Carpal Bones
Introduction
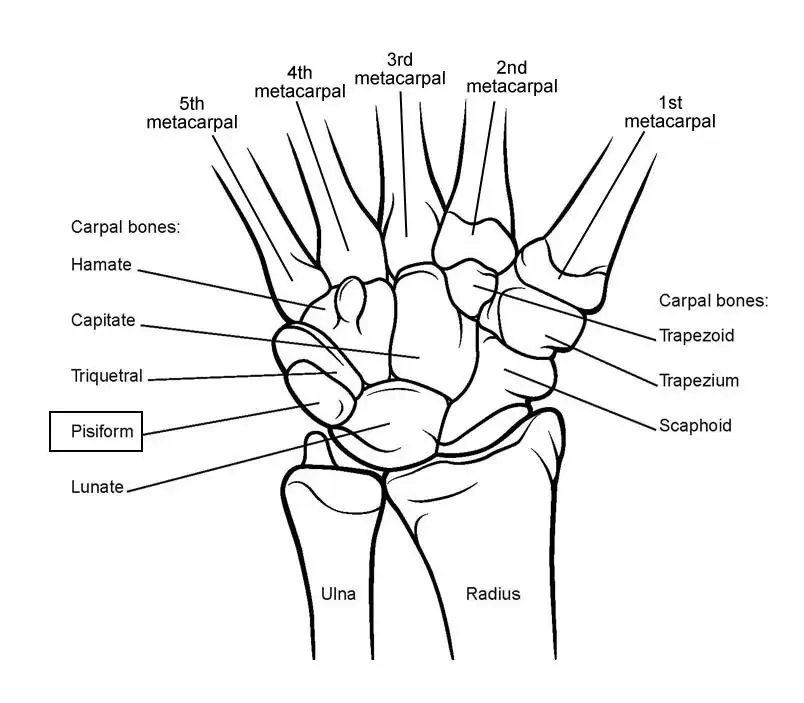
The wrist bones known as the carpal bones connect the distal ends of the radial and ulnar bones of the forearm to the bases of the five metacarpal bones of the hand. The proximal and distal rows include the two rows of the eight carpal bones.
From radial to ulnar,
- Proximal rows: Triquetrum, lunate, scaphoid, and pisiform.
- Distal rows: Hamate, trapezium, trapezoid, and capitate.
These bones comprise the majority of the wrist’s skeletal structure and provide the innervation and blood supply for various neurovascular systems and tendons that enter the wrist to reach specific bone structures and muscle groups and provide the blood and innervation needed for their correct functioning.
Structure and Function
Each carpal bone in the wrist has a unique function and purpose that sets it apart from the others. The scaphoid bone forms the radial boundary of the carpal row. Because articular cartilage covers almost all of the scaphoid’s surface, it can bridge the joint between the two rows of carpal bones.
The lunate, so named because of its crescent form, is situated next to the median nerve and between the scaphoid and triquetrum The pisiform, lunate, and hamate bones articulate with the pyramid-shaped triquetrum. Finally, the pisiform is a pea-shaped bone that articulates on the dorsal aspect of the triquetrum and acts as an attachment point for many tendons and ligaments.
The trapezium bone is situated between the base of the first metacarpal bone and the scaphoid, anterior to the distal row. For articulation, the first metacarpal carries a saddle-shaped facet. A few tendons and ligaments can either connect or pass through this point. The trapezoid, the smallest carpal bone, is located between the capitate and the trapezium.
With attachments to several intercarpal ligaments and articulations to various other bones, the capitate is the biggest and most central carpal bone.
The skeleton of the hand is typically organized into three arches: a longitudinal arch that extends throughout the hand’s length, two transverse arches at the carpus, and the other at the metacarpal head levels. Specifically, the carpal bones create a transverse arch that creates the carpal tunnel’s floor and provides protection for the fingers’ flexor tendons and median nerve.
In addition, the prominent forward tubercles of the scaphoid and trapezium have a major impact on the bone architecture of the carpal tunnel. Additionally, the thumb has a supportive base due to these tubercles, which allows it to resist the rest of the hand and enhances the hand’s capacity to grab items.
