscles have the potential to relieve nerve strain by supporting your spine and abdomen more effectively.
Summary
A complicated disorder called ilioinguinal neuralgia can result in chronic pain and discomfort in the groin and lower abdomen. Understanding the structure, anatomy, origins, diagnosis, and available therapies is essential for efficient handling and enhancing the well-being of those impacted. Better results and relief from ilioinguinal neuralgia symptoms can result from early detection and suitable treatments.
FAQs
What is ilioinguinal neuralgia?
Ilioinguinal neuralgia, which occurs when a nerve is wounded or entrapped, is a common source of discomfort in the upper thigh and lower abdomen following lower abdominal surgeries.
What is the test for ilioinguinal nerve entrapment?
Certain diagnostic procedures could be performed for confirmation: A guided injection utilizing ultrasound or CT scan is particularly helpful for diagnosis when the nerve becomes superficial, allowing us to track it down to the superficial inguinal ring.
Which is the medicine used for ilioinguinal nerve blocks?
Anesthetics (bupivacaine or lidocaine) and occasionally steroids (cortisone, Kenalog, or dexamethasone) are injected together.
What causes the ilioinguinal neuralgia?
It is caused by compression of the ilioinguinal nerve in the lumbar (lower) spine region as it travels through the transverse abdominal muscle. Trauma, especially blunt trauma, to the lumbar spine region is typically the cause.
What adverse consequences can an ileoinguinal nerve block cause?
After your procedure, the effects of the local anesthetic will wear off in 12 to 18 hours. It could take the steroid 48 hours to begin acting. There can be a window of greater pain or discomfort during this period. You could feel a little weak in your legs.
What is the treatment for pain in the ilioinguinal nerve?
The first line of treatment for ilioinguinal nerve pain typically consists of nonsteroidal anti-inflammatory, anti-neuropathic, and mild opioid medications. Another cautious approach to localized treatment is the use of qutenza patches.
How is the ilioinguinal nerve released?
Treatment options for iliohypogastric or ilioinguinal nerve entrapment include topical or oral medicine, physical therapy, and local anesthetic injection.
References
Elsakka, K. M., Das, J. M., Leslie, S. W., & Allam, A. E. (2024, February 18). Ilioinguinal Neuralgia. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK538256/
Technologies, W. (n.d.). Ilioinguinal Neuralgia: Causes, Symptoms, and Treatments | Best Back Pain, Slip Disc, Knee Arthritis, Sciatica Treatment in Aundh Pune. Spinalogy Clinic. https://www.spinalogy.com/understanding-and-managing-ilioinguinal-neuralgia
Ilioinguinal Neuralgia | Dr. Vanessa Sammons. (2021, July 8). Dr Vanessa Sammons. https://drvanessasammons.com.au/nerves/pelvis-and-leg-nerves/ilioinguinal-neuralgia/
Lpcadmin. (2017a, June 5). London Pain Clinic: Medication for Ilioinguinal Neuralgia Treatment London Pain Clinic. https://www.londonpainclinic.com/neuropathic-pain/medication-treatment-ilioinguinal-neuralgia/
Physical activities or movements performed without a lot of movement or positional change are referred to as static exercises. These exercises, which usually target particular muscles or muscle groups, concentrate on holding a specific pose or position for a predetermined amount of time
These are easy to execute with little to no equipment by people of all fitness levels. As a type of static exercise, isometric exercises are widely used. The only distinction between isometric and static exercises is that the former uses maximum resistance while the latter holds the muscle without causing any discernible movement. Both exercises function as holding movements and strengthening the muscles. Muscles generate the highest tension and force output possible.
Types of Static Exercise:
Exercise for building muscle: This is an isometric, low-intensity exercise that is done with little to no resistance. It won’t increase muscle strength unless the muscles are extremely weak because it is done at a very low intensity. Stabilization exercise Multiple angle isometrics
Importance of Static Exercise:
It is used to reduce pain or spasms following any soft tissue or muscle injury during the acute healing phase, as well as to promote muscle relaxation and circulation.
During the healing process, muscle setting promotes greater movement between muscle fibers.
aids in preventing atrophy when there is no movement
and increases muscle strength in situations where dynamic exercise is not possible or is not possible at all.
When immobilization is required during a muscle’s rehabilitation, muscle setting can prevent muscle atrophy.
Encourage muscle contraction and activation, particularly following surgery or in cases of acute injury to the joint or the soft tissue around it.
to increase static muscle strength at specific range points by needs related to a given task
Cardiovascular response to Static exercise:
Isometric (iso = same, meter = length) exercise is an alternate name for static exercise, which refers to skeletal muscular contraction without any change in muscle length. Static activity causes a wide range of cardiovascular reactions, as dynamic exercise demonstrates. Static exercises can include commonplace activities like lifting large boxes or carrying a large briefcase, as well as sports like weightlifting and hammer throw.
The prolonged, constant activation of skeletal muscles, which arises when muscle fibers constrict blood arteries, inhibits regional blood flow. When the muscle contracts at 70% of its maximum effort, full blood flow obstruction can happen, although local dilatation of the arteries partially offsets this decrease. Because of the reduction in blood flow, acidic metabolic byproducts can build up and activate muscle chemoreceptors.
Another mechanism regulates how the heart responds to static exercise. The cardiovascular and respiratory control regions are activated in response to increased motor output by this central nervous system mechanism, which has its origins in the higher centers of the central nervous system.
The above-discussed feedback mechanism and this central nervous system mechanism work together to raise heart rate.
But unlike dynamic exercise, this approach results in an almost total increase in heart rate due to the increased cardiac output, without also increasing stroke volume.
Furthermore, due to the somewhat localized nature of muscular tension, there is less systemic vasodilation during static exercise, which results in a different increase in stroke volume than during intense activity; For this, the peripheral circulation compensates. In this condition, an increase in cardiac output is directly correlated with an increase in mean arterial pressure.
As a result, there are noticeable variations between the circulatory reactions to dynamic and static exercise.
Indications of Static Exercise:
during the period of immobilization, such as following the application of casts or splints, or when using different kinds of equipment.
Following any accident or surgery that impairs mobility or makes exercise uncomfortable
Muscle strain
Ligament sprain
Examples of Static exercises for whole-body strengthening:
The exercises that follow will challenge every part of your body to become stronger and identify any weak points. They’re easy to do, straightforward, and will provide you with a solid foundation for developing new strength levels:
Plank:
Planks
Drop on all fours with your feet together, head straight, and hands slightly wider than but parallel to your shoulders. Put your shoulders down, tense your glutes, and tighten your core to lock your body into place. Hold until your muscles give out.
Low Squat:
Low Squat
Put your feet shoulder-width apart.
Pose in a tall position with your hands at your sides, your feet shoulder-width apart, and your toes pointed forward.
Calf Raise Hold:
calf raise exercise
Start by kicking up your heels and using both legs to raise your torso off the ground. After reaching your maximum height, hold this position for one minute and then slowly lower yourself. You can extend the duration by 30 seconds at a time until you reach 5 minutes, or until your body becomes accustomed to the added stress.
Static Lunge:
Static Lunge
Spread your feet hip-width apart and keep your hands by your sides. Step forward with your right foot while maintaining an erect posture in your shoulders and chest. back flat, and core engaged. Hold for a while, completing the same number of repetitions on both sides, until you start to feel tired.
Pull-Up Hold:
Pull-Up Hold
Keeping your hands shoulder-width apart, grasp the pull-up bar. RRaise yourself until the bar and your upper chest reach the same height. For one to two minutes, keep your elbows lowered, press your shoulder bones together, and maintain your solid footing.
Dead Hang:
dead-hang
Grasp an overhand or underhand grip on a pull-up bar with your hands shoulder-width apart. With your toes pointing downward and your legs crossed behind you, let your body hang. Continue until you’re exhausted.
Bridge:
BRIDGE
Rests on your back on the floor. Bend at the knees, place your hands by your sides, and keep your feet and palms flat on the floor. Raise your hips slightly while maintaining your body supported by your feet and hands.
