
Golfer’s Elbow ( Medial Epicondylitis )
What’s a Golfer’s Elbow?
Golfer’s elbow, medically known as medial epicondylitis, is a condition characterized by pain and inflammation of the tendons that attach to the medial epicondyle of the humerus, the bony prominence on the inner side of the elbow. You may get wrist and forearm pain.
The condition known as “golfer’s elbow,” or medial epicondylitis, is a tendinopathy resulting from excessive strain or use on the elbow’s medial common flexor tendon. In addition to epicondylitis, it is also known as pitcher’s elbow, tendinosis, or epicondylalgia.
The shared origin of the forearm’s flexor and pronator muscles is the medial epicondyle. The muscles that originate on the medial epicondyle, such as the pronator teres muscle, flexor carpi radialis muscle, palmaris longus muscle, and flexor digitorum superficialis muscle, are innervated by the median nerve.
The ulnar nerve innervates the flexor carpi ulnaris, which also attaches to the medial epicondyle. Together, these five muscles constitute the conjoined flexor tendon of the medial epicondyle of the humerus.They all have the same origin. This tendon, which is about three centimeters long, acts as a supplementary stabilizer by running parallel to the ulnar collateral ligament after crossing the medial glenohumeral joint.
Medial epicondylitis, another name for golfer’s elbow, is a common condition that causes pain and inflammation on the inside side of the elbow.
The medial epicondyle of the humerus at the elbow joint is the source of the single tendinous sheath that unites the tendons of these muscles. This point of insertion gets inflamed, a condition known as medial epicondylitis, sometimes in reaction to a slight injury and sometimes for no apparent cause at all.
similar to a tennis elbow, which affects the outside at the lateral epicondyle, a golfer’s elbow can cause comparable symptoms. Numerous muscles in the front forearm flex the hand’s fingers as well as the wrist’s pronation and flexion.
The tennis elbow, which develops on the outside of the elbow, is comparable to a golfer’s elbow. It’s not only for golfers either. Golfer’s elbow can also occur to tennis players and other people who clench their fingers or use their wrists excessively.
A golfer’s elbow doesn’t have to stop you from participating in your favorite hobbies or from going to the course. With proper care and relaxation, you can resume your normal activities.
One type of tendinitis that is characterized by tendon inflammation or irritation is medial epicondylitis. Medial epicondylitis is a condition when the tendon that joins the elbow to the wrist rips somewhat due to overuse or trauma. Pain and tendon swelling are the results of these tears.
Pain usually occurs when a person with medial epicondylitis bends their wrist toward their forearm. Often called “golfer’s elbow,” this condition may affect anybody who engages in activities that continuously strain their wrists and forearms.
Epidemiology
10% to 20% of cases of epicondylitis are medial, although they are less frequent than lateral epicondylitis. One research estimates that the prevalence is 0.4% of the total population. It is more prevalent in women than in males and is greatest in people between the ages of 45 and 64. In some professions, the percentage might reach 3.8% to 8.2%. The dominant arm is involved in three of every four instances.
Athletes who have training faults, poor technique, equipment, or functional risk factors such as a lack of strength, endurance, or flexibility are at risk of developing medial epicondylitis. Heavy physical labor, excessive repetition, a high body mass index, smoking, the existence of comorbidities, and demanding psychosocial job requirements are risk factors associated with a particular occupation. Type 2 diabetes and tobacco smoking are examples of general risk factors. Higher educated persons see fewer cases, and they don’t seem to be connected to physical activity, leisure, or recreational pursuits.
Pathophysiology
The overuse tendinopathy known as medial epicondylitis is brought on by persistent, repeated, concentric, or eccentric loading of the wrist flexion muscles and pronator teres muscle, which induces angiofibroblastic alterations. Tendon microtears that reoccur and eventually result in tendonosis are caused by repetitive exercise. The research indicates that all muscles, with the exception of the palmaris longus muscle, are impacted equally, despite the belief that the pronator teres muscles and flexor carpi radialis muscle were the most frequently affected.
There’s no inflammation of the bones. Repetitive microtears in the tendon cause the collagen fibers to restructure and the amount of mucoid ground material to grow. There may be calcification or focal necrosis. Collagen strength then declines, increasing tendon fragility, causing scar tissue to develop, and thickening the tendon. Acute trauma can also result in medial epicondylitis, though less frequently, by causing a quick, strong contraction of the muscles.
Causes of Golfer’s elbow
Playing activities like golf, American football, tennis, bowling, weightlifting, javelin throwing, archery, and other tennis can cause medial epicondylitis. The condition is frequently acquired by pitchers and athletes who throw objects above due to high-energy valgus stresses during the late cocking and acceleration phase. It is said to happen in golfers from the peak of the backswing to the instant before the ball hits the ground. Still, over 90% of instances have nothing to do with athletics. Construction, plumbing, and carpentry are among the aggressive, repetitive labor-intensive vocations that are also implicated.
