Patellar Fracture
Introduction
A patellar fracture, commonly known as a broken kneecap, is a disruption of the patella, the small bone that sits at the front of the knee joint.
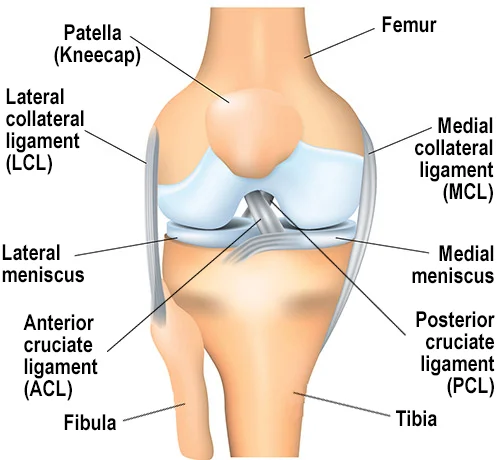
The largest sesamoid bone in the human body is called the patella. The thickest layer of cartilage in the body is found on the posterior portion of the patella. The articular surface’s medial and lateral facets are divided by a vertical ridge, which also articulates with the femoral tendons.
In addition to acting as the quadriceps tendon’s insertion point and a fulcrum to enhance the extensor mechanism’s efficacy, the patella guards the anterior aspect of the knee joint.
The patella tendon is where the inferior pole of the patella is attached. The vastus lateralis, vastus medialis, and fascia lata all contribute to the formation of the patellar retinaculum. The geniculate arteries supply the patella with centripetal blood flow; the superior vessels are located anterior to the quadriceps tendon, and the inferior vessels are located posterior to the tendon of the patella. The patella’s main blood supply enters the inferior pole through the fat pad beneath the patella.
Causes of Patellar Fracture
Direct or indirect forces can cause patellar fractures, and the manner of damage frequently determines the fracture pattern. Indirect failure of the patella most frequently occurs under strain. The extensor mechanism’s eccentric forces may be excessive for the bone’s mechanical characteristics. A hit to the anterior knee, such as from a fall or impact from the dashboard in a car accident, may cause a direct damage because of the patella’s subcutaneous site.
Periprosthetic patella fractures will probably happen as a result of the demand for primary total knee arthroplasty, which will rise to 3.48 million procedures performed in 2030—a 673% increase from 2005. Periprosthetic fractures have increased concurrently with a longer lifespan, higher activity demands on patients, and a growing requirement for total knee arthroplasty.
Complex issues like periprosthetic fractures require in-depth preoperative discussions with the patient and their family, a full history, and intensive surgical preparation. Periprosthetic fractures are similar to native patella fractures in that they are caused by direct trauma or eccentric stress through the patella or quadriceps tendon.
Epidemiology:
Approximately one percent of all fractures are patellar fractures. Males are more likely to experience them. Because of their high-energy mechanism, open injuries frequently occur in conjunction with other injuries and comprise 6% to 9% of patellar fractures. A divided patella is caused by a tiny percentage of individuals in which a secondary ossification center in the patella fails to fuse. This occurs most frequently near the superolateral patellar edge. Radiographs might indicate them as a fracture. The bipartite patella is present in both knees in half of the people with this disease.
Patella periprosthetic fractures are the most common complication after total knee arthroplasty, and they can be serious injuries. Periprosthetic patellar fractures were shown to be 0.68% common after 12,000 initial total knee arthroplasties were examined over a thirteen-year period by the Mayo Joint Registry. Compared to intraoperative fractures, postoperative periprosthetic patella fractures occur more frequently. When compared to primary total knee arthroplasty, the rate of postoperative periprosthetic patella fracture (1.8%) and intraoperative patella fracture (0.2%) is twice as high in revision total knee arthroplasty with patellar component substitution. Timing (intraoperative or postoperative) determines the classification of periprosthetic fractures, which are further divided into subclasses based on factors such as displacement, bone stock adequacy, patella component stability, and extensor mechanism competence.