Static back exercise:
Static back exercise
Exercise for a static back: Rest your back on a plinth. Place your leg on the table for support after bending your legs to a 90-degree angle at the knee and hips. Exert your lower back toward the ground while maintaining a breathing pattern. Hold the back down for 30 seconds.
Contraindications of Static Exercise:
could raise blood flow and heart rate, which might not be good for cardiac patients.
During exercise, the patient must not hold their breath to avoid performing the Valsalva maneuver.
During any soft tissue trauma
Pain while performing isometrics
Inflammation
Joint effusion
Infection
Disadvantages of Static Exercise:
Injury risk: Patients should not hold their breath while exercising, as this can increase the risk of soft tissue or muscle injury.
Muscular endurance: You won’t gain muscle strength from isometrics because they require muscle tension without actual movement. Strength training, for instance, increases muscle endurance by directing blood to the muscles. Upon performing an isometric The muscles are deprived of oxygen-rich blood when blood flow to them ceases.
Not made for every person: Static exercise is not recommended for everyone because some patients may become exhausted during exercise or may not be able to continue.
Limited strength: Isometrics and static exercise are not going to be helpful if your goal is general muscle strength.
Time-consuming: Static exercises can take a lot of time because they keep the patient in a single, static position while they work out.
Static vs Dynamic exercise:
Exercises fall into two categories: dynamic and static, each with its own benefits and characteristics. A synopsis of their differences is given below.:
Definition:
Static exercise: Static exercises entail maintaining a posture or position with little to no movement. Although the muscles are contracted, the joints move very little or not at all. Dynamic exercise: Dynamic exercises are motions that are repeated and continuous, actively using a variety of muscles and joints across their whole range of motion.
Muscle Engagement:
Static exercise: Dynamic exercises are motions that are repeated and continuous, actively using a variety of muscles and joints across their whole range of motion. Dynamic exercise: A wider range of muscle engagement is possible during dynamic exercises because the movement requires the cooperation of several muscle groups.
Benefits:
Static exercise: Static workouts are a great way to increase muscle stability, strength, and endurance. They can improve posture, build muscle tone, and strengthen the core. These movements are often included in isometric training and rehabilitation programs. Dynamic exercise: Cardiovascular fitness, general strength, flexibility, and coordination are all improved by dynamic exercise. They support functional movements used in daily life and sports, improve muscular strength and power, and increase joint mobility.
Examples:
Static exercise: Static exercises include planks, wall sits, bridges, side planks, and isometric contractions (squeezing a muscle without moving). Dynamic exercise: Dynamic exercises include things like walking, running, cycling, swimming, weightlifting, squats, lunges, push-ups, and yoga poses.
Impact:
Static exercise: Because there is little to no movement during static exercises, they usually have a lower impact on the joints. Dynamic exercise: The impact of dynamic exercises can vary based on the type and degree of movement. Joint strain may increase with running and other high-impact workouts like leaping.
Static and dynamic exercises are both appropriate in a comprehensive fitness program. A thorough workout that addresses several facets of fitness, such as strength, endurance, flexibility, and cardiovascular health, can be achieved by combining the two styles. It’s critical to select workouts that work for your fitness objectives, skill level, and any unique constraints or concerns you may have.
Summary
Maintaining static postures helps to stabilize the joints in the body. Further, they support the development of a stronger environment for more dynamic exercises, such as full-body active exercises or a wide range of motion exercises for the thighs. One ought to think about including static exercise in their regular training regimen.
FAQ’s
What is static exercise?
Isometric exercises—also called static exercises—involve tense muscles while keeping them long. An isometric exercise requires the prevention of joint motion. Pressing up against a wall or other fixed item will help you do this.le sujet.
What is the importance of static exercise?
Static stretching improves range of motion (ROM), lessens musculotendinous stiffness, and lowers the risk of acute muscle strain injuries by relaxing and lengthening the muscles.
Are static exercises good?
Static hold exercises are a great way to get muscles warm before performing larger muscle movements to help prevent injury. He claims that the key is to increase your body temperature all the way before working out, such as by lifting weights or going for a run.
Is static bad for health?
In general, static shocks do not pose a health risk, although they can be annoying. Thankfully, there is not much of a risk involved with these kinds of electrostatic discharges. Generally speaking, they are just annoying. The greatest danger is that a shock could inadvertently injure you.
Exercises that increase the range of motion in the knee joint can be done passively, actively, or with active assistance.
Types of Knee range-of-motion exercises.
Passive range of motion
Active-assisted range of motion: When it comes to the knee joint, the patient’s own effort and the outside force may be applied in equal measure.
Active range of motion: The final one is an active range of motion, which is the patient’s complete control over the knee joint’s mobility throughout the exercise.
The knee joint
The knee is the largest joint in the body and one of the most vital. When it comes to action involving bearing the weight of the body in vertical (jumping) and horizontal (running and walking) directions, it is crucial.
Additionally, it permits limited lateral rotation when the knee is “unlocked” and flexed, as well as medial rotation when the knee is flexed and at the final stage of extension.
What Is a Goniometer?
The goniometer is positioned next to the knee joint, and the angular distance on the instrument is read by glancing at the numbers. The goniometer is most frequently used by physical therapists to test knee range of motion. The physical therapist can use the goniometer to measure the patient’s range of motion at the initial assessment if they have a limited range of motion in their knee joint. Subsequently, the goniometer can be used to ensure that the intervention is effective.
Types of Goniometers
Although there are many different kinds of goniometers available, the universal goniometer is the most commonly used kind.
Universal Goniometer
Inclinometer/gravity goniometer
Smartphone/Software-Based Goniometer Using a smartphone as a digital goniometer has several advantages, including portability, simplicity of usage, application-based tracking of the data, and one-handed operation.
Arthrodial Goniometer
Cervical rotation, anteroposterior flexion, and lateral flexion can all be measured with this kind of goniometer.
Twin axis electrogoniometer The electrogoniometer has better intra- and inter-rater reliability than a universal goniometer, but it is more difficult to use in clinical patient evaluations; as a result, it is more frequently utilized in research settings.
Techniques for using a goniometer
When measuring the knee range using a goniometer, only one notation scheme may be used.
Adjust and stabilize the knee joint appropriately
Go through the knee’s proper range of motion (ROM) for the affected body part.
After that, palpate the relevant skeletal markers.
Align the goniometer with the landmarks on the knee.
Accurately read the measuring device.
Make accurate measurements (measure and record the knee’s active and passive range of motion, respectively).
Movements of the knee joint
Flexion of the knee: Knee flexion is the action of bending the knee and placing the foot up against the back of the thigh.
Extension of the knee
Anatomical motion: Flexion of the knee
Axis location: the femur’s lateral epicondyle
Anticipated Results.
Placement of the Goniometer
Knee extension
Placement of the Goniometer
Axis location: the femur’s lateral epicondyle
Stationary arm: stretching from the femur to the greater trochanter.
Passive range of motion exercise
When an accident or even a paralysis attack renders the knee joints immobile, the passive range of motion exercise is incredibly helpful. To encourage a quicker recovery of the stiff or flaccid knee joint, therapeutic stretching activities are typically coupled with passive range of motion exercises. Here, the medical professional stretches the knee’s soft tissue to release tension and relax the nearby muscles. The immobilized knee joint experiences less stiffness, rigidity, or even flaccidity thanks to the passive range of motion exercises.
Using a stretching strap is the most popular method for performing this workout. It is more advantageous to perform the passive range of motion (PROM) exercises with the assistance of a therapist. In order to increase muscle flexibility, a qualified practitioner does this kind of exercise by both moving the body into the stretch and holding it there.
First, a therapist is someone who knows when and how to set appropriate boundaries. The second is that the clinician is aware of how long to maintain the stretch. Finally, in order to maximize benefits, therapists are taught to determine whether they are focusing on the right locations. Considering that in the mind.
Exercises involving a passive range of motion are usually administered in cases of paralysis attacks, comatose patients, mending fractures, and even when pain is triggered during active muscular contraction. It’s important to keep in mind, though, that passive range-of-motion exercises are unable to stop muscle atrophy.
Advantages
In addition to aiding in the promotion of healthy joint functionality, passive range of motion exercise helps patients reduce pain, speed up the healing process, maintain and restore the range of motion in knee joints that are injured, gain muscle mass, improve blood flow, and raise oxygen levels.