Common cause: excessive tendon usage
Medial epicondylitis, another name for golfer’s elbow, occurs as by injury to the tendons and muscles that govern your fingers and wrist. The injury is usually caused by severe or repetitive stress, especially by powerful wrist and finger motions. Inadequate warm-up or conditioning, together with improper lifting, throwing, or striking, can also lead to a golfer’s elbow.
Only 9 to 20% of all diagnoses of epicondylopathy are for medial epicondylar tendinopathy, which is less common than lateral epicondylopathy (tennis elbow). Pitcher’s elbow and golfer’s elbow are interchangeable terms. A progressive pathologic alteration of the tendon may lead to irreversible fibrosis or calcification, as well as structural collapse.
Most often, patients complain of chronic elbow pain on the medial side that gets worse with everyday activity. During the late cocking or early acceleration phases of the throwing action, athletes may exhibit more symptoms. Baseball pitchers experience pathology as a result of high-energy valgus stresses produced by overhead throws. There have also been reports involving American football, racquetball, tennis, bowling, archery, weightlifting, and javelin throwing.
However, athletes are not involved in 90–95% of cases. Occupations including carpentry, plumbing, and meat cutting have also been linked to the most frequent etiology of chronic repeated concentric or eccentric contractile loading of the wrist flexors and pronator. Abrupt damage to these tendons in a single traumatic event can potentially cause disease. Workplace trauma has been found to be the root cause of symptoms in several situations. More particular occupational physical characteristics linked to medial epicondylopathy include repeated arm motions in women and vigorous activities in males. Both current and past smokers, as well as individuals with type 2 diabetes, are linked to medial epicondylopathy.
In addition to golf, a variety of hobbies and professions can cause golfer’s elbow, such as:
- sports using rackets. Tennis stroke improperly handled, particularly on the backhand, can result in tendon damage. Injuries can also result from using a racket that is too tiny or heavy or from employing excessive amounts of topspin.
- sports including throwing. Another problem in softball or baseball pitching is improper technique. A golfer’s elbow can also result from throwing a javelin, playing football, or archery.
- lifting weights. Lifting weights incorrectly can strain the elbow muscles and tendons. One example of this is curling the wrists during a biceps workout.
- laborious, recurring moves in the workplace. These are found in trades including carpentry, plumbing, and building.
- squash
- Rowing
- A golfer’s elbow often requires more than an hour of action every day, many days a week.
Signs & Symptoms of Golfer’s Elbow
The primary signs and symptoms include
Tenderness in the elbow on the medial epicondyle
gripping difficulty, overall wrist weakness, and flexor tendon inflammation.
Medial epicondylitis symptoms might appear gradually, especially if the illness was caused by overuse. Some people could have a quick onset of symptoms, particularly after an accident.
Mild to severe symptoms can be linked to medial epicondylitis. Among them are:
- pain that radiates from the inside of the elbow through the wrist to the pinky a weak grip and elbow pain while flexing the wrist toward the forearm
- pain while shakin’ hands
- having trouble extending the elbow
- Tenderness and pain. The pain is usually on the inside of your elbow, but it can sometimes occasionally go down the inside of your forearm. Usually, certain motions make the pain worse.
- rigidity. It might hurt to make a fist and your elbow can feel stiff.
- Weakness. It’s possible that you have wrist and hand weakness.
- Any tingling or numbness. One or more fingers may experience these feelings; often, the ring and little fingers do.
- Certain motions, like swinging a golf club, may make the pain worse.
The patient often reports pain radiating up and down the arm, most commonly to the wrist and, on rare occasions, the fingers, from the elbow distal to the medial epicondyle of the humerus.
In addition, there may be localized pain over the conjoined tendon of the flexor group and the medial epicondyle without any sign of erythema or edema. Additional symptoms include numbness or tingling in the fingers (particularly the ring and little finger), wrist and hand weakness, and elbow stiffness.
Pronation and resistance to wrist flexion cause the pain. Hand grip weakness generally coexists with the pain. Either abrupt or gradual pain development is possible.
Risk factors
The following factors may put you at greater risk of getting a golfer’s elbow:
- 40 years of age or older
performing repetitive tasks for a minimum of two hours per day - Overweight
A puffer
Some could be in danger as a result of things done at work. The tendon may be strained by any action that requires repetitive wrist twisting or bending.
