Distal Radioulnar Joint
The distal radioulnar joint (DRUJ) is a synovial pivot joint located between the distal ends of the radius and ulna. It allows for forearm rotation (pronation and supination) by enabling the radius to move around the fixed ulna.
Stability is provided by the triangular fibrocartilage complex (TFCC), along with ligaments and muscle support. The DRUJ plays a crucial role in wrist and hand function, facilitating smooth and coordinated movement.
The palm faces up when it is supinated and down when it is pronated. These movements are specific to the upper limb’s forearm inside the human body.
Introduction
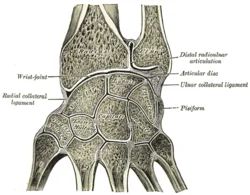
A synovial pivot joint connecting the radius and ulna, the distal radioulnar articulation is also referred to as the inferior or distal radioulnar joint. Along with the proximal radioulnar articulation, it is one of two joints that connect the radius and ulna. The dorsal radioulnar and palmar ligaments strengthen the joint, which has an articular disc.
The distal radioulnar joint (DRUJ) maintains the integrity of the articulation between the distal ulna and distal radius, which is crucial for anteroposterior translational stability, forearm pronation, and supination. A vital supporting component of the ring, the distal radioulnar joint stabilizes the ulna and radius. Disorders affecting this joint can affect the elbow, wrist, and hand.
The distal radioulnar joint is of great clinical significance because it can sustain an acute injury or develop chronic degeneration as a result of long-term aftereffects of prior traumas. Significant wrist pain, dysfunction, degeneration, and mild to severe instability are caused by this spectrum of pathology.
Structure
During pronation and supination, the distal radioulnar joint’s main function is to support the radius’s articulation around the immobile ulna.
Osteology
There is an ulnar head and a styloid process on the distal ulna. Between them lies a fovea, or depression. The ulnar head is situated inside the radius’s sigmoid notch. They attach to the radioulnar ligaments near the styloid process. The styloid process, the sulcus of the extensor carpi ulnaris tendon, the fovea, and the form of the joint cartilage all influence the distal end of the ulna’s shape.
According to an anatomical analysis of this osseous structure, the sigmoid notch’s length increases from volar to dorsal. Significant variance also exists in the ulnar length, which was found to be negatively correlated with the sigmoid notch’s mid-coronal length.
The ulnar variance was also observed to correspond with the obliquity of the distal radioulnar joint. The sigmoid notch was seen to be angled in a proximal-ulnar direction in patients with a typical negative ulnar variation. However, as the ulnar variance increased, this became less angled, ultimately leading to a reverse obliquity.
Articular disc
The joint has a triangular articular disc whose base is connected to the inferior margin of the ulnar notch and whose apex is connected to a fossa at the base of the ulna’s styloid process. The distal extremities of the two bones are securely joined by the articular disc.
Articular surfaces
The concave ulnar notch of the radius and the crescent-shaped convex distal head of the ulna articulate to form the distal radioulnar joint. The hyaline cartilage lines both surfaces.
A triangular fibrocartilaginous articular disc is present in the joint. The base of the disc is fixed to the inferior edge of the ulnar notch of the radius, and the tip is connected to the lateral surface of the styloid process of the ulna.
In addition, the disc’s inferior surface contributes to the radiocarpal joint and the distal radioulnar joint. Since the disc’s center is narrower than its periphery, a possible perforation would allow the distal radioulnar and radiocarpal joints to communicate.
Joint Capsule
The “L” form represents the radioulnar joint cavity. The fibrous ring that surrounds the distal radioulnar joint is known as the radioulnar joint capsule. To allow for the twisting of the capsule with pronation, it features a sack-shaped depression.
Though less research has been done on their roles in preserving joint stability, the articular disc, joint capsule, and interosseous membrane are all included in the sectioning sequences employed in biomechanical studies and have not always been linked to the joint’s overall instability.
Ligaments
The primary stabilizers of the distal radioulnar joint (DRUJ) are the radioulnar ligaments. These are the triangular fibrocartilage complex’s (TFCC) proximal condensations.
The ulna is prominent on the styloid process’s dorsolateral aspect. This is the location where the radioulnar ligaments attach. The articular surface of the fovea and the styloid process of the distal ulna are joined by the radioulnar ligaments. The radius and ulna are joined to form the radioulnar joint by the volar and dorsal radioulnar ligaments. Stabilizing the DRUJ during dynamic loading requires the radioulnar ligaments, which join the distal ulna and articular disc. The distal radioulnar joint and the wrist joint cavity are divided by the articular disc.
The triangular fibrocartilagenous complex (TFCC) and the volar and dorsal radioulnar ligaments (RULs) combine to form the structures that support and stabilize the distal radioulnar joint (DRUJ).