Suggestions
When executing a knee movement, always maintain the leg’s weight.
Continue moving smoothly and slowly.
If the knee joint or muscle is stiff, don’t push yourself through the motion.
The physical therapist ought to limit their movements to what the knee joint or muscle will allow.
If the knee motions hurt during the passive range of motion, stop and notify a physical therapist.
Passive range of motion exercise
Passive knee flexion in prone
Passive knee flexion in prone
The patient should be instructed to lie in a comfortable position, such as prone, by the therapist first. Subsequently, the therapist held the ankle joint with one hand while placing the other on the back of the thigh. The patient should attempt to assist in bending the knee at that point, as this will help to strengthen the muscles. Perform ten rounds in a session. Work out three times a day.
Passive knee extension in prone
A physical therapist should first instruct a patient to lie in a comfortable position, such as prone with their knees bent. This helps strengthen the knee extensors, thus the patient should also try to assist in straightening the knee during this time. In one session, perform ten repetitions. Work out three times a day.
Passive knee flexion in supine
Next, a medical professional applies pressure to the front of the thigh with one hand while holding the ankle joint with the other. Subsequently, a physical therapist bends the hip and knee in the direction of the face. At that point, when the physical therapist moves a leg, the patient should attempt to assist in bending the hip and knee as well, as this aids in strengthening the knee flexors. For five seconds, a physical therapist holds the affected leg at the endpoint. In one session, perform ten repetitions. Work out three times a day.
Passive knee extension in supine
The therapist should first instruct the patient to lie down in a comfortable position, such as a supine position with their knees bent. The physical therapist next straightens the knee, which means that it is facing away from the face. At this point, the patient should attempt to aid in straightening the knee as well, since this helps to strengthen the knee extensors. Perform ten rounds in a session. Work out three times a day.
Active-assisted range of motion exercise
As the name implies, patients can perform these exercises with some assistance from the physical therapist, from themselves, or by using a band or strap. The patient does the majority of the movements but receives minimal assistance in doing the knee movement appropriately.
These limited knee movements are typically the consequence of weakness or pain from falls, bruises, accidents, or more serious injuries in the majority of cases. When beginning these exercises for the knee joint, a patient may experience severe pain and weakness.
The knee active-assisted range of motion exercise has several advantages.
Improve the lower limb’s overall and knee joint’s functionality.
Increase your level of functional independence.
Reduce pain in the knees.
Both preserve and enhance the integrity of the knee joint.
What is the first step for a patient?
The patient’s home health therapist can teach you the knee joint’s active-assisted range of motion activities. With the help of the patient’s home health therapist, perform the exercises. A patient may receive instruction from a physical therapist regarding proper handholds and assistance requirements. In order to prevent injury or exhaustion, the therapist may also demonstrate the simplest technique to perform each exercise. The majority of patients would rather exercise while supported in bed.
Perform all knee ROM exercises carefully, evenly, and slowly. Avoid overstretching or jerking the knee muscles. Rather than being helpful, this could injure the joint or muscle. At this stage, a patient’s ability to bend a joint is limited.
Request that the patient’s physical therapist promptly inform them if they have reduced pain or persistent soreness following cessation of exercise. Exercises that increase knee range of motion may produce moderate pain, but these should also pass fast. To lessen the pain associated with the exercise, try performing all of these exercises again while adjusting the physical therapist’s level of support.
Active-assisted range of motion exercise
Active-assisted knee flexion in prone
A physical therapist should first instruct a patient to lie down in a comfortable posture, such as prone. Next, a physical therapist directs the patient to bend their knee toward their face; however, the therapist will assist the patient in completing the full range of motion once the patient stops bending the knee. In one session, perform ten repetitions. Work out three times a day.
Active-assisted knee extension in prone
The therapist first instructs the patient to lie down in a comfortable position, such as prone with their knees bent. The patient is then instructed to straighten their knee, which means to move away from their face. Perform ten rounds in a session. Work out three times a day.
Active-assisted knee flexion in supine
Active-assisted knee flexion in supine
The patient is then instructed by the physical therapist to bend both their knee and hip in the direction of their face. Perform ten rounds in a session. Work out three times a day.
Active-assisted knee flexion
Active-assisted knee flexion
The patient should then roll a strap onto their foot and hold both ends of the strap in place. If the patient is not able to achieve the whole range of motion, they are then instructed to pull the strap towards their body side and accomplish the full range of knee flexion. In one session, perform ten repetitions. Work out three times a day.
Active-assisted knee flexion in prone
The therapist first instructs the patient to lie down in a posture that is comfortable for them, such as prone. Subsequently, the patient should roll the strap on their foot and grab both ends of the strap while lying down. Perform ten rounds in a session. Work out three times a day.
Active range of motion exercise
What is the active range of motion exercises?
The patient can use these exercises to fully extend the range of motion in their knee joint. Exercise can help maintain the knee joints’ flexibility, lessen pain, and enhance strength and balance.
Before a patient does the exercises on their own, they should be practiced with a healthcare professional. Do knee exercises daily, or as often as your healthcare provider prescribes. Perform the same sequence of knee joint exercises each day.
Proceed smoothly, slowly, and gently. Avert sudden or abrupt movements. If the patient is in agony, stop. It is quite typical to have some initial pain when doing the action.
Active range of motion exercise
Active knee flexion in prone
The patient is then instructed by the therapist to bend their knee as far as they can without stopping at the endpoint. Perform ten rounds in a session. Work out three times a day.
Active knee flexion and extension in prone
Active knee extension in prone
A physical therapist should first instruct a patient who assumes a comfortable position, such as prone. The patient is then instructed by a physical therapist to straighten their knee as much as they can, although they are not required to maintain this position at the goal. In one session, perform ten repetitions. Work out three times a day.
Active knee flexion in supine
Next, a patient receives an instruction from a physical therapist to bend their knee as much as they can with their hips, without holding at the endpoint. In one session, perform ten repetitions. Work out three times a day.
Active knee extension in supine
Active knee extension and flexion in supine
The therapist should instruct the patient to lie down in a comfortable posture before beginning. The patient is then instructed by the therapist to straighten their hip and knee as well, but they are not required to maintain this position at the finish. Perform ten rounds in a session. Work out three times a day.
Active knee flexion in high-sitting
Active knee flexion in high-sitting
The patient should be instructed to take a comfortable position, like high sitting, by the physical therapist first. The patient is then instructed by the physical therapist to bend their knee as much as they can, although they are not required to maintain this posture at the finish. Perform ten rounds in a session. Work out three times a day.
Active knee extension in high-sitting
A physical therapist should instruct a patient to get into a comfortable position before beginning, such as elevated sitting. Perform ten rounds in a single session. In one day, complete three sessions.
FAQs
What exercise program is best for persons who have tight knees?
Strength, flexibility, and range of motion can all be enhanced by biking yoga. Yoga is great for increasing flexibility, particularly in the potentially tight areas surrounding the knee. Walking.
How can you extend the range of motion in your knees?
If your knee is not totally straight, try this exercise. Let your knee extend straight. Repeat multiple times daily.
What size knee joint is typical?
In a narrow and constricted medial joint compartment, forceful instrumentation may damage the articular cartilage, raising the risk of arthritis down the road.
Which angle gives the strongest knee?
The dynamometer’s axis aligned with the axis of motion, and measurements were taken at joint angles of 25° and 67° to investigate variations in maximal muscle strength.
How does the range of motion test get done?
Goniometers, which come in various sizes and shapes to accommodate the various joints in the human body, display angles in degrees from zero to 180 or 360 degrees.
What angle of the knee is ideal?
Men will usually be around 141°, while women may be 1-2° higher. The reason for the variation is that women’s hamstrings are looser, which permits the knee to extend farther. Many find that a knee angle of less than 140° may be more comfortable for them since tight hamstrings will prevent the knee from fully extending.
What constitutes a knee that functions normally?
Knee Joint: Anatomy & Function Your knees enable your legs to bend and move while supporting some of your weight. Your knees are necessary for almost every leg-based movement, including walking, running, and jumping. An effective form of exercise for those who have knee pain is water aerobics.