Those with high-risk jobs include: - plumbers and butchers
laborers in construction
ordinary users of computers
workers in assembly lines, chefs, and painters
When to visit a physician
If rest, ice, and over-the-counter pain medicines don’t help your elbow pain and soreness, see your doctor. Seek out help right away if: - You have a fever and a hot, inflamed elbow.
Your elbow cannot be bent.
Your elbow appears distorted.
You fear that you could have a broken bone.
Differential Diagnosis
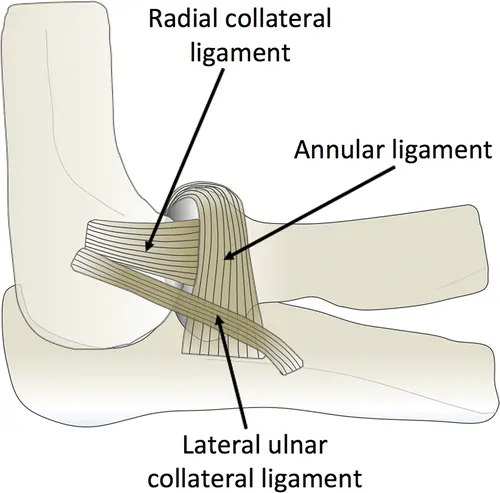
The range of conditions that can cause medial epicondylitis differs greatly and includes ligamentous injury (like ulnar or medial collateral ligament instability, sprain, or tear) and neuropathy (like C6 or C7 radiculopathy, cubital tunnel syndrome, ulnar or median neuropathy, ulnar neuritis, tardy ulnar nerve palsy, also known as anterior interosseous nerve entrapment).
Together with osseous problems like medial epicondyle avulsion fracture or osteophytes, it also includes intra-articular problems like adhesive capsulitis, arthrofibrosis, or loose bodies; myofascial problems like flexor or pronator strain; tendinopathy (lateral epicondylitis, triceps tendonitis); synovitis; valgus extension overload; or dermatological problems (e.g., herpes zoster).
Diagnosis
Typically, a physical examination and your medical history are used to diagnose a golfer’s elbow. The doctor may ask you to move your elbow, wrist, and fingers in different ways, or he or she may apply pressure to the affected region in order to assess your pain and stiffness.
Local pain at the elbow, soreness, and pain when palpated distally and anteriorly of the medial epicondyle are used to make the diagnosis of medial epicondylopathy. Examinable conditions include pronation of the wrist, repeated flexion, and a rise in pain at the medial epicondyle with resisted isometric flexion.
History and Physical Examination:
Patients will describe any history of grasping, valgus stress, or acute traumatic blows to the elbow. They will describe a sharp pain that starts at the epicondyle and travels down into the wrist and forearm on the medial or ulnar side of the elbow. Even though it can cause acute damage, it is often subtle. Throwing, clutching, and forearm mobility all exacerbate the pain.
Tennis strokes with the forearm, golf swing, and overhead throwing are examples of this in athletics. When you stop moving, the agony goes away. Elbow numbness, tingling, weakness, or stiffness are most frequently reported by patients with an ulnar nerve distribution. More persistent presentations could indicate grip strength deficit. In up to 20% of cases, ulnar nerve problems are reported.
Acute instances are more likely to show abnormalities on inspection; chronic cases are less likely to show erythema, warmth, or swelling upon exam. The area five to ten millimeters distal and anterior to the medial epicondyle will be painful for the patient, particularly in the vicinity of the conjoined tendon and pronator teres muscle and flexor carpi radialis muscles. Pain is experienced with resisted wrist flexion or pronation. The affected arm of the patient can be feeble. Usually, the range of motion is normal.
The gold standard for diagnosing medial epicondylitis is magnetic resonance imaging, which is also often performed to rule out other potential causes of medial elbow pain, such as tears or strains in the ulnar collateral ligament, osteochondritis dissecans, or other soft tissue injuries. Computed tomography and bone scans can be helpful in ruling out additional etiologies as well. Electromyograms and nerve conduction investigations may be recommended if there is concern over involvement of the ulnar nerve.
Assessment
The primary diagnostic assessment for medial epicondylitis is clinical. Radiographs are most helpful in excluding other causes of elbow pain since they are often normal. Patients may have periostitis or calcific tendinopathy in 20% to 30% of cases. If a child’s growth plates are still open and the diagnosis is not apparent, it may be necessary to compare the radiological results with the arm that is not affected.
A rapid, simple, and affordable way to assess the muscle and tendon and help differentiate it from other etiologies is with ultrasound. The diagnosis of medial epicondylitis has a strong positive and negative predictive value, sensitivity, and specificity. Furthermore, dynamic assessment is possible. It is possible to see the hypoechoic tissue in regions of chronic degeneration.