Pathophysiology:
Loading patterns are dynamic and complex for the patella. The pull of the quadriceps causes the patella to become tense when the knee is extended. Conversely, when the knee is bent, compressive stresses are placed on the posterior patella. During knee flexion, the quadriceps and patellar tendons also apply compression and 3-point bending stresses to the patella. The patella may fail in compression due to the 3-force bending forces if there is fast knee flexion during an aggressive quadriceps contraction.
Avulsion fractures of the inferior pole or transverse fractures extending into the extensor retinaculum, causing fracture displacement, are frequently the result of indirect eccentric strain through the extensor mechanism. Despite significant fracture comminution and cartilage loss, the retinaculum and extensor mechanism frequently survive direct patellar fractures.
Periprosthetic patellar fractures are categorized as either intraoperative or postoperative depending on when they occur. Predisposing factors related to their pathophysiology are present in postoperative periprosthetic patellar fractures, which are more common than intraoperative fractures. Revision arthroplasty, excessive force applied to the patella clamp, extensive reaming of the patella (less than 10 to 15 mm of remaining bone stock), anterior perforation during preparation, and thermal necrosis after cement application are all potential causes of intraoperative periprosthetic patellar fractures.
There are two types of postoperative periprosthetic patellar fractures: traumatic and atraumatic. The causes of trauma are comparable to those mentioned in cases of native patellar fractures. Implant selection, patient characteristics, and surgical technique all contribute to the atraumatic mechanism of fractures. Reuben advocated for the retention of a well-positioned and little-used prosthesis during revision total knee arthroplasty and suggests against the revision to a new patellar component if less than 10 mm of bone stock is left. In 504 primary total knee arthroplasties, periprosthetic patella fractures occurred 3.5% of the time, according to Tria et al. Of those, a lateral release was connected to all of the periprosthetic patellar fractures. Lateral release may damage the primary circulatory supply to the patella and risk the superior lateral geniculate artery. Osteolysis and patellar loosening.
Postoperative stress failure of the patella is commonly associated with inadequate reaming, in contrast to intraoperative periprosthetic patellar fractures associated with active reaming. Abnormal tension is placed on the patella and stress failure is predisposed when the patellofemoral joint is overstretched with a patellar prosthesis larger than the bone removed or an excessively large femoral component. A major factor in patella tracking during index arthroplasty is component malpositioning. A postoperative fracture can result from patellar maltracking, which puts excessive strain on the patella. The risk of periprosthetic patellar fracture is influenced by the implant that the surgeon chooses for the index arthroplasty.
Postoperative fracture is related to patellar prosthesis with single or large central pegs, metal backs, and press-fit insertions. While the huge central peg requires additional bone excision for implantation, the single central peg causes stress risers. Metal-backed parts are prone to failure because they raise the contact stress across the patellofemoral joint.
Male sex, inflammatory arthritides, insufficient bone stock, osteopenia/osteoporosis, and greater activity level are patient variables linked to periprosthetic patellar fractures. Because males tend to weight more and be more active, they experience increased patellofemoral stress.
Seven common fracture types were identified by the original classification of patellar fractures: nondisplaced, transverse with displacement, inferior pole, comminuted without displacement, comminuted with displacement, vertical, or osteochondral. This system’s descriptive design offers suggestions for the cause of harm, but it does not prescribe a course of therapy or offer prognostic data.
Extra-articular fractures (avulsion or isolated body fractures) are categorized as 34A in the AO/OTA classification of patellar fractures. 34B is the classification for vertical partial articular fractures. Total articular fractures are categorized as 34C and classified according to the degree of comminution.
The stability of the patellar prosthesis, the extent of fracture displacement, the position and pattern of the fracture, the quality of the bone stock, and the extensor mechanism’s competency are the main factors used to classify periprosthetic patellar fractures.
Although there isn’t a single, widely recognized categorization for periprosthetic patellar fractures, Ortiguera and Berry created one that might be utilized to determine the course of care. While Type II and III fractures frequently require surgical intervention, extensor mechanism repair or reconstruction, and revision of the patellar prosthesis, Type I fractures are typically managed non-operatively.