What is the typical knee bend?
Contrary to popular belief, a person’s range of motion (ROM) should not exceed 140 degrees. This is because most people have some hyperextension, which causes their ROM to be negative.
What is an abnormal knee range of motion?
This might be best described as having a restricted range of knee extension, both actively and passively.
What results in knee range of motion loss?
Another common cause of restricted range of motion is meniscal tears, especially in the medial or lateral knee menisci. Degenerative alterations or trauma are two possible causes of these injuries.
Do knee ROM workouts exist?
For ten seconds, hold this posture. Slowly stretch your knee straight in reverse, then repeat.
How can the range of motion in my knees be improved?
In conclusion, after an injury or surgery, it is advised that you try to regain your entire range of motion for knee flexion by putting your heel to your butt or as close to it as feasible. You can do heel slides for ten to fifteen repetitions or spend five to ten minutes on a stationary bike early on.
References
Prajapati, N. (2022e, May 19). Knee Range of motion exercise: Passive, Active & Active assisted exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/knee-range-of-motion-exercise/
The disease known as intercostal neuralgia is characterized by neuropathic pain in the intercostal nerves, which are the nerves that run throughout the abdomen and rib cage. Numerous illnesses could be the reason, such as physical trauma, cancer, inflammatory diseases, and infections.
Neuropathic pain can be caused by injury or inflammation of the somatosensory nerves. It might have a variety of reasons, but regardless of the cause, there are similar options for therapy. Learn more about intercostal neuralgia’s symptoms, potential causes, and available treatments and preventative measures in this article.
What is the Intercostal Neuralgia?
Intercostal nerves are the spinal cord divisions that arise immediately below the ribs. The word “intercostal neuralgia” refers to neuropathic pain caused by particular illnesses that aggravate or inflame these nerve roots.
Patients having intercostal neuralgia commonly sense pain in the chest wall as well as the upper chest. Being affected by this condition can be very problematic because the pain can occasionally be extremely resistant to conservative treatment.
Causes of the Intercostal Neuralgia
Post-viral intercostal neuralgia can be caused by viral infections such as the varicella zoster infection, which is known to cause shingles and chickenpox.
A ribcage fracture or impairment to the chest wall could have resulted in this.
An abdominal or chest tumor trapping the intercostal nerve has also been linked to benign tumors.
The intercostal nerve might sustain damage as a result of an accidental surgical treatment. These surgeries entail opening the chest to reach the heart, lungs, throat, or diaphragm.
Add additional surgical treatments, like mastectomies or chest tube replacements.
Pregnancy, although infrequently
Inflammation of the nerves is called neuritis a condition that can cause serious inflammation of more than one intercostal nerve.
Pulling or straining the muscles in the shoulders, chest wall, or back could be another cause.
Idiopathic refers to a condition where there is no obvious cause for it.
Traumatic injury
Symptoms of the Intercostal Neuralgia
Patients typically describe pain in the rib cage areas.
Patients may report pain down the length of their rib cage, or they may complain of discomfort from the back to the chest.
Intercostal neuralgia is frequently described as causing severe, stabbing, or agonizing pain. Some people have said that it hurts like a burning or spasm.
The discomfort is normally intermittent, but it can be made worse by lifting, sneezing, coughing, twisting and turning the torso, and laughing.
A fever, itching, stomach ache, tingling, numbness, limited mobility, and pain in the arms, shoulders, and back are possible associated symptoms.
Risk factors for the Intercostal Neuralgia
Here are some intercostal neuralgia risk factors:
Age: People over 50 are more likely to get intercostal neuralgia.
Chest wall trauma can result from falls, auto accidents, or sports-related injuries.
Repetitive movements: Exercises like weightlifting and rowing that require repeated motions of the chest wall raise the possibility of developing intercostal neuralgia.
The shingles virus can produce excruciating skin lesions and nerve pain. Postherpetic neuralgia is a persistent pain syndrome that can damage the intercostal nerves and is more common in people who have had shingles.
Specific medical conditions: Rheumatoid arthritis, diabetes, and osteoporosis are some of the conditions that can raise the risk of intercostal neuralgia.
Diagnosis of the Intercostal Neuralgia
Intercostal neuralgia’s appearance is frequently mistaken for a heart attack or another cardiac condition. A clinical evaluation is required because light pressure in the intercostal nerve distribution can occasionally cause pain. We can rule out the various causes of intercostal neuralgia with the aid of the tests listed below. These are the following:
In addition to assisting in locating the site of rib and chest pain, chest radiography can detect problems with the heart, lungs, and airways.
Nerve conduction velocity testing: This technique assesses damage and functioning of the nerves.
Ultrasound of the musculoskeletal system: High-definition ultrasonography provides a wealth of information about the condition of the soft tissues involved.
Treatment for the Intercostal Neuralgia
Intercostal neuralgia symptoms can occasionally go away on their own, but for many people, the condition progresses to a chronic state, resulting in ongoing pain and frequently a resistance to painkillers, which can hurt mood and quality of life. For efficient pain management, you might require a mix of therapies, such as some of the ones listed below.
Medications.
Aspirin, nonsteroidal anti-inflammatory medications (NSAIDs), and low-dose opioids typically don’t work well for nerve pain. Over-the-counter medications (OCT) such as capsaicin creams, lidocaine patches, and lidocaine gel might be useful.
Even if you don’t have depression, your doctor may nevertheless prescribe antidepressants to relieve your pain. Although the precise mechanism by which antidepressants relieve nerve pain is unknown, most patients experience some degree of relief in a matter of weeks. Antidepressants such as protriptyline, amitriptyline, doxepin, imipramine, clomipramine, and desipramine can be used to treat intercostal neuralgia.
An additional class of medication that could be used to treat intercostal neuralgia is an anticonvulsant, such as Carbamazepine, Oxcarbazepine, Pregabalin, and Gabapentin.
Opioid-based painkillers
Opioid medications for nerve pain consist of oxycodone, morphine, and tramadol. However, there is a chance of addiction and accidental deaths with opioids. For pain unrelated to cancer, the CDC advises physicians to explore alternative therapies. If you use opioids, you will require close medical supervision from your physician. The lowest practicable dosage is what you can use.
Methods: Your physician might inject steroids and analgesics during a technique called an intercostal nerve block. This may lessen discomfort and reduce inflammation. Dorsal root ganglion pulsed radiofrequency and a thoracic epidural are two further procedures that might be beneficial.
Physical Therapy for the Intercostal Neuralgia
Intercostal neuralgia can be effectively treated with physical therapy. Your posture, strength, and flexibility can all be improved with the help of a physical therapist, and these changes can help lessen pain and swelling. A physical therapist may use the following specific techniques to treat intercostal neuralgia:
Electric modalities: To help reduce pain and inflammation, they include electrical stimulation, heat, cold, and ultrasound.
Breathing exercises: By strengthening the diaphragmatic breathing process discomfort can be lessened and lung function can be enhanced.
Manual Therapy: To increase soft tissue and joint mobility in the thoracic region and ribs, manual therapy procedures include massage, mobilization, and manipulation.
Stretching and Strengthening Exercises can help increase the strength and flexibility of the muscles in the back, chest, and abdomen.
Posture Correction: Intercostal neuralgia may be a result of poor posture. You can lessen the strain on your ribs and intercostal muscles by correcting your posture with the help of a physical therapist.
Prevention for the Intercostal Neuralgia
Intercostal neuralgia risk can be decreased by following certain healthful lifestyle practices. These are the following:
When operating a vehicle, always buckle up.
Timely vaccination against shingles, herpes, and chickenpox Senior immunizations
Wear protective sports gear if you plan to play sports that require contact.
Proper medical care for any inflammatory chronic conditions that are already present.
Summary
Intercostal neuralgia is a condition in which neuropathic pain throughout the intercostal nerves, which are nerves that span throughout the abdomen and rib cage.
Numerous illnesses could be responsible for this, such as physical trauma, cancer, inflammatory diseases, and infections.
Because there are so many possible underlying causes, intercostal neuralgia can be challenging to treat. Furthermore, standard treatments for intercostal neuralgia may not be effective for some underlying causes of the condition. Despite that, people can choose to pursue a variety of preventative techniques in addition to the many treatment choices available.