The gold standard for diagnosing medial epicondylitis is magnetic resonance imaging, which is also often performed to rule out other potential causes of medial elbow pain, such as tears or strains in the ulnar collateral ligament, osteochondritis dissecans, or other soft tissue injuries. Computed tomography and bone scans can be helpful in ruling out additional etiologies as well. Electromyograms and nerve conduction investigations may be recommended if there is concern over involvement of the ulnar nerve.
- Palpable tenderness, commonly over the flexor carpi radialis muscle and pronator teres muscle.
- Localized edema and warmth
- Test for medial epicondylopathy
- To identify medial epicondylopathy, there are two tests included: an active and a passive one. Patients with severe epicondylopathy may complain of pain even when they are only shaking hands or pulling open a door. The patient must resist wrist flexion during the active resistance test. The forearm must be fully supinated while performing this with the elbow extended. The therapist stretches the elbow and wrist together for the passive test.
- A complete range of motion may be possible early in the illness, although a reduced range of motion may eventually occur.
- It may be necessary to assess the upper extremity kinetic chain as a whole. Strength, mobility, and stabilization of the shoulder and scapula are given special attention. Elbow overuse problems frequently accompany shoulder or scapular dysfunction.
Golfer’s elbow test:
With his or her fingers contracted into a fist, the patient should be either seated or standing. With one hand, the examiner feels the medial epicondyle; with the other, they hold the patient’s wrist. Next, the examiner extends the wrist and elbow and passively supinates the forearm. A complaint of soreness or pain in the area of the medial epicondyle along the medial portion of the elbow would indicate a positive test result.
Treatment of Golfer’s elbow
In order to treat golfer’s elbow, nonsteroidal anti-inflammatory medicines (NSAIDs) are usually used in conjunction with rest pain and inflammation. To increase flexibility and strengthen the forearm muscles, physical therapy activities are frequently advised. A brace or splint may be used to immobilize the elbow and promote recovery in more severe situations.
Medical Management
Ibuprofen, naproxen, or aspirin are examples of non-steroidal anti-inflammatory medicines (NSAIDs). Heat or ice treatment.
An “elbow strap,” also known as a counter-force brace, lessens pain provocation, lessens strain around the elbow epicondyle, and guards against further injury.
- Mini-open Muscle Resection Procedure Under Local Anesthesia
A mini-open muscle excision operation is used to remove the degenerative tissue at the origin of the flexor carpi radialis brevis in cases of medial epicondylopathy. Low levels of pain following surgery, a brief hospital stay, a brief recovery period, and an early return to regular activities are all results of this operation. The possibility of posterolateral instability, the development of neuroma following surgery, and the delayed return to work and athletic activities are the drawbacks of open flexor carpi radialis brevis muscle release.
- Fascial Elevation and Tendon Origin Resection
With little soft tissue dissection, the CFPO (Chronic Flexor Palmar Origin) can be fully seen and resected with the use of facial elevation and tendon origin resection (FETOR). FETOR reduces pain on average, at rest, and during exertion or heavy lifting. Additionally, the mean pain-free grip strength has improved.
- Steroid Injections
When more conservative measures fail to cure chronic pain and disability or when significant acute pain impairs functioning and necessitates an urgent intervention, injectable treatment for epicondylopathy is typically used.
These injections appear to be useful in reducing symptoms quickly—between two and six weeks—and have a short half-life. With the patient to gain as much as possible from the injection, the right placement is required.
- Autologous Blood Injection
Patients with refractory medial and lateral epicondylopathy may benefit from a combination of dry needling and ultrasound-guided autologous blood injection. The VAS pain ratings significantly decreased. The basic fibroblast growth factor and transforming growth factor-ß that are transported in the blood are thought to function as humoral mediators to trigger the healing cascade.
- Extracorporeal Shock Wave Therapy
Patients with recently diagnosed medial or lateral epicondylopathy respond well to extracorporeal shock wave treatment. When administering local steroid injections to a patient is not recommended, this might be an additional alternative. At the targeted location, tissue regeneration might result from the pressure-focused pulses. When recalcitrant chronic epicondylopathy is present, this approach can also be applied.
Surgical Management:
Surgical therapy must be considered when conservative care is ineffective, there is still pain after six to twelve months, and all other diseases have been ruled out. When conservative therapy fails, surgery provides pain relief, strength restoration, and the ability to resume everyday activities and sports participation. It is preferable to do the following surgical procedures:
minimally invasive technique
Scar tissue in the area of the tendon pain is removed under ultrasound guidance.
injections of corticosteroids.
During surgery for a golfer’s elbow, tendon grafts are used to replace or repair damaged tissue.
The procedure known as medial epicondyle release is frequently performed to treat a golfer’s elbow. Around the elbow, this condition can cause excruciating agony. This procedure aims to remove the injured tendon causing the elbow pain. Next, a healthy tendon is reattached in its stead by the physician.