Embryology
The limb buds open on Days 26 and 27. A cluster of mesenchyme wrapped in ectoderm makes up each limb bud. Until it is ready to later in development differentiate into bone, cartilage, and blood vessels, this mesenchyme stays undifferentiated. In the meantime, the ectoderm thickens at the apex of every limb bud to produce the apical ectodermal ridge, which promotes the proximal-distal axis growth and development of the upper limb opening.
By controlling growth along the anteroposterior and dorsoventral axes, respectively, other signaling centers and primary morphogens, such as the pathway of Wnt expressed from the dorsal epidermis of the limb bud and the zone of polarizing activity derived from an aggregate of mesenchymal cells in the limb develop, also contribute to the development of the upper limb bud.
The capitate and hamate carpal bones are the first chondrogenic sites to emerge as juvenile cartilage early in the eighth week; the pisiform occurs later in the eighth week.
The “hamate” starts to take shape by the end of the ninth week. It doesn’t reach full growth until the twelfth week. Blood Supply and Lymphatics. At the fourteenth week, a vascular bud finally breaks through the lunate cartilage mold, initiating the osteogenic process that will last for the first year of life.
Blood Supply and Lymphatics
The anastomoses, ulnar artery, and radial artery all provide blood to the wrist. The ulnar artery supplies blood to both the medial side of the index finger and the fingers that were spared. The vascular supply is specially handled by the anastomotic network, which is composed of three dorsal and three palmar arches that span the carpal bones and arise from the radial and ulnar arteries. There is a single intraosseous vascular supply in the scaphoid, capitate, and a small percentage (20%) of lunates. A single intraosseous vascular supply can be seen in the capitate, scaphoid, and a small subset (20%) of lunates.
The scaphoid’s proximal pole is particularly susceptible to avascular necrosis since it only has one blood supply—the radial artery—which enters the bone from the distal end and supplies the proximal section.
There are two blood flow zones in the hamate and trapezoid without intraosseous anastomoses. Thus, following a fracture, the other carpal bones (save the scaphoid, capitate, and a small number of lunates) are less likely to develop avascular necrosis.
Nerves
The wrist joint’s innervation comes from the:
- The interosseous branch of the anterior branch of the median nerve.
- The radial nerve’s posterior interosseous branch,
- Ulnar nerve’s dorsal and deep branches.
Dorsum side:
This site is associated with the superficial branch of the radial nerve, the dorsal branch and perforating branches of the ulnar nerve, the posterior interosseous nerve, the lateral antebrachial cutaneous nerve, and other nerves.
Palmar side:
The wrist joint is innervated by
- the anterior interosseous nerve
- the palmar cutaneous nerve (median nerve branch)
- the deep branch and main trunk of the ulnar nerve.
Muscles Around Carpal Bones
Extrinsic and intrinsic hand muscles are two different kinds. By maintaining the hand’s position on the concave radial surface during co-contraction, tendons that enter the wrist and muscle bellies that begin in the forearm contribute to the stability of the wrist. Due to their connection to the metacarpal bases, intrinsic muscles, which have their origins in the hand itself, also balance flexor and extensor forces, assisting in wrist stability.
The wrist joint may be flexed and adducted by the extrinsic muscle known as the flexor carpi ulnaris, which is connected to the hamate, pisiform, and base of the fifth metacarpal bone. All intrinsic muscles originate from the carpal bones on the front side.
The thenar muscles originate from the scaphoid and trapezium tubercle. The capitate, second, and third metacarpal bones, are the source of the adductor pollicis while The pisiform and hamate bones are the source of the muscles of the hypothenar area, such as the flexor digiti minimi brevis, opponens digiti minimi, and abductor digiti minimi.
Anatomical Variantions
Even though they are rare, additional bones, split bones, anatomical variations, and congenital defects can affect how many carpal bones there are. There are reports of more than twenty different accessory carpal bonesThe triangular bone, the centrale carpi, the radiale externum, and the stylopodium bone are the most often described changes.
The scaphoid, lunate, and possibly hamate split bones are possible extra carpal bone examples. The lack of fusion from the carpal bones’ ossification centers results in morphological differences that create additional carpal bones. Finally, congenital defects that result in fewer carpal bones might arise from a coalition between two carpal bones, most often the lunate and triquetrum, or a congenital lack of normal bone.