FAQs
How does the pain associated with intercostal neuralgia feel?
Usually felt as pain, tightness, stabbing, aching, and burning along the rib, chest, back, and upper abdomen, intercostal neuralgia pain will distribute throughout the affected dermatome or in a band-like pattern.
How is intercostal neuralgia tested?
A specialist would first attempt to rule out any other potential root cause for any of the other symptoms before determining intercostal neuralgia as the cause. During a physical examination, they may suggest you push the space between your ribs or take a deep breath.
Which type of doctor handles intercostal neuralgia cases?
This is the neurologist’s area of expertise. Complex therapy may occasionally be administered together with a cardiologist and a therapist (pulmonologist, gastroenterologist). Experts perform diagnostic procedures and write prescriptions for medications to treat intercostal neuralgia.
How severe is intercostal neuralgia?
In adults over 25, intercostal neuralgia is a frequent condition that can arise from a variety of sources. The illness has a severe negative impact on the patient’s quality of life and overall health since it causes ongoing pain and discomfort when moving.
How may intercostal neuralgia be treated?
To provide steroids and painkillers, your doctor could carry out an intercostal nerve block surgery. This may lessen discomfort and reduce inflammation. Dorsal root ganglion pulsed radiofrequency and a thoracic epidural are two further procedures that might be beneficial.
Which cancers result in intercostal neuralgia?
Without the nerve root being directly compressed, osteoblastoma in the thoracic spine may release inflammatory cytokines that lead to intercostal neuralgia. One of the most important symptoms for identifying osteoblastoma in the thoracic spine may be intercostal neuralgia.
Which drugs are given to patients having an intercostal nerve block?
Local anesthetics such as lidocaine or bupivacaine are used to numb the injection site; the numbness normally goes away in two to six hours. A steroid called triamcinolone is used to alleviate pain and inflammation.
What may be misdiagnosed as intercostal neuralgia?
Chest tightness or discomfort: Intercostal neuralgia-related chest tightness, pressure, or discomfort might be mistakenly identified as heart-related pain.
References
Rees, M. (2023, November 22). What is intercostal neuralgia? https://www.medicalnewstoday.com/articles/intercostal-neuralgia#causes
Pietrangelo, A. (2020, January 18). Intercostal Neuralgia. Healthline. https://www.healthline.com/health/intercostal-neuralgia#treatment
Barhum, L. (2023, August 23). Reasons for Intercostal Neuralgia and Ways to Find Comfort. Verywell Health. https://www.verywellhealth.com/intercostal-neuralgia-4802193
Professional, C. C. M. (n.d.-a). Intercostal Nerve Block. Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/17134-intercostal-nerve-block
Lawrence, R. A., & Lawrence, R. M. (2011). Anatomy of the Breast. In Elsevier eBooks (pp. 40–61). https://doi.org/10.1016/b978-1-4377-0788-5.10002-1
What to Know About Intercostal Neuralgia. (2023, July 20). WebMD. https://www.webmd.com/pain-management/what-to-know-intercostal-neuralgia
Bastia, S. (2024, April 1). What Is Intercostal Neuralgia? Alleviate Pain Clinic. https://www.alleviatepainclinic.com/blog/what-is-intercostal-neuralgia/
Coordination exercises are designed to improve the ability to synchronize multiple body parts and systems, enhancing overall physical performance and efficiency. These exercises are crucial for athletes, dancers, and anyone looking to maintain or improve their motor skills.
Definition of coordination exercise:
The capacity to produce motor responses that are accurate, controlled, and fluid—the best possible interplay of muscle function—is known as coordination.
The capacity to choose the appropriate muscle at the appropriate moment and intensity to produce the desired action is known as coordination.
For motions to be coordinated, each of the systems listed below has to be present.
Cerebellum
Vestibular system
Motor system.
Flexibility and ROM.
Deep sensations.
Vision.
Components of Coordinated Movement
Coordination of movement is reliant on:
Perception:- The brain combines motor impulses with sensory feedback to interpret stimuli and form implicit preconceptions. Vestibular and visual signals counteract reductions in preconception. Dexterity:-using the fingers deftly while performing the line motor task. The capacity to start, stop, or alter movement quickly and smoothly while keeping postural control.
Balance
balance
-the dynamic mechanism that keeps the body in an equilibrium position. -A body in equilibrium can be found at rest (static equilibrium) or moving steadily (dynamic equilibrium). -The center of mass or center of gravity of the body remains constant over its support base.
Center of gravity
-It is a hypothetical point of equilibrium where it is reasonable to assume that the body weight is evenly distributed and concentrated. -Ant.2nd sacral vertebra.
Line of gravity
-The vertical line that goes through the center of gravity is called the “line of gravity”.
Base of support
-the limits of the body’s contact area with its support surface.
Receptors involved in coordination and balance
position of sense
To feel position, a variety of muscle senses are employed. the consciousness of one’s fixed position.
Kinesthesia ( kinesthetic sense )
Information from tendons, muscles, and joints is absorbed by sensory receptors.. pertains to joint motion awareness. -EXAMPLE: to detect a moving arm
Proprioception -join receptors’ (mechanoreceptors and sensory receptors’) function -provides feedback on.
joint position
movement
direction
speed
Mechanoreceptors system
There are 3 types of mechanoreceptors
TYPE 1: (RUFFINI MECHANORECEPTORS)
-react slowly to a stationary joint position
TYPE 2:-(PACINIAN MECHANORECEPTORS)
-quickly adjust to modifications in joint position -reduce ligament strain -subtract the motion’s velocity
TYPE 3: (FREE NERVE ENDING)
-transmit data about inflammation and pain.
How can coordination be strengthened?
The nervous system is crucial to the synchronization of movement or action.
The afferent impulses that travel through motor pathways to each muscle group determine how that muscle group contracts.
2) cerebral cortex
Voluntary movement begins, most of the time, but not always, in response to a sensory stimulus. This strategy is predicated on recollections of prior usage patterns.
3) cerebellum The afferent pathways that bring impulses of kinesthetic sensation from the periphery and other areas of the brain, such as the cerebral cortex and vestibular action, to the cerebellum, serve as information-receiving stations.
4) kinesthetic sensation
The proprioceptors in muscles and the understanding of limb position and movement are the origins of the afferent impulses that give rise to kinesthetic experience.
Causes of in-coordination
Atherosclerosis is known to have several causes. They cover both chronic illnesses and those with an abrupt start.
A functional cerebellum, spinal cord, and peripheral nervous system are necessary for coordinated movement. Diseases and injuries that damage or kill any of these structures can cause ataxia.
For fine motor activity, which includes tasks like typing, writing, sketching, playing games, and blowing bubbles, the little muscles in the hands and face must be coordinated.
Gross Motor skills:
Coordinated contraction of a large muscle or group of muscles is necessary for gross motor movement (trunk, extremities) like jogging, walking, and lifting exercises.
Hand-Eye skills:
The visual system can take in visual information, send it through the brain, and then use that information to control or guide the hands to finish a task. like catching a ball, stitching, or utilizing a computer mouse
Incoordination
-Jerky, a rhythmic movement that is referred to as incoordination, is produced when any one of the components that work together to create a coordinated movement is interfered with.
Depending on where the lesion is located, there are four primary forms of incoordination.
A certain muscle group’s weakness or flaccidity is linked to incoordination.
-A lesion to the LMN stops the muscles from receiving the proper signals, or the muscles’ usual response to these impulses is altered.
2. related to muscular stiffness and lack of coordination.
-lesion affecting the cerebral cortex’s motor region other than UMN.
3. Incoordination resulting from cerebellar lesions.
-usually referred to as cerebellar ataxia, is characterized by an erratic, swaying movement that has a noticeable intentional tremor.
4. Dysfunction of the kinaesthetic sense resulting in imbalance.
When a patient has sensory ataxia, also known as tabes dorsalis, they are oblivious to their body’s position in space or the locations of their joints.
Examine your coordination:
Dysmetria
-The term “dysmetria” particularly describes a problem with appropriately scaling movement distance.