Surgery for medial epicondyle release can be performed in a number of ways. These include open and arthroscopic procedures, which are performed by your surgeon with small skin incisions. The majority of surgeons do this procedure as an outpatient. You may start your progressive healing process at home on the same day as the procedure.
A little incision is made on the side of your elbow by your surgeon. To obtain a clear picture of the tendon, they manipulate the soft tissues. To remove the irritated and injured section, the surgeon makes an incision in this tendon. In addition, the surgeon eliminates any debris or scar tissue that may aggravate pain or inflammation. They use sutures to restore the healthy tendon to its original position.
Physiotherapy Treatment:
The goals of physical therapy are:
- relief of the elbow pain.
- helping in the healing of tissue.
- return of the joint’s range of motion and functionality to normal.
- return of normal strength, length, and movement patterns to the muscles.
- your upper limb neurodynamics returning to normal.
- restoring the cervical joint’s normal function.
Physical therapy treatment Plan :
- Rest: Until the pain subsides, put off playing golf or engaging in any other repetitive activity. Resuming too soon might exacerbate the situation.
- To reduce pain:
IFC (interferential Current therapy)
TENS ( Transcutaneous Electrical Nerve Stimulation )
Ultrasound therapy - Ice: In the impacted region. For many days, apply ice packs to your elbow three or four times a day for 15 to 20 minutes at a time. Use a small cloth to wrap the ice packs over your skin to protect it. Applying ice to the inner elbow for five minutes at a time, two or three times a day may be beneficial.
- Put on a brace: Your physician may advise you to use a counterforce brace on the injured arm to lessen the tension on your muscles and tendons.
- Stretching and Strengthening exercise: exercises for strengthening and stretching may be recommended by your doctor. Chronic tendon irritation has been found to respond particularly well to an eccentric strengthening technique that lengthens the wrist extensor muscle tendon.
Golfers elbow exercises
Your elbow and forearm muscles will experience a reduction in inflammation, pain, and increased blood flow as a result of the exercises. They can help in strengthening and stretching these tendons as well.
Perform the following exercises twice a day to improve flexibility, prevent and treat pain, and build strength.
Over time, progressively and gently build up. Perform these stretches both before and after engaging in any stressful or taxing activity. Don’t overdo any of the movements; instead, be soft. While performing these exercises, you could feel pains, feelings, and mild pain, but nothing more than that.
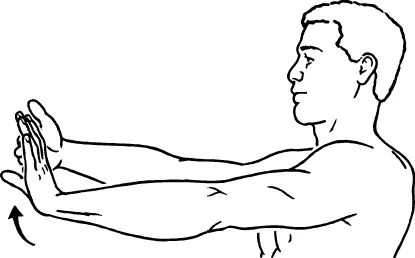
- Isometric wrist strengthening (extension)
You should remain motionless during the exercise.
With your hand facing down, rest your affected forearm on a table or chair arm while seated.
Put the hand that is not affected on the back of the one that is.
Using your unaffected hand as support, press up while applying pressure with your other hand to produce resistance.
Proceed for ten seconds while gradually raising the resistance.
Release gently. Perform 15 repetitions.
- Isometric wrist strengthening (flexion)
When performing this exercise, maintain your posture.
With your palm facing up, place your affected forearm on a table or chair arm while seated.
Place the palm of your other hand against the injured hand.
As you press down with your opposing hand to produce resistance, press your affected hand upward.
Proceed for ten seconds while gradually raising the resistance.
Release gently. Perform 15 repetitions.
- Resisted wrist extension
Hold a weight with the affected arm while sitting.
With your hand dangling over the side and your palm facing down, place your forearm on a table or chair’s arm.
Lower your hand slowly, then bring it back up to the starting position.
Perform one to three sets of fifteen repetitions.
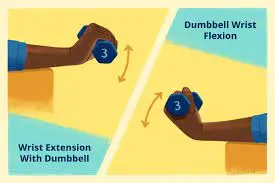
- Resisted wrist flexion
Hold a weight with the affected arm while sitting.
With your palm facing upward and your hand dangling over the edge, place your forearm on a table or chair’s arm.
Lower your hand slowly, then bring it back up to the starting position.
Perform one to three sets of fifteen repetitions.
- Golfer’s elbow stretch
This stretch will be felt in your forearm’s underside.
With your fingers and palm facing up, extend the affected arm in front of you.
Pull your wrist and fingers gently down toward your body with your opposing hand.
For thirty seconds, hold this stretch. Perform two to five repetitions.
- Ball squeezes

A basic exercise with a stress reliever or soft rubber ball is called a squeeze. Form a fist around the ball and place it in the affected hand’s palm. Repetitively squeezing and releasing will build forearm strength.
