Trochlear nerve
Introduction
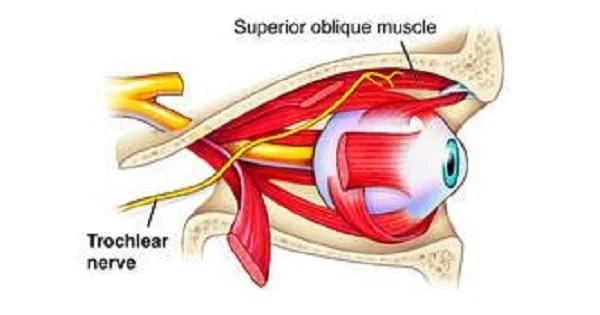
The trochlear nerve, or fourth cranial nerve (CN IV), acts as one of the ocular motor nerves that regulate eye movement. As the only cranial nerve with a dorsal outflow from the brainstem, the trochlear nerve, despite being the smallest, has the longest intracranial path.
It starts in the midbrain and travels laterally and anteriorly to the superior oblique muscle. This muscle allows you to lower your eyeball and shift your gaze from side to side.
The word “trochlear nerve” comes from the Latin word Trochlea, which means “pulley.” This name describes the way your nerve interacts with your superior oblique muscle to rotate your eye downward, as well as the connective tissue sling that encases a portion of the nerve.
The trochlear nerve is the only cranial nerve that leaves the brain through the back. As a result, this nerve covers the greatest distance through the cranium.
Anatomical Course
The trochlear nerve emerges from the posterior aspect of the midbrain and has its origin in the brain’s trochlear nucleus.
It passes through the subarachnoid space anteriorly and inferiorly before puncturing the dura mater close to the sphenoid bone’s posterior clinoid process.
The nerve then travels along the lateral wall of the cavernous sinus (along with the oculomotor nerve, the abducens nerve, the ophthalmic and maxillary branches of the trigeminal nerve, and the internal carotid artery) before entering the orbit of the eye through the superior orbital fissure.
Embryology
The trochlear nerve, like the abducens (VI), hypoglossal (XII), and oculomotor (III) nerves, is a ventral root of the spinal nerves. These cranial nerves originate in the brainstem’s somatic efferent columns. In early skeletal muscle development, the cranial (preoptic and occipital) myotomes give rise to the muscles they innervate.
During the fourth week of development, the neural tube is made up of three primary vesicles: prosencephalon, mesencephalon, and rhombencephalon. The mesencephalon eventually develops into the midbrain. The trochlear nerve originates in the posterior midbrain. From here, the nerve runs ventrally to innervate the superior oblique muscle.
Blood Supply and Lymphatics
The basilar artery, superior cerebellar artery, and posterior cerebral artery all supply blood to the midbrain. Because cranial nerve IV contains a motor nucleus, it is situated near the midline along the medial longitudinal fasciculus. The disruption of any of the previously mentioned arterial structures could impact the trochlear nucleus as well as the medial midbrain.
Function
General somatic efferent impulses from the trochlear nerve synapse in the skeletal fibres of the superior oblique muscle. The eyeball can be made to rotate (intort) medially, abduct, and be depressed thanks to the superior oblique muscles. Although the superior oblique muscle is situated behind the eyeball, its tendon approaches it from the front, guided by the trochlea.
At a 51-degree angle to its normal position, the tendon connects to the superior aspect of the eyeball, which is where one looks straight ahead. As a result, the tendon’s pull is divided into two parts: a forward component that pulls the eyeball downward (depression) and a medial component that rotates the top of the eyeball towards the nose. The relative intensity of these two forces varies depending on where the eye looks.
- When the eye is adducted (looking towards the nose), the depression becomes more intense.
- The force of intorsion increases but the force of depression decreases when the eye is abducted or turned away from the nose.
In the primary position (looking forward), superior oblique contraction results in approximately equal amounts of depression and intorsion.To summarise, the superior oblique muscle causes:
- Eyeball depression occurs, particularly when the eye is adducted.
- Eyeball intorsion happens, especially when the eye is abducted.
Trochlear nerve palsy
The fourth cranial nerve regulates the superior oblique muscle, an external eye muscle. The muscle extends from the back of the eye socket to the top of the eye. It goes through a loop of tissue near the nose called the trochlea. It directs the eye inward and downward.
The fourth cranial nerve is the only one that originates at the back of the brain. Compared to other cranial nerves, it passes through the skull the furthest. It enters the eye socket from the back and travels to the superior oblique muscle.
Diseases or injuries to the fourth cranial nerve can paralyze the superior oblique muscle. The term for this condition is fourth nerve palsy. It’s also called superior oblique palsy or trochlear nerve palsy.
Fourth nerve palsy can occur at birth or develop later in life. It usually affects only one eye, but it can occur in both.
Causes of Trochlear nerve palsy
A variety of medical conditions can affect the trochlear nerve, including:
Congenital conditions. Fourth nerve palsy can be congenital, which means that it can be present at birth.
Trauma. Fast and jerky head movements can damage the delicate trochlear nerve. Such an injury can occur during car accidents or other incidents that cause whiplash.
Guillian-Barre Syndrome. This poorly understood syndrome develops when your immune system attacks your nerve cells, resulting in numbness, temporary paralysis, and other symptoms. However, many people do recover completely from this syndrome.