Dysmetria can appear in a few forms
1)hypermetria:- when you go too far or step too soon 2)hypometria:-when you step or underreach
Upper limb test for in-coordination:
finger nose test
Nose-to-doctor’s finger test
finger-to-finger test
Alternate nose to finger
Finger opposition
mass grasp
pronation / supination
Rebound test
Tapping of U.E
Lower limb test for in-coordination:
Tapping of L.E
Alternate Heel-to-knee / Heel-to-toe
Toe to examiner’s finger
heel on shin
finger nose test:
From Shoulder Horizontal abduction to Elbow Flexed, shoulder down, and keep at a 90-degree angle.
The person places the tip of their index finger on the nasal bridge.
Nose-to-doctor’s finger test:
Patients & therapists sit opposite each other. The patient is instructed to lie supine and first to touch the therapist’s finger, then their big toe.
finger-to-finger test:
The patient is instructed to abduct their shoulders, bring both hands towards the midline, and roughly match the tip of the index finger with the hands across from them to 90 degrees and their elbow extended.
Alternate nose to finger:
The therapist’s index finger is placed first, then the tip of the patient’s nose.
Finger opposition:
The patient touches each fingertip individually. Speed may be gradually changed.
Mass grasp:
The alteration between opening & closing fists. Full finger flexion to full finger extension. Speed may be gradually increased.
pronation / supination:
Elbow flexed to 90* &close to the body, Patient alternately raises and lowers palms. The elbows can be extended, and the shoulders can be bowed to a 90-degree angle.
Rebound test:
The patient’s elbow was bent, and the therapist applied just enough manual force to cause the patient’s biceps to contract isometrically. Resistance is suddenly released.
Tapping of U.E:
Elbow flexed & forearm pronated, patient is asked to the hand on knee.
Tapping of L.E:
Without elevating their knee, the patient is to tap the ball of one foot on the ground while maintaining their heel in touch with the ground.
Alternate Heel-to-knee / Heel-to-toe:
Without elevating their knee, the patient is to tap the ball of one foot on the ground while maintaining their heel in touch with the ground.
Toe to examiner’s finger:
The patient is advised to touch their big toe and then the therapist’s finger while lying supine.
Heel on shin:
The heel of one foot is moved up and down the opposing extremity’s shin while the person is prone.
Fixation or position holding U.E. /L.E. :
U.E – patient holds arms horizontally in front. (in sitting or standing position) L.E -The patient holds the posture longer. (in a sitting position)
Coordination Tests for Athletes:
To evaluate and enhance an athlete’s abilities and performance, numerous advanced tests are available, such as the Stick Flip Coordination Test, Wall-Toss Test, Block Transfer, Soda Pop Test, Plate Tapping, Light Board, and Test Heel-to-Knee.
Fundamentals of Coordination Activities:
Repeat a few motor exercises repeatedly.
Utilizing proprioceptive, tactile, and visual cues to improve motor performance
An increase in activity speed over time
Tasks are divided into manageable pieces that can be completed accurately.
When assistance is required, it is given.
After two or three repeats, the patient should take a little pause to avoid weariness.
Repetition of accurate performance at a fast rate is necessary to develop an engram.
Every time a new movement is taught, the patient is given a variety of inputs to improve motor performance, such as auditory instructions, tactile stimulation, or positions where they can see the movement.
Exercise for progression:
1) Speed of exercise:- when a patient moves quickly, which needs less control than moving slowly. 2) Range of exercise:-broad range of motion utilizing large joints. 3) Complexity of exercise should begin with very basic motions and work their way up to more complex ones.
Neurophysiological Basis of Developmental Techniques
Sensory Integrative Therapy
1) Tai Chi
-Tai chi and other Chinese movement activities are beneficial for treating a range of ailments. It also emphasizes flexibility, balance, stability, and muscular control, all of which can have major advantages. Also, the motions are extremely soft.
Warmup
-Your leg muscles will get stronger and your balance will be better after this warm-up. -Maintain a slight bend in your knees and both legs wider than hip-distance apart while standing. Your hands can rest on your hips, but your arms should remain at your sides. -Transfer almost 70% of your weight to your right leg by moving gently and methodically. -Do this at least three times.
Torso twists
-Place both hands on your hips to gauge how much you are turning during this exercise. It is not desirable to be rotating from the hips. Instead, You should move your face away from the body in its place. – Although your hips may naturally move slightly with your body, this is a twist for your spine. -They ought to remain equally twisted. – At least five twists to each side should be made.
A take on Holding Up the Sky called Energy to the Sky)
-Core stability will be improved with this exercise. -With your hands at your sides, step your left foot to hip distance apart while maintaining the same starting posture as the warm-up. putting both hands in front of your face, maintaining your arms as straight as possible, and pointing your fingertips in each other’s direction, palms down. -As you inhale slowly and start to extend your arms straight in front of you, then upward until they are above your head, keep your gaze fixed on your hands. -At least five times should be repeated.
Drawing the bow -This workout stimulates the heart and circulation while strengthening the arms, shoulders, chest, and legs. -Pull your arms to the left, create a little fist, and bring them to your chest. Take a breath. Your left arm will naturally stretch somewhat farther than your right since you are rotated. -Look past the “L” your left hand is making in reverse. Breathe in this place, then exhale as you put your hands down, extend your legs, and return to your starting posture.
-Continue on the opposite side. -Be careful to do this on each side at least three times.
Penetrating Heaven and Earth -It stretches and stimulates the body’s front side. Step back in with your right foot after Drawing the Bow. Place your feet hip-distance apart. -Raise both hands to chest height, fingertips pointing inward towards one another while inhaling. Once you’re there, relax and inhale deeply. -As you exhale, bring them back together, maintaining their position in the middle of your body. Make sure to repeat this at least eight times.
2) Pilates
These principles can be applied to the exercises to achieve some advantages: better posture and balance More stability and strength in the core Enhanced synchronization decreased back pain in the lower back increased adaptability Increased awareness of kinaesthetics
The Corkscrew -This exercise aims to facilitate the development of whole-body balance in a supine position while also mobilizing the hips and spine. It’s crucial to try to avoid rotating your spine during this exercise and to let your hips guide the movement instead. As you go, get the cores ready, and don’t put too much strain on your neck. -Osteoporosis patients should not perform this exercise.
The saw -This exercise can help you become more flexible in the hip, spine, and shoulder areas. To get the most out of this exercise, start by sitting tall, maintaining a neutral pelvis and spine, and extending your legs in front of you. Throughout, the pelvis should remain fixed to maintain the coccyx’s contact with the floor. -For people with tight hamstrings or lower backs, this exercise can be modified by adding a block. It serves as an alternative to spine twists.
The Scissors -enhancing hip flexor and hamstring flexibility, strengthening pelvic and spinal stability, and encouraging balance, awareness, and control throughout the body. -With your legs outstretched and arms by your sides, palms down, begin supine. Use both hands to support the hips while the legs are raised higher. Breathe out, divide your legs in half like a scissor, and then inhale again to extend beyond. It is preferable to avoid letting the leg sag too much or drop in front of the face.
The Bicycle -This exercise helps to flex the knees and hips. If you find it too challenging, you can adjust it by lying on your side. Take care throughout this exercise to avoid placing too much weight on your neck.
Swimming -This exercise promotes upper and lower body coordination on reciprocal sides while mobilizing the hip and shoulder joints. Assume a prone position with your spine straight and your legs abducted to hip distance apart. The legs should be stretched together during this exercise; the knees should not be bent. With every count, switch sides and apply pressure on the gluteals. -You can lift one arm or one leg at a time while lying prone to complete this exercise. To incorporate a progression, the movement’s speed can also be accelerated.
3) Frenkel’s Exercises
–Frenkel exercises help ataxic patients regain their coordination by involving a series of movements that get harder and harder. Restoring coordinated, fluid, and rhythmic motions is the goal of Frenkel’s workouts. -Frenkel exercises were designed to compensate for the loss of kinaesthetic sensation by utilizing any remaining portion of the sensory mechanism—most notably, sight, sound, and touch—to establish voluntary control over movement. The steps involved in learning this alternate control method are the same as learning any new exercise; the key components are as follows:
Concentration or attention
Precision
Repetition
General Guidelines for the Frenkel Workouts
The patient can perform exercises unilaterally or bilaterally, with the limbs supported or unsupported.