The primary stabilizers of the distal radioulnar joint are the radioulnar ligaments. The triangle fibrocartilage complex has these proximal condensations. According to the current theory, the palmar radioulnar ligament becomes relaxed during supination while the dorsal radioulnar ligament gets tight during pronation.
There have also been several studies on the role of the radioulnar ligaments in preserving the translational stability of the distal radioulnar hip. The dorsal radioulnar ligament is particularly important for dorsal translational stability during forearm pronation, according to these findings. The stability of volar translational stability with the forearm in supination is correlated with the palmar radioulnar ligament. Furthermore, in the biomechanical investigation conducted by Ward et al., it was discovered that radioulnar ligament disruption increased the rotational range of motion. According to this new report, the ligamentous complexes are crucial for the distal radioulnar joint’s rotational stability.
Triangular Fibrocartilage Complex (TFCC)
Lesions of the triangular fibrocartilage complex (TFCC), which is essential for maintaining the distal radioulnar joint, are the most frequent cause of DRUJ instability. In addition to the articular disc, proximal and distal laminae, volar (anterior) radioulnar ligament, dorsal radioulnar ligament, ulnar collateral ligament, ulnolunate ligament, ulnotriquetral ligament, ulnocollateral ligament, and the insertion of the extensor carpi ulnaris tendon on the fovea, the triangular fibrocartilage complex is made up of these elements.
A component of the triangle ligament is the fovea. The distal ulna is where a radioulnar ligament is located. The distal radioulnar joint’s ligamentous stability is mostly attributed to the foveal connection. Under pressure on the wrist, the ulnar variation may result from the disruption of the triangular fibrocartilage complex.
Interosseous Membrane
The radioulnar joint is stabilized by the interosseous membrane, particularly when it is supinated. The interosseous membrane and the triangular fibrocartilage complex join the ulna and radius. The central, proximal, and distal bundles of the forearm are the constituents of the interosseous membrane of the forearm. Stability over time is influenced by the interosseus membrane.
Both the triangular fibrocartilage complex and the central band of the interosseous membrane play a crucial role in providing the radius with axial stability in situations of proximal radial head fracture. A distal radioulnar joint fracture can cause instability in a variety of ways, including anterior, posterior, and intermediate.
Innervation
The anterior and posterior interosseous nerve branches provide innervation for the distal radioulnar joint. The radial nerve is the origin of the latter, whereas the former is a branch of the median nerve.
Blood Supply and Lymphatics
The anterior interosseous artery’s palmar and dorsal branches supply blood to the distal radioulnar joint. A lesser degree of joint vascularization is contributed by the ulnar and posterior interosseous arteries.
The palmar and dorsal branches of the anterior interosseous artery provide the majority of the arterial supply to the distal radioulnar joint. At the pronator quadratus’ proximal boundary, these arteries split off to form an anastomotic complex. The dorsal interosseous artery to the dorsal branch of the anterior interosseous artery, the ulnar artery to the palmar branch of the anterior interosseous artery, and collateral circulation from the dorsal and palmar carpal arches are further contributions produced by anastomoses.
Although the upper extremity’s lymphatic channels are not well understood, some routes have been identified, such as perforators that enable access to the wrist compartment. These flow inconsistently from deep to superficial or superficial to deep, draining from distal to proximal. In the upper extremities, the cubital and axillary regions are where primary lymph node collections are found.
Related Muscles
The wrist, hand, and finger flexors and extensors give the distal radioulnar joint more soft tissue support and stability. In particular, the pronator quadratus is noteworthy. The pronator quadratus plays a part in tensioning the distal radioulnar joint, according to a biomechanical study.
The pronator quadratus’s superficial and deep heads both attach to the palmar aspect of the radius after emerging from the dorsoulnar aspect of the ulna. By allowing the distal radioulnar joint to be tensioned during pronation, this posture helps to avoid capsule interposition and joint diastasis.
Function
As a load-bearing joint, the radioulnar joint’s function is to raise and move weight from the distal radioulnar joint and distribute it across the ulna and radius of the forearm. The radioulnar joint can range from 0 degrees neutral to about 80-90 degrees in supination and 0 degrees neutral to about 70-90 degrees in pronation.
The palms are facing up (supination) as opposed to down (pronation). All pronator muscles (brachioradialis, pronator quadratus, and pronator peres) and supinator muscles (biceps brachii, brachioradialis, and supinator) have a role in this function.
Movements
The distal radioulnar joint, in conjunction with the proximal radioulnar joint, allows the forearm to rotate around a sagittal axis. The distal radioulnar joint has one degree of flexibility and is uniaxial;
- Pronation (61-66°) – supination (70-77°)
The distal end of the radius revolves around the ulna’s head during these motions. The rotational axis is dynamic and varies according to the location of the forearm. The axis in supination travels through the ulnar attachment of the articular disc in the distal radioulnar joint as well as through the center of the head of the radius proximally. The distal point of the axis travels medially during pronation, passing through the ulna’s head.