Classification of Periprosthetic Patellar Fractures by Ortiguera and Berry:
- Type I: Rigid extensor mechanism and stable implant
- Type II: Extensor mechanism disruption
- Type IIIa: Reasonable bone stock, loose patellar component
- Type IIIb: Insufficient bone stock and a loose patellar component
Symptoms of patellar fracture:
There are two types of patella fractures displaced or non-displaced. Because they are unequal, displaced fractures can also be categorized as:
Comminuted:
Can lead to damage to the articular cartilage of the patella and femoral condyles as a result of a direct hit (mostly from blows or falls on a knee when the knee is flexed).
Stellate or transverse:
caused by intense muscle contraction or excessive strain on the extensor mechanism; an example of this would be an explosive contraction of the quadriceps following a jump from a height.
The most common type
There could be a problem with proximal blood circulation.
usually as a result of knee hyperflexion.
Marginal:
- When the knee is flexed, the reason for a fall on the knee
- either horizontal or vertical
- either the upper or lower pole
- Osteochondral
- Sleeve (for patients only in their childhood)
- The degree of chondral damage present at the moment of injury determines the injury’s prognosis. The attainment of a pain-free and stable range of motion during the early phase is crucial for achieving a functional outcome.
Types of Fracture of patellar fracture:
The varieties of patellar fractures that might occur are characterized by medical professionals at NYU Langone. A fracture of the patella is one of the most unique types. A fracture can occur in any part of the patella and range in severity from a tiny crack to one that breaks the bone into separate pieces.
A broken patella can cause severe pain around the kneecap, especially while flexing the knee. There may be redness and swelling in the area around the injured knee. Many people who receive care from an orthopedist go on to fully heal and regain function of their knees.
Closed Fracture:
Among all patella fractures, closed fractures—in which the patella does not pass through the skin—are among the most common. Without surgery, a number of closed fracture types can be managed.
Open Fracture:
When a fractured bone breaks through the skin to show the injured patella, it is known as an open fracture. A correction surgery and quick emergency care are necessary for an open fracture of the knee. An open fracture may require more time to heal and frequently involves harm to the surrounding soft tissues.
Open fractures are particularly dangerous because there is a higher risk of infection in both the bone and the wound after the skin is broken. To prevent infection, treatment must be started right away.
Nondisplaced Fracture:
This kind of fracture does not move. The fractured bone fragments might continue to be joined. When a fracture is stable, the bones usually stay in place while the patient heals. Closed fractures are often those that are not displaced.
Displaced Fracture:
A fracture type known as a misplaced fracture occurs when the patella breaks into two or more fragmented pieces that do not remain together. Any part of the patella is susceptible to this type of fracture, and the bone may break horizontally or vertically. There are two types of displaced fractures: closed and open.
Osteochondral, comminuted, and simple fractures are examples of displaced fractures. In many cases, this type of fracture requires surgery in order to reconstruct the broken bone.
Simple Fracture:
- A simple patella fracture is a closed fracture in which the bone breaks into two pieces. It can be easily repaired in its original location or it can be nondisplaced.
Comminuted Fracture:
A fracture of the patella where the bone is broken into more than two or more fragments is called a comminuted fracture. A fracture that has been comminuted may be closed or open. Some of your bone fragments may be too small to rejoin after an open comminuted fracture and may need to be removed during surgery.
Osteochondral Fracture:
The layer of cartilage beneath the patella, where it joins the other bones in the knee joint, is another area a displaced fracture can occur. To prevent bones from rubbing against one another while moving, cartilage, a soft substance, lines the ends of the bones in joints. An osteochondral fracture is the term used to describe the injury to this cartilage and the underlying bone. This kind of injury is typically a closed fracture. Acute patellar dislocation is closely associated with osteochondral fractures of the patella. These can result from both noncontact twisting damage to the knee and traumatic-type injuries to the knee.
All types of patella fractures have the potential to cause cartilage damage, which can lead to additional issues such as osteoarthritis, a degenerative disease of the joint characterized by cartilage loss. An individual with osteochondral fractures is more likely to develop osteoarthritis of the knee because these fractures continue to affect the cartilage in the knee joint.