During the exercise, they should be counted out as the therapist speaks slowly to provide directions.
Exercises should be done within the normal range of motion (ROM) to avoid overstretching the muscles.
Before moving on to more challenging patterns, it is recommended to complete the first easy exercise.
It’s critical that the space be well-lit and that the patients be arranged so they can readily observe every action.
Avoid exercising more than four times a week. To prevent fatigue, take a break between each exercise.
The workouts advance From the most secure to the most difficult positions.
The exercises advance to stopping and starting on command, expanding the range, and carrying out the same movements with the patient’s eyes closed if their voluntary control improves.
Balance and coordination can only be improved with practice and focus.
Frenkel exercises for lower limb
Exercises for the legs in lying
-(laying with one side up) One leg is extended and flexed by allowing the heel to move fluidly across the table. feet flat on the table, knee bent, and hips adducted and adducted. -With the knee and hip extended, perform abduction and adduction by sliding the entire leg across the table. -Both legs are extended and flexible, with the heel gliding on the table. -Extend one leg and flex the other. -The tibia’s shin from the knee to the toe, from one leg to the other. -The heel of one limb is transferred to the other by sliding along the crest of the tibia to the ankle (knee). -The patient may also be instructed, under the therapist’s supervision, to first, place the heel of one leg on various points of the other leg, and extend the toe on one leg, and then the other.
Exercises for the legs in Sitting
Exercises for the legs in Sitting
-The second leg is extended to transfer the heel to a spot on the floor designated by a mark. -the patient was instructed to stand and then sit while in a stride. -Knees together, take a seat or stand. -Hip adduction and abduction during seated.
Exercises for the Legs in Standing
Exercises for the Legs in Standing
-weight is transferred from one leg to the other while the patient is standing in stride. -Stroll along the narrow path. -The patient walks in between two parallel lines. -The patient enters sideways by planting their feet on the designated spot. -Go about and make a turn.
Frenkel exercises for upper limb
-To improve coordination of all upper limb movements, similar exercises can be designed for the patient’s upper limb. The patient would be instructed to place their hand on various points marked on a table or wallboard. -the patient places several objects on a table in front of them, sits down, and touches each one with one hand before moving on to the next. -The patient extends their elbow and wrist while flexing one shoulder to a 90-degree angle. -As quickly as possible, the patient taps both hands on both thighs, alternating between the palmer and dorsal aspects. Additional activities that help with coordination include building with toy bricks or drawing on a blackboard, buttoning, combing, writing, and typing.
4) Strengthening exercise
-A common feature of dysdiadochokinesia is muscle weakness, which makes movement more challenging. Muscle strength also decreases with age. Enhancing balance and muscle strength can be achieved or maintained with the aid of exercises targeting the upper and lower extremities, particularly the shoulders and hips. Exercises that strengthen the core can also be helpful.
5) Balance training
In addition, patients can attempt coordinated arm and leg movements while sitting or standing, tapping their heel and toe alternately on the ground. By making you tense your abdominal muscles and pay attention to your posture at that precise moment, this exercise helps develop your core muscles.
-Static balance control -Maintaining sitting -half-kneeling -tall kneeling -standing postures on a firm surface -tandem, single-leg stance -squat position -working on soft surfaces(e.g.-foam,sand,grass)
Perturbation
-the COG tracks the moving body parts. -learning adaptation: distinguished by a notable decrease in the reactive reaction.
Romberg exercise
-The steps in this exercise are the same as those in the Romberg test. The patient is standing with a chair in front of them and their feet forced on the wall behind them. When they start to lose their balance, close their eyes for 30 seconds after keeping them open for 10 seconds to help them catch their balance. If someone loses their balance, they are told to stand with a chair in front of them and a wall behind them. Make sure the patient can stand alone with their eyes closed as the activity goes on.
Unilateral stance exercise
-asked the victim After a maximum of thirty seconds, place one leg on the ground. Use the other leg for this exercise. As the patient repeats this motion several times, the therapist may see that their balance has improved. As the patient advances in their exercise regimen, they can start working on different surfaces and motions to improve their posture and balance.
Dynamic balance exercise using moveable surfaces
1)Balance board exercise
Balance board exercise
Starting position:
Board: Any type -To find your balance on the board, place your feet hip-distance apart. Hold yourself upright with a neutral spine. -As needed, shift your weight to the center of the board to keep its edges off the ground. -Hold it for at least 30 seconds. -Increase difficulty: Extend both arms straight above your head, palms facing in, and place it down while maintaining a straight spine.
Front-to-back Board: Wobble board -Start from the beginning position. -Make it easier: To keep your balance, use a railing or the wall. -Increase difficulty: Extend both arms straight out from your sides.
Side-to-side Board: Wobble or rocker board Start from the beginning position. -tilt for thirty seconds in each direction. -Make it simpler: Add extra support with a railing. -Raise the difficulty by fully extending both arms from your sides.
Round the clock Board: Wobble board -Start from the beginning position. -The board should be rotated in a clockwise 360-degree circle. -Continue rolling for about 30 more seconds. -Make it simpler: Maintain your balance by using the wall.
2) SWISS BALL
SWISS BALL
Swiss Ball Sitting weight shifting
-This Balance Ball workout starts with you sitting up straight on a Swiss Ball with your feet together on the floor. Without elevating your leg, softly and slowly move the ball forward and backward keeping your back straight.
Swiss Ball sitting leg lifts
-With your feet together, start this Swiss Ball exercise by sitting up straight on a physioball. down your leg, then go to the opposite side as long as the exercise is pain-free, complete two to three sets of ten repetitions on each side.
Swiss Ball Squats
-To do this exercise, place a ball between the patient’s lower back and a wall while keeping your feet shoulder-width apart and pointing forward. Squat slowly while maintaining a straight back. Your knees should not go backward towards your toes; instead, they should be in line with your middle toes.
Swiss Ball Prone Single Leg Lifts
Take a seat on a Swiss ball to start the workout. With the Swiss Ball still in position and your knee straight, carefully raise one leg.
Stability Ball Hamstring Curl
-Stability Ball Exercises: Hamstring Rollout -Benefits: Using your core can strengthen your glutes and hamstrings. -With your legs straight and the backs of your calves resting on a balance ball, assume a flat, laying position on your back. -to ensure that your body forms a straight line from your shoulders to your heels, prepare your core and tighten your glutes to lift your hips off the ground. This is where things begin. -Roll the ball as close to your butt as you can by dragging your heels (until your knees form 90-degree angles). -To gently straighten your legs and return to the beginning position, pause and then roll your feet away from your glutes.
Stability Ball Deadbug
-Exercises with a Stability Ball: Dead bug
Advantage is a full-body exercise that requires coordination between the legs and arms maintaining an upright posture while your arms and legs work independently. Maintain an erect posture as your arms and legs work independently. -As you slowly lower your left leg and right arm to within six inches of the floor (both should stay in line with your body), prepare your core and hold. -To get back to the starting position, reverse the movement, then repeat on the opposite side. -Maintain switching between the sides, doing the same number of reps on each.
Stability Ball V-Pass
-Stability Ball Exercises: V-Up -Prepare your core so that any lower back arch is minimized. This is where things begin. -To form a “V” shape with the ball between your calves, lift your arms and legs by using your abs. -Repeat the motion, alternating between your hands and legs.
Stability Ball “I-Y-T” Shoulder Raise
-Workouts with Exercise Balls – IYT Raise -Extend your legs straight behind you while lying prone on a Swiss ball, pushing your toes into the ground for support. -With your thumbs facing upward, make fists with your hands and let your arms fall straight down towards the floor. This is where things begin. -Raise your arms straight up and in front of your ears, leading with your thumbs, while maintaining a downward pressure on your shoulders. The “I” formation is this. -Lower your arms towards the floor, then raise them once more, but diagonally to form a ‘Y’ shape. -“I-Y-T” is a single set cycle.
Stability Ball Rollout
-Workouts with Exercise Balls – Stability Ball Rollout -Benefits: Your core stability and strength are evaluated with this workout. -With your hands on a Swiss ball, kneel with your legs hip-width apart and your toes planted on the ground for support.