The distal radioulnar joint assumes a closed, packed form at 5° of supination. The forearm is in the open-packed (resting) position when it is 10° supinated. The distal radioulnar joint has a broad range of motion in its capsular arrangement, with discomfort at excessive rotation. The ulna’s head can glide anteroposteriorly against the radius thanks to the distal radioulnar joint.
Muscles acting on the distal radioulnar joint
The pronator quadratus and pronator teres are the muscles that cause the forearm to pronate at the distal radioulnar joint. When the action is not resisted, the pronator quadratus can perform it; however, rapid motions and movements against resistance require the pronator teres.
The supinator muscle produces supination when the forearm is stretched and not under strain. The biceps brachii muscle serves as an accessory supinator during resistance exercises and/or forearm flexion.
Embryology
Although the triangular fibrocartilagenous complex has been the subject of extensive embryologic research, few studies focus on other wrist ligamentous structures. According to reports, the ligamentous structures start to form in O’Rahilly stage 23 embryos and are finished by week 14.
The onset of wrist joint creation is indicated by the presence of the Interzone, a section of the condensed mesenchymal structure. The growth of the wrist’s ligamentous structures is believed to be mostly dependent on the intermediate layer, one of the three layers that make up the Interzone.
Clinical significance
The distal radioulnar articulation is frequently injured when someone falls onto an outstretched hand. Injury may be solitary or may coexist with a distal radius or ulna fracture. The distal radioulnar distance’s upper limit has an origin range of 2 to 5 mm. A classification framework has been provided by Estaminet and companions.
Estaminet Classification
Two subtypes of distal radioulnar articulation injuries were identified by Estaminet: those that were solely ligamentous (subclass A) and those that had accompanying bony injury (subclass B).
- Attenuation on MRI alone (Estaminet I)
- The Volar Distal Radioulnar Ligament is implicated (Estaminet II). Supination instability. In pronation, the fixation should be.
- The dorsal distal radioulnar ligament is implicated (Estaminet III). unstable when prone. Supination is the proper fixation position.
- The two ligaments are affected by estaminet IV. Pronation and supination are both unstable. Fixation is in a neutral state.
FAQs
The distal radioulnar is what kind of joint?
The ulnar notch of the distal radius and the head of the ulna are separated by the distal radioulnar joint, a pivot-type synovial joint.
How does the distal radioulnar joint look, and how does it function?
Significant rotational and translational motion is possible at the distal radioulnar joint (DRUJ), a complicated articulation. Bony contact, the triangular fibrocartilage complex’s intrinsic stabilizers, and the distal forearm’s extrinsic stabilizers are all necessary for the DRUJ to remain stable.
Which pair of bones make up the distal radioulnar joint?
A synovial pivot joint connecting the radius and ulna, the distal radioulnar articulation is also referred to as the inferior or distal radioulnar joint. Along with the proximal radioulnar articulation, it is one of two joints that connect the radius and ulna.
In what way can a distal radioulnar joint be fixed?
When instability occurs, the patient must either undergo open reduction through an incision centered over the DRUJ to rejoin the TFCC and repair the capsule and ECU or extra-articular pinning in the decreased position for six weeks while immobilization captures the elbow. If there is no instability in the ECU, arthroscopy can be used to repair it.
What kind of motion takes place at the distal radioulnar joint?
During pronation and supination, the distal radioulnar joint’s main function is to support the radius’s articulation around the immobile ulna. The ulnar head and styloid process are features of the distal ulna. Between them lies a depression, or fovea.
What is the typical distance between the distal radioulnar joints?
In volar ulna dislocation, the distal radius and ulna overlap, although normally, there is a difference of 2-3 mm between them.
What is the main way that the distal radioulnar joint is stabilized?
The palmar radioulnar ligament was found to be more crucial than the dorsal radioulnar ligament in stabilizing the distal radioulnar joint in pronation, and the dorsal radioulnar ligament was more crucial than the palmar radioulnar ligament in pronation when the interosseous membrane was first disrupted.
What are the distal radioulnar joint stabilizers?
Primary and secondary stabilizers of the DRUJ have been identified in some anatomical soft tissue structures. The pronator quadratus, flexor carpi ulnaris (FCU), and extensor carpi ulnaris (ECU) muscles provide dynamic stability (Johnson and Shrewsbury, 1976; Linscheid, 1992).
DRUJ injuries: What are they?
An irregular orientation or movement of the radius and ulna bones at the wrist relative to each other is known as distal radioulnar joint instability. Damage to the muscles, ligaments, and/or tendons that support the joint can result in partial or total dislocation.
References
- Distal radioulnar joint. (2023, November 3). Kenhub. https://www.kenhub.com/en/library/anatomy/distal-radioulnar-joint
- Wikipedia contributors. (2025, January 4). Distal radioulnar articulation. Wikipedia. https://en.wikipedia.org/wiki/Distal_radioulnar_articulation