- Finger extensions
Tighten all five fingers around them with a rubber band. Stretch the fingers apart as much as the rubber band will let.
- Forearm pronation and supination

Holding a dumbbell or other heavy item is part of the exercise.
For stabilization, place the injured forearm on a table or your knee. Hold the thing in the beginning with the palm parallel to the body. Turn the hand so that the back of the hand is facing down. After stepping back to the beginning position, turn the hand so that the palm is facing upward.
Preventing golfer’s elbow
To avoid a golfer’s elbow, you might attempt the following measures:
- Squeeze a tennis ball for five minutes at a time or perform small weightlifting exercises to improve your forearm muscles. Your muscles can absorb the energy of abrupt physical stress with the aid of even basic exercises.
- Before you do anything, stretch. To warm up your muscles, take a few minutes to walk or jog. Stretch a little after that before starting off your game.
- To lessen the impact your arm absorbs as you swing the golf club, alter your technique and slow down.
- Maintaining good form to prevent overusing your muscles.
- Make use of the appropriate tools. Consider switching to lighter graphite clubs if your current set of golf irons is getting outdated. If
- Make sure your racket suits you if you play tennis. Elbow issues may arise with a racket with a big head or short grip.
- Lift correctly. Maintain a firm and tight wrist while lifting anything, including free weights, to lessen the strain on your elbow.
- Water is a great way to stay hydrated before, during, and after your round of golf.
- Recognize when to take a break. Don’t use your elbow excessively. Take a pause as soon as elbow pain appears.
- Return to your regular activities gradually. Practice your sport’s or activity’s arm motions after your pain has subsided. With the help of a coach, check that your tennis or golf swing is accurate and make any necessary corrections.
- Warming up before a round of golf is one of the greatest ways to avoid it. This warms your muscles and increases blood flow, readying your body for more strenuous exercise. Before every workout, stretch your back, shoulders, and arms.
- Before engaging in any sport or activity, warm up: basic active wrist motion combined with a few minutes of walking to help your muscles warm up. Then, to lower your chance of injury, warm up with a few gentle stretches before beginning your game or activity.
- Adjust the form: Check your form when you first start your sport to prevent overusing your elbow muscles.
- Make use of the appropriate tools: Swap out your old golf irons for lighter graphite clubs if you play. Make sure your tennis racket fits you and is lightweight if you play the game. Elbow pain may arise more frequently with a racket with an incorrect grip or a hefty head.
- Lift properly: To lessen the strain on your elbow, make sure your wrist grasp is solid and strong while lifting objects like free weights.
- Make sure you get adequate rest in between tasks or Athletics: By giving your muscles a break, you may prevent overusing your elbow. Take a break if you are feeling tired or experiencing elbow pain.
- Keep up a healthy level of general fitness: Exercise on a regular basis to keep your strength and general fitness. You can increase your endurance and lower your chance of injury by doing this. Incorporate workouts that focus on strengthening your arms, shoulders, and core to offer stability and support during your golf swing.
Keep in mind that while taking these precautions may lessen your chance of developing a golfer’s elbow, they cannot completely avoid the condition. It is advisable to speak with a healthcare provider if you are already exhibiting symptoms in order to receive a precise diagnosis and suitable treatment recommendations.
Golfer’s elbow brace:

If you’re in pain already, you might want to consider using a splint or counterforce brace. Instead of applying stress directly at the site of damage, these devices assist in distributing it throughout the tendon and muscle. Applying a compression bandage is an additional choice.
Nonsurgical Treatment
Pain and inflammation reduction are the primary objectives of conservative therapy. These two measures will facilitate a successful recovery and, eventually, a return to regular activities.
Three stages can be distinguished in nonsurgical therapy.
Phase 1
The patient must cease the objectionable behavior right away. It is not advised to give up on sports or activities entirely since this may result in muscular atrophy.
“PRICEMM,” which stands for “prevention/protection, rest, ice, compression, elevation, modalities, and medication,” is the first step in the therapy. For around a quarter, the affected elbow should be iced many times each day. This enhances the analgesic and vasoconstrictive effects locally. Regarding treatment, nonsteroidal anti-inflammatory drugs (NSAIDs) are an option for the patient.
Night splinting for a while is sufficient if the patient’s condition doesn’t get better. A local corticosteroid injection is often administered in the area where the wrist flexor group originates. Ultrasound and high-voltage galvanic stimulation are two examples of physical treatment modalities (although there isn’t currently research indicating their effectiveness).
It is advised that athletes who exhibit signs of medial epicondylopathy use counterforce bracing. Additionally, it might help when the patient resumes sports.