6) Neuromuscular exercise
-By improving the quality of motion in all three planes, the neuromuscular exercise program seeks to achieve functional joint stabilization and improve sensorimotor control. -Many neurological rehabilitation approaches are built on the foundation of increasing and enhancing muscle activation to better motor control. -Exercises in sitting, standing, and lying that involve closed kinetic chains in order to enhance sensorimotor control and achieve a low distributed articular surface pressure through co-activation of the muscles.
7)Proprioceptive neuromuscular facilitation
Tapping
-The technique known as “tapping” involves a therapist applying a light force to a tendon or muscle belly to promote voluntary control. -A rapid contraction of the muscles is a normal response, and tapping is used to assess reflex activity.
Brushing
-Fast brushing is a treatment that uses a battery-operated brush on the skin overlaying the muscle to enhance static holding postural extensors and promote movement responses. -Using this technique, the therapist applies firm, deep pressure to the skin to prevent itching, scratching, or tickling. -The pressure input from rubbing the brush over the skin helps the central nervous system by focusing on touch receptors.
Cryotherapy-Brief
-Ice can be used to help muscles respond by combining the sensation of coolness with pain to cause the desired movement.
Passive Stretching
Passive Stretching
-During neurological rehabilitation, stretch can be applied in many different ways to get different results. Among the stretching techniques employed are
Fast / Quick
Prolonged
Maintained
-The quick stretch that is applied helps to cause a muscle contraction that can result in a brief inhibition of the antagonist muscle and a brief contraction of the agonist muscle. It starts the monosynaptic reflex arc and reflexive facilitation of the muscle by turning on the main terminals of the muscular spindle.
Joint Compression
-Joint compression may improve joint awareness, which will enhance motor control. There are two possible outcomes from joint compression: exhibitory and inhibitory. -Joint compression of the joint surfaces facilitates the work of the posture extensors, which are necessary to support the body. You can apply this compression slowly to impair muscle control or quickly to improve it. It is possible to apply with the help of weight-bearing postures or manually.
Joint compression can be achieved using one of two methods:
1) Light Compression: It is believed that allowing the body’s natural weight to travel down the long axis of the bone helps to avoid muscular stiffness. 2)Heavy Compression: More compression than that provided by body weight is believed to enable co-contraction at the joint that is under compression.
Vibration Muscle Vibration -Neurological patients have benefited from the application of muscle vibration to lessen their spasticity and tone. It is expected that muscle vibrations will enhance both inhibitory neuronal activity in the antagonistic muscle and corticospinal excitability.
-Muscle vibration can be applied in two ways: either at a high or low frequency, and it is essentially applied directly to the selected muscle or tendon.
Whole Body Vibration -Whole body vibration is a relatively new modality that has been used to enhance balance and gait.
Vestibular Stimulation -A very effective method for self-soothing, attentional focus, and a proprioceptive, unique sensory system with multisensory function is vestibular stimulation. Sending particular electrical signals to a nerve in the ear that regulates balance is known as galvanic vestibular stimulation. -It is possible to achieve total body inhibition by moving slowly in all directions—forward and backward, horizontally, vertically, and linearly. -Crawling, extended elbow rolls, and rocking motions on elbows can all be used to exhibit the entire body. -Tonal responses are produced when spinning, and the overflow of impulses to higher centers greatly facilitates movement. -Another benefit of vestibular stimulation is the facilitation of the back extensors when the patient is in the prone position and is moved quickly forward and backward or angularly.
Proprioception Neuromuscular Facilitation (PNF) -A series of stretching exercises known as proprioceptive neuromuscular facilitation are used to increase flexibility and range of motion in both active and passive domains, which helps with motor control and rehabilitation. PNF is regarded as an ideal stretching technique that, emphasizes the development of movement sequence and increasing volitional movement.
-PNF places a strong emphasis on diagonal mass movement patterns that resemble the body’s overall functional movement. -The principles of neurophysiology and functional human anatomy form the basis of PNF exercise.
Three areas are the main focus of PNF therapy methods:
-Enhance the agonist’s motor learning by using rhythmic initiation and repeated movement contractions. -Reverse the antagonist muscles’ motor patterns. -For isometric contraction, two methods are used: rhythmic stabilization and slow reversal.
-learning how to relax your muscles enhances flexibility and reduces spasticity.
-The movement patterns associated with PNF include multi-joint, multi-planar, diagonal, and rotational motions of the limbs, back, and neck. There are several PNF stretching methods, including Contract Unwind, Hold Unwind, and Contract Let go of the antagonist contract.
Contract Relax The antagonist is contracted isotonically to encourage the patient to overcome resistance when stiff muscles restrict one’s range of motion.
Hold Relax starts with the antagonist contracting isometrically against resistance, and then the agonist muscle contracts concentrically.
8) Sensory integrative therapy
-A therapy known as sensory integration therapy makes use of all five senses: touch, taste, smell, sight, and hearing. Repetitive behavior is improved by this therapy. -In addition to therapies like deep pressure, brushing, weighted vests, and swinging, this therapy may involve the use of equipment like swings, trampolines, and slides. It can ease a child’s anxiety. -Using headphones to immerse children in soothing sounds can help mitigate the effects of auditory processing disorders. You can play natural sounds to experience them as they would in real life, such as wind, rain, bird songs, and waves. -A child can freely play with materials that enhance tactile processing, such as mud, dough, sand, water, or bubbles. Making bread dough by hand is a tough and enjoyable project. -Aromatherapy, which involves giving kids a tiny bottle of essential oil to cover up smells they find offensive, is a popular and effective treatment for olfactory sensitivity. -Children often like to guess the flavor of the foods, so play taste games with fruit and other foods. Using food on a plate to play games with could promote sampling. -Children who struggle with proprioception are advantageous to them. such as labor-intensive tasks like pushing grocery carts, moving and stacking books or chairs, lifting large weights like full grocery bags, or raking and digging in the garden. -Seesaws, swings, ride-on toys, and indoor or outdoor trampolines are all beneficial for reducing vestibular disorders.
Visually guided training of gait:
During visually guided gait training, the brain’s oculomotor and locomotor control systems (hand-eye-leg coordination) interact because the locomotor system needs information from the oculomotor system to place the feet correctly during a training session.
In a small trial, patients with mild cerebellar ataxia who underwent gait training with guided steps showed very positive outcomes.
Enhancing one’s gait, performance, and safety can be achieved by using eye movement alone to guide gait training. This involves looking at the foot to ensure proper placement for each step. This easy exercise can be done at home with assistance from family members, but it is task-specific and improves balance, coordination, and speed.
FAQs
How can you improve your coordination?
Maintaining an equally vital, healthy body requires coordination. Different exercises can help enhance your coordination. Simple activities that improve coordination, like hopscotch, juggling, or catching a ball, benefit beginners. Hand-eye coordination and motor abilities are needed for these tasks. as well as hand-eye coordination are required for these tasks.
How do we test for coordination?
Pointing a finger at one’s nose then to the examiner’s finger (finger-to-nose testing) The heel-to-shin test involves running the heel down the shin from the opposing knee. With the help of the index finger, tap the thumb. faster hand movements that switch between pronation and supination.
What is the coordination ability?
The capacity for swiftly and deliberately executing complex spatiotemporal movement structures is known as coordination ability. In this context, coordination skills are viewed as an outwardly apparent result of the central nervous system’s control and regulation mechanisms for motor activity.
What is the main aim of coordination?
The goals of the organization and the individual can coexist peacefully when coordination exists. Explaining to people how achieving organizational goals will also benefit their personal goals, creates harmony between the two sorts of goals.
What are the advantages of coordination?
Conflicts, rivalries, waste, tardiness, apathy, and other organizational issues are reduced through coordination. It guarantees the organization’s efficient operation.
References:
Dhameliya, N. (2022, August 7). Coordination exercise: Types, Test, Exercise – Samarpan Physio. Clinic. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/coordination-exercise-types-test/
Kathiriya, N. (2022, July 24). CO-ORDINATION EXERCISE – Mobile Physiotherapy Clinic. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/co-ordination-exercise/