Differential diagnosis:
- Bipartite patella
- dislocation of the knee
- Dislocation of the patella
Diagnose:
- Information about the accident
- Injury mechanism
- There is knee pain.
- complaints about being unable to stand or make a knee crack sound.
Physical examination:
Observation:
- Complete limb
- A bruised, swollen knee
- abnormality located around the knee
- Possible injuries (open fractures)
- Palpation (often performed later to lessen pain with local anesthetics):
- sensitivity at the patella
- Palpable space (in case of misplaced fractures).
Discard any concurrent injuries,
such as tibia, femur, and acetabulum fractures.
Hemarthrosis
Range of motion:
Acute:
Minimal discomfort in the knees during flexion and extension
Often incapable of performing a straight leg raise
Chronic:
- Complete knee flexion with latency in extension
- distant pulses
- Examine the leg’s compartment.
- neurological evaluation
Special investigations:
X-rays:
- AP view: It could be difficult to see the patella in the back view:
- Undisplaced—distance of more than 2 mm
- Displaced; step deformity observed; more than 2 mm separation
- View of the sky
- used to regularly check on the healing process and any possible problems.
CT scan:
Typically not required
MRI:
Identification of associated damage to surrounding ligaments and tendons
Bone scans:
to identify fractures caused by stress
Outcome measures:
- Osteoarthritis outcome score and knee injury
- survey of knee outcomes
- Scale of lower extremity function
- McGill Pain Questionnaire
Medical Treatment:
Regional anesthetics can be used to relieve pain in severe situations. This aims to help in the patella fracture examination and diagnosis.
- Conservative management: Used: Non-displaced fractures with an extensor mechanism in place that occur frequently in the vertical, horizontal, and comminuted types
- Management: For four to six weeks, the fracture is immobilized with a POP cylinder cast or a range-of-motion brace locked in the extension position.
- Gradually, knee flexion can be improved as healing progresses.
- Wearing a range-of-motion brace is crucial until there is union (on X-rays) and clinical healing indicators (not painful to the touch).
- 6–8 weeks of crutch walking
- Rehabilitation to fully regain strength, range of motion, and functionality.
Surgical intervention:
Significant displacement with fracture displacement greater than 1 to 4 mm or unbroken articular step off more than 2 to 3 mm when using the extensor mechanism.
Objectives: Realign articular incongruities, restore extensor function, and allow for beginning movement
- Management: Transverse, comminuted type fracture: ORIF connects the fractured sections by applying Fig. of 8 techniques and the tension band wire technique with pins and wires.
- POP cast in a six-week extension position
- Greater than 1/3, either proximal or distal, simple or comminuted: tendon repair and tiny portion excision
- POP cast for a period of six weeks
- Unusual longitudinal data: Interfragmentary attaching of screws
- Comminuted fracture, simple or irreversible fracture, or excessively injured cartilage: Whole and partial.
- Patellectomy: During a total patellarectomy, the quadriceps muscles, which are linked to the patellar ligament, enable the extensor appliance to operate.
- Patellectomy: outdated methodology, with the option’s last treatment lacking much in extension
- bilateral vastus muscle repair
- Rehabilitation is the same as under the previously mentioned conservative management.
- Later stages: When arthrofibrosis occurs, manipulation while under anesthesia or arthroscopic adhesion, and release are required.
Physical therapy:
The physician will direct rehabilitation while taking the results of the X-ray into account, since clinical healing phases do not always correspond with theoretical recovery. Here is an example of how to restore a patient following a patella fracture. It is always enjoyable to talk about treatment plans with the orthopedic physicians who referred the patient.
- Conservative management: If the extensor mechanism is still intact, conservative management should be used.
Phase 1: 0-6 weeks
Range of motion, in the surgeon’s opinion:
- For two to three weeks, the range-of-motion brace was locked in the extended position.
- brace for controlled mobility at two to three weeks
- Exercises: Focus on active flexion and extension in internal ranges; begin open kinetic chain strengthening and knee range of motion at three to four weeks.