Phase 2
After phase 1 shows signs of progress, a carefully planned rehabilitation can begin. The establishment of a complete, painless wrist and elbow range of motion is the primary objective of the second phase. Stretching and progressively challenging isometric exercises come next. To reduce the pain, start these exercises with your elbow flexed.
It is believed that strength training reduces tendinitis symptoms, albeit this is not yet proven. In cases of medial epicondylopathy, the short-term analgesic impact of manipulation techniques may enable more strenuous stretching and strengthening activities, which may improve and expedite the damaged tendon’s healing.
The elbow’s flexion can be lessened as soon as the patient shows some improvement. The rehabilitation regimen is expanded to include concentric and eccentric resistance activities as the elbow area’s strength and flexibility recover. A simulation of the patient’s sport or employment completes this step. Research backs up the use of Muscle Energy Techniques (METs) to increase the range of motion. METs are comparatively painless methods that may be applied in therapeutic settings to treat limited range of motion (ROM).
Phase 3
Examining the patient’s gear and/or technique is essential once they are cleared to resume their sport. To enable a safe resumption of activities, several safety measures should be implemented.
Postoperative Management
After the procedure, the skin sutures and splint are taken out seven to ten days later. It’s time to start physical therapy now. The first phase of the treatment consists of mild passive and dynamic exercises for the elbow, wrist, and hands. After three to four weeks, the patient can begin mild isometric exercises. At six weeks, more challenging resistive activities can be initiated. Finally, it is necessary to implement a gradual strengthening program. Typically, the patient can resume their activities three to six months following the procedure.
Home Advice:
These easy-to-do at-home treatments help reduce flare-up symptoms and stop them from coming again.
- Rest:
If your symptoms are severe, take a few days off from activity. Take a rest from any painful movements. Try to change or tweak the motions as much as you can if you have to do them for a job. Raise your elbow over your heart to avoid swelling. - Treatment with heat and ice
Apply an ice pack or heating pad to the injured region. To prevent it from coming into close touch with your skin, wrap it in a towel. Every few hours, spend 10 to 15 minutes doing this. - reduction of pain
For pain relief, take acetaminophen or non-steroidal anti-inflammatory medications (NSAIDs). Take them before the pain becomes worse. Avoid taking painkillers for more than ten days, and always adhere to the authorized dosage.
Cloves, willow bark, and turmeric are natural pain relievers.
Ergonomics
Adjust your posture and stance to allow for better movement if your desk posture, lifting or carrying large bags or things causes you pain.
You may treat golfer’s elbow symptoms as soon as they appear by using the straightforward and efficient exercises shown above. You can perform these many times each day.
A nutritious diet, lots of sleep, and a couple of times a week of exercise are also recommended. After two weeks of therapy, your symptoms ought to go away. experience your doctor if, after this period, you still don’t experience improvement.
Postoperative and Rehabilitation Care
Rehabilitation and postoperative treatment are guided by the surgeon’s decision. An early phase aimed at reducing pain and swelling, early range of motion followed by increasing range of motion, and eccentric strengthening exercises and stretching are typically included in post-operative therapy. The goal of the late phase is to resume activities.
Complications
Persistent pain appears to be the most prevalent consequence of medial epicondylitis. Individuals may experience carpal tunnel syndrome, lateral epicondylitis, rotator cuff tendinitis, ulnar neuropathy, or damage to the ulnar collateral ligament. Complications in surgically treated instances include damage to the ulnar nerve, infection, and medial antebrachial cutaneous nerve neuropathy.
Medial epicondylitis complications are not prevalent. Individuals who cease or reduce their engagement in the activity that first triggered the disease will often heal.
The only people who often encounter new problems are those who persist in engaging in troublesome behavior despite the pain. In certain cases, surgery could be necessary to treat the issue.
Prognosis
For medial epicondylitis, the prognosis is good. Following physical treatment and activity adjustment, the majority of patients are able to resume their jobs or participate in sports.
Conclusion:
The condition commonly referred to as medial epicondylitis or golfer’s elbow, is typified by pain and swelling on the inside aspect of the elbow. It is a typical overuse injury that mostly affects those who do repetitive actions, such as tennis players, golfers, manual laborers, and participants in specific sports.
Although conservative methods can effectively cure most cases of golfer’s elbow, in rare circumstances, surgery may be required to remove scar tissue or repair severely damaged tendons.
A healthcare provider must be consulted in order to receive an accurate diagnosis and a treatment plan that is customized to each patient’s needs.
FAQs
Can yoga help with the golfer’s elbow?
Preventing Tennis, Golf, and Carpal Tunnel Syndromes…
Carpal tunnel syndrome, tennis elbow, and golfer’s elbow are all brought on by these. The best defense against injury to the tendons or deeper tissues is to regularly practice yoga poses that strengthen and extend the arm and shoulder muscles.