Surgical Importance
There are two types of surgical methods for the carpus: general and specialized carpal exposes. Both dorsal and volar approaches to general exposures offer extensive exposure to wide regions of the wrist and give surgeons access to pathologies involving numerous joints or carpal bones. Specific exposures provide limited exposure and permit access to a particular bone, often the scaphoid, or joint in situations where the diagnosis is definite treatment plan is necessary.
Because the deep structures of the carpal and hand are so near to one another, extra attention must be paid while performing surgical procedures on the hand and wrist. F An in-depth examination of the anatomical links between important ligaments, tendons, nerves, and blood arteries should begin with the initial skin incision. To prevent harm to essential components of the hand and wrist, the incision design must take into account the proximity between these tissues. These include the creases in the skin to prevent contracture, the blood flow to the skin or skin flaps for the early healing of wounds, the sensory homunculus of the hand, which is mostly composed of nerves, and even the patient’s choice of hand cosmetics.
Clinical Significance
Hand and wrist injuries are prevalent among athletes; studies show that athletic events are responsible for about 22% of adult hand fractures. 54%). When someone falls on an outstretched hand, the scaphoid receives most of the stress from the radius because of its size and anatomical location (FOOSH injury). Due to its restricted blood supply and inadequate collateral circulation, the proximal pole of the scaphoid bone is particularly subject to avascular necrosis in the event of fractures across the scaphoid waist.
During pincer grasps, axial stress of the thumb, and radial-sided wrist discomfort and soreness in the anatomical snuffbox are frequent presentations of scaphoid fractures. Although radiographic imaging is typically used to diagnose them, a CT scan may be necessary to determine the exact nature of the fracture. Non-displaced fractures, however, can occasionally go unnoticed because of the uneven shape of the bone or even because of faint fracture lines. Bone scintigraphy or MRI may be utilized to confirm the diagnosis in certain situations.
The location of scaphoid fractures and whether or not bone displacement determine how they should be treated. Distal pole scaphoid fractures can be treated conservatively, whereas proximal pole fractures need to be surgically corrected. Because of the higher risk of nonunion associated with displaced fractures, headless compression screw fixation surgery is necessary for the quickest healing and return to sports. Non-displaced fractures are managed by immobilizing the cast.
The Hamate Fracture Hook
Direct strikes, such as “checking” a baseball bat or “grounding” a golf club, are the typical causes of these fractures. They mostly feel muscle pain, soreness in the hypothenar muscles, and paresthesias in the ulnar nerve area. The current standard of treatment is still to remove the hamate fragment’s hook, which has led to good outcomes and a six-week return to sports.
Lunate Displacement
Owing to the lunate’s proximity to the median nerve, anterior displacement of the bone may result in mechanical compression of the nerve within the carpal tunnel, causing symptoms and signs that are typical of neuropathy caused by the median nerve, including weakness and atrophy of the thenar eminence and paresthesias of the first three and radial halves of the fourth fingers.
In addition, ligament injuries may potentially alter the anatomic connection of the carpal bones, leading to the development of two different forms of instabilities: volar intercalated segmental instability (VISI) and dorsal intercalated segmental instability (DISI).
FAQs
What are the 8 carpal bones?
The proximal and distal rows include the two rows of the eight carpal bones.
From radial to ulnar:
Proximal rows: Triquetrum, lunate, scaphoid, and pisiform.
the distal rows are: The hamate, trapezium, trapezoid, and capitate.
What is pisiform?
The wrist joint comprises eight carpal bones, one of which is the pisiform. The name pisiform comes from the Latin terminology where “pea” (Pisum) shape. On the anteromedial side of the wrist, it is palpable. Though it adds to wrist stability, it is considered a sesamoid bone.
Which carpal bone is most injured?
Scaphoid fractures are by far the most common type of fracture, accounting for nearly 55% of carpal fractures and over 10% of hand fractures.
Reference :
- Bair, M. M., & Gondal, A. Z. (2023, July 31). Anatomy, Shoulder and Upper Limb, Forearm Radius. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK544512/
- Rohit, B. (2023a, March 30). Carpal bone – Structure, Function, Movement – Samarpan Physio. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/carpal-bone/

3 Comments