- The quadriceps
- Hamstrings tighten SLR
- Dynamically closed and open chains exercises that strengthen the hips
- circulatory drills
Weight-bearing:
- Wearing a brace while partially bearing weight
- Maybe in tandem
- Limitations on load bearing typically used for 7-8 weeks
- The duration of crutches or restrictions on weight bearing in accordance with orthopedic Patella mobilization
- Cryotherapy for the management of pain and edema
Phase II: 6-12 weeks
- knee brace with range of motion according to orthopedics Range of motion: Improvement of total knee flexion and extension
- Exercises: stationary bike with no resistance and a raised seat
- progression of closed kinetic chain workouts, such as step-ups, retro steps, and mini squats
- Increase the resistance when performing hip workouts.
- The sense of proprioception
- Weeks 8–10: Lunges
knee brace with range of motion according to orthopedics Range of motion:
- Improvement of total knee flexion and extension
Exercises:
- stationary bike with no resistance and a raised seat
- progression of closed kinetic chain workouts, such as step-ups, retro steps, and mini squats
- Increase the resistance when performing hip workouts.
- The sense of proprioception
- Weeks 8–10: Lunges
Post-operative rehabilitation:
When there is a noticeable displacement and the extensor mechanism is intact, surgery is performed. The preferred course of action is typically open reduction and internal fixation using the tension band wire technique.
Phase I: 0-2 weeks
- Brace range of motion: Locked-in extension position (in the event that a POP cast is not suggested)
- For the purpose of physical therapy sessions, a knee flexion range of 0 to 30 degrees is initially allowed.
- Mobilization: Range-of-motion brace used to lock the knee in extension.
- Exercises: Strengthening of the isometric quadriceps, hamstrings, and abductors
- resisted ankle exercises (with a TheraBand, for example)
Phase II: 2-6 weeks
- ROM brace (if appropriate): To be secured in an extension and used during weight-bearing exercises
- Maybe taken out at night
- Range of motion: To reach 90 degrees in one week, add 5 degrees of flexion each week. Six Workouts
- Strengthening of the isometric quadriceps, hamstrings, and abductors
- Resistance training for the ankles (e.g. with theraband)
- Start the SLR
Phase III: 6-10 weeks
- Flexibility of movement brace;
- Unlocked; to be worn while bearing weight
- Range of motion: By week 10, progress to the complete range of motion.
- Exercises: Same as in the earlier stage
Phase IV: 10-12 weeks
- Brace for range of motion: Avoid
- Range of motion: Full
- Activities: As in the earlier stage
- Start with stationary cycling.
Phase V: Up to 3-6 months
- As permitted, begin your regular activities.
Complications of Patellar Fractures:
Some patients with patellar fractures may face long-term problems even after receiving successful treatment.
Post traumatic Arthritis:
One kind of arthritis that appears after an accident is called posttraumatic arthritis. Even in cases when your bones heal properly, over time discomfort and stiffness may result from damage to the articular cartilage that covers your bones. A tiny proportion of people who have patellar fractures go on to develop severe arthritis. Much more prevalent is chondromalacia patella, a disease characterized by mild to moderate arthritis.
Muscle Weakness:
Following a fracture, certain patients may experience lifelong weakness in the quadriceps muscle located in the front of the leg. It is also typical to have some loss of knee range of motion, including flexion (bending) and extension (straightening). Usually, this loss of mobility is not crippling.
Chronic Pain:
Patellar fractures can result in ongoing discomfort in the anterior region of the knee. Although the exact etiology of this pain is unknown, posttraumatic arthritis, stiffness, and muscular weakening are probably factors. Some patients discover that wearing a knee brace or support makes them more comfortable.
Summary:
Following a patellar fracture, recovery times vary depending on several factors, such as:
- The severity of your injury
- Whether surgery or non-surgical treatment was used for you
- The length of time required for recovery
- In three to six months, the majority of patients will be able back to their regular activities. It could take longer for people with serious fractures to resume their normal activities.
To preserve your knee and prevent more issues, your doctor could advise making certain lifestyle adjustments. This may include staying away from exercises that require frequent deep knee bends or squats. Additionally, you should refrain from walking on steep inclines and using ladders or stairs.