Is there a way to help golfers elbow?
Certain natural supplements may be able to assist treat a golfer’s elbow because of their anti-inflammatory qualities. Examples include bromelain, ginger, turmeric (curcumin), and omega-3 fatty acids.
Which foods aid with the golfer’s elbow?
Dietary Avoidance for Golfer’s Elbow
For the best healing, don’t forget to include anti-inflammatory items in your diet, such as fatty salmon, berries, and leafy greens. For individualized advice on the healthiest foods to include or avoid in your diet, speak with your naturopath or nutritionist.
Do pushups improve the golfers’ elbows?
Although pushups are meant to strengthen your shoulders, pectorals, and triceps, performing them will require you to often bend your elbows. This implies that the already damaged elbow tendons will be subjected to further stress. Chin-ups are another popular activity that individuals should refrain from doing while healing from tennis elbow.
Which workouts are best avoided when having a golfer’s elbow?
The Best Golfer’s Elbow Exercises
Exercises for golfers’ elbows to stay away from are:
hefty lifting, particularly when positioned palm up.
tugging or lifting repeatedly.
motions that you perform with your affected side.
Types of injury to nerve damage are golfer’s elbow?
It’s interesting to note that around 60% of people who have golfer’s elbow also have compression of the Ulnar nerve. These patients frequently describe changed feelings in their ring and little fingers, as well as tingling and numbness.
Can the golfer’s elbow be healed?
A physical therapist can teach you these and other strengthening and flexibility exercises. For the most part, the golfer’s elbow may be healed with physical therapy and self-care; additional treatment is not necessary.
Should I apply the golfer’s elbow massage oil?
One common massage technique for treating tennis elbow and golfer’s elbow is transverse friction massage. Applying it to the tendons and muscles requires using one or two fingertip tips.
What is the most effective treatment for pain in golfers’ elbow?
Rest is a crucial part of the golfer’s elbow rehabilitation regimen. Additionally, cooling the wounded region has been demonstrated to be beneficial. This will minimize pain, albeit maybe not enough. You could think about taking some medication to reduce the pain and inflammation if the pain is unbearable.
What is a golfer’s elbow diagnosis?
Medial epicondylitis may typically be diagnosed with a physical examination. When the doctor sets the patient’s arm on a table, palm up, the patient can be instructed to raise their hand by bending their wrist against resistance. When someone has medial epicondylitis, they usually describe soreness in the inside part of the elbow.
Which treatment is best for treating a golfer’s elbow?
The most effective treatment for golfer’s elbow
Rest: Wait until the pain goes away before returning to golf or any other repetitive exercise.
Ice the area that was damaged. Use ice packs on your elbow three or four times a day for a duration of fifteen to twenty minutes each time for many days.
Put on a brace.
Expand and fortify the affected region.
Can a golfer’s elbow totally recover?
Yes, with the right care—which may include rest, ice, NSAIDs, physical therapy, and in certain situations, bracing—a golfer’s elbow can heal completely. In severe situations, longer recovery periods or, on very rare occasions, surgery may be necessary. The chance of a complete recovery is increased with early diagnosis and appropriate care.
Which muscle is activated in the of a golfer’s elbow?
Recent research indicates that a golfer’s elbow often results from damage to a certain forearm muscle. When the elbow is bent, the flexor carpi radialis (FCR) and pronator teres muscles assist in stabilizing the wrist.
How is a golfer’s elbow resolved?
modification of the action.
intramuscular corticosteroids.
Under the direction of ultrasonography, extracorporeal shock wave therapy applies energy waves to damaged soft tissues in the elbow.
Cold.
Anti-inflammatory or painkilling medications.
Physical intervention Exercises for range of motion and treatment.
What causes pain in golfers’ elbow?
Golfer’s elbow, also known as medial epicondylitis, is brought on by damage to the tendons and muscles controlling your fingers and wrist. The injury is usually caused by severe or repetitive stress, especially by powerful wrist and finger motions.
References
- Dhameliya, N. (2023, November 12). Golfer’s Elbow: Physiotherapy Treatment, Exercise – Samarpan. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/golfers-elbow/
- Physiotherapist, N. P. (2023, December 13). Golfer’s Elbow: Causes, Symptoms, Diagnosis, Treatment. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/golfers-elbow-or-medial-epicondylitis/
- Kiel, J., & Kaiser, K. (2023, June 26). Golfers Elbow. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK519000/
- Medial Epicondyle Tendinopathy. (n.d.). Physiopedia. https://www.physio-pedia.com/Medial_Epicondyle_Tendinopathy


One Comment