FAQs
How severe a fracture of the patella is?
Broken Kneecaps: Patellar Fractures
A serious injury that can make it difficult or impossible to walk or straighten your knee is a patellar fracture. Wearing a cast or splint until the bone heals can be the treatment for certain mild patellar fractures. However, in most cases of patellar fractures, the broken bones move about throughout the trauma.
If you had a patellar fracture, could you still walk?
signs of a fractured patella
Anatomically, the quadriceps femoris, or thigh muscles, are connected to the patella. These muscles are essential for walking and aid in leg straightening. The interruption in this link could make it impossible for the person to walk or bend their knee.
How should a fractured patella be treated?
Without surgery, this kind of fracture typically heals well. Your physician will immobilize your knee in extension using a cast, hinged knee brace, or knee immobilizer if they decide you don’t require surgery. You are free to carry as much weight as you feel comfortable with.
What is the initial treatment for a fractured patella?
Apply ice to your knee. To make an ice pack, place ice cubes into a plastic bag and cover it with a cloth. Use the ice pack for 10 to 15 minutes every hour on the first day of the injury. Ice the region every three to four hours for two or three days after the initial day, or until the pain subsides.
Can surgery be used to repair a patella?
Wearing a cast or splint until the bone heals can be the treatment for certain mild patellar fractures. However, the majority of patellar fractures result in the bone fragments shifting during the injury. Kneecap repair requires surgery for these more complex fractures.
How is a patella fracture fixed?
To fix a fractured kneecap, two surgical procedures can be used: Procedures for open reduction-internal fixation (ORIF): The surgeon makes an incision in the skin and uses metal wires, pins, or screws to reattach the damaged bones. Broken bone fragments that are too little to be repaired are taken out.
Does a person need a patella to walk?
Even while it is theoretically feasible to walk without a kneecap, doing so would probably result in severe discomfort. Your leg’s bones would directly contact with one another, resulting in friction and inflammation.
Painful patellar surgery?
You will be in pain, but it should be bearable. There may be a tiny amount of drainage at the surgical site the first few days, this is NORMAL and caused by the joint being filled with fluid during the surgery. In two to three days, the swelling will subside.
What occurs if a fractured patella is not treated?
If a bone fracture is not treated, it may result in a malunion, in which the bone heals improperly, or a nonunion, in which the bone heals partially but stays broken. Both will permit decline in function, discomfort, and edema over time.
When following a patella fracture may you start walking?
The majority of patients who have patella fractures heal rather well and are able to walk again. Patients typically feel very comfortable by six weeks, and after three months, they are usually allowed to return to full activities including manual labor, skiing, and motocross.
What kind of patella fracture occurs most frequently?
A straightforward two-part diversion brought on by a direct strike is the most typical fracture pattern (i.e. dashboard injury). The knee joint’s extensor mechanism may become insufficient due to a bony lesion.
Is surgery on the patella successful?
A recurrence of instability may happen during specific activities and necessitate further treatment. Nonetheless, the outcomes are positive since more than 80% of patients show improvements in pain and knee function, and more than 90% show patella stabilization.
What is the need for patellar surgery?
Surgery is typically necessary for displaced fractures, which result in many fractured fragments of the patella that have split apart. Furthermore, in the event that any of the bone pieces have created an open fracture—a break in the skin—surgery is usually arranged right once.
After having patellar surgery, can I sleep without a brace?
After surgery, we advise wearing a post-operative knee brace for two to three weeks. After the first week, you do not need to sleep with this brace on. The rehabilitation process takes about six months in total. This amount of time is required for the MPFL ligament to develop to the stage where Dr.
Reference:
- Luo, T. D.,Marino,D. V., & Pilson, H. (2023, July 31). Patella Fractures.StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK513330/
- Physiotherapist, D. (2023, April 28). Patellar Fractures – Type, Symptom, Treatment – Samarpan Physio. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/patellar-fractures/
- Patellar Fractures (Broken Kneecap) – OrthoInfo – AAOS. (n.d.). https://orthoinfo.aaos.org/en/diseases–conditions/patellar-kneecap-fractures/