Lyme Disease. Ticks transmit this bacterial infection to humans through their bite. This disease has a variety of symptoms, including facial drooping and vision problems.
Meningioma. This type of cancer causes slow-growing tumours to form on the meninges, which are layers of membrane that cover the brain. A tumour pressing on the trochlear nerve can result in fourth-nerve palsy.
Shingles. Individuals who have chickenpox may develop shingles afterward. This disease presents as a painful rash that can cause long-term pain.
Some of these conditions can be fatal, so if you develop fourth nerve palsy, seek medical attention right away.
Symptoms of Trochlear nerve palsy
The most common symptom of fourth nerve palsy is double vision (diplopia). It only happens when both eyes are opened. With one eye closed, you only see one image. But if you open both eyes, you might see two images. One image may appear to be above or to the side of the other. Some people may notice that one image appears slightly turned in comparison to the other. If there is little space between images, the overall image may appear blurry rather than double.
Additional symptoms may include:
- One iris is higher than the other. The coloured portion of the eye is called the iris.
- Holding your head tilted. This is intended to help with the vision problem.
- Pain, typically above the brow. This can occur if the fourth nerve palsy is idiopathic or associated with diabetes.
- If you’ve had palsy for a while, your brain may have learned to ignore images from that eye. If this is the case, you might not have double vision.
Assessment
Superior oblique weakness is a clinical indicator of CN IV palsy. When this muscle works independently, it depresses and abducts the eyeball. In contrast, the extraocular muscles work together to move the eye. Because the superior oblique contributes most to this motion, the trochlear nerve is tested by having the patient look “down and in.” Convergent gaze is needed for two common hobbies: reading the newspaper and taking the stairs. When CN IV palsy is present, diplopia is a crucial symptom that must be addressed.
Diagnosis
A doctor may order tests to differentiate fourth nerve palsy from other conditions. This may include:
- Blood tests to detect autoimmune diseases and thyroid hormone levels
- CT scan or MRI, to examine your brain and cranial nerves.
- Ultrasound, to examine the muscles of the eye.
- Spinal tap (lumbar puncture) to look for causes of elevated intracranial pressure.
- Nerve stimulation tests.
Your medical professional may refer you to an ophthalmologist for diagnosis and treatment. You may even need to consult a neuro-ophthalmologist. This is an eye doctor who has received specialised training in treating eye nerve problems.
Differential diagnosis
- Oculomotor palsy.
- Guillain-Barre Syndrome
- Orbital Pseudotumor – Brown Superior Oblique Tendon Sheath Syndrome
- Fisher Syndrome
- Botulism
- Chronic progressive external ophthalmoplegia (CPEO).
- Vertical one-and-a-half syndrome
- Monocular Supranuclear Gaze Palsy
- Myasthenia Gravis: Ocular Tilt Reaction or Skew Deviation
- Thyroid Eye Disease.
Treatment
Trochlear nerve palsy treatment is determined by the underlying cause. Idiopathic fourth nerve palsies usually go away on their own. Palsies caused by injury can also improve over time. If something is pressing on your fourth cranial nerve, you may require surgery to relieve the pressure.
Possible treatments for fourth nerve palsies include:
- Over-the-counter pain medications and prism glasses. These can combine the double images into a single image.
- Eye patch. You alternate between one eye and the other to prevent one eye from becoming weak or lazy.
- Surgery to realign the eyes.
The goal of surgery is to eliminate the double vision. This can also help with the tendency to tilt your head. If your vision problem is severe, you may require surgery on both eyes.
Prevention
Congenital trochlear palsy and associated injuries are frequently unavoidable. However, you can protect this important nerve using a few simple strategies, such as:
- Adding safety equipment like baby gates or grab bars to your home to protect infants and the elderly from falls that may result in head injuries.
- Using a seatbelt in the car reduces your odds of experiencing whiplash during a collision.
- Wearing a helmet during physical activities that can cause a head injury, such as playing football or riding a bike.
- Protecting your head and neck from injury will help you keep your trochlear nerve healthy and your vision intact.
Summary
The trochlear nerve, also known as the fourth cranial nerve (CN IV), is a vital ocular motor nerve that regulates eye movement. Originating in the brain’s trochlear nucleus, it travels through the subarachnoid space and the dura mater before entering the orbit of the eye through the superior orbital fissure.
The trochlear nerve is the mainly cranial nerve that exits the brain via the back and travels longest through the cranium. Its function is to regulate the superior oblique muscle, which allows the eyeball to rotate, abduct, and be depressed. The trochlear nerve is situated near the midline along the medial longitudinal fasciculus, and disruptions in arterial structures can impact it.
Trochlear nerve palsy, also known as superior oblique palsy or trochlear nerve palsy, is a condition where the superior oblique muscle is paralyzed by diseases or injuries to the trochlear nerve. Symptoms include double vision, iris elevation, head tilting, and pain. The trochlear nerve is tested by having the patient look “down and in” to assess the condition.
Fourth nerve palsy is a condition characterized by double vision, often caused by autoimmune diseases or injury. Diagnosis involves tests like blood tests, CT scans, MRIs, ultrasounds, spinal taps, and nerve stimulation tests. Treatment depends on the underlying cause and may include pain medications, eye patches, or surgery. Prevention strategies include using safety equipment, seatbelts, and helmets to protect the nerve and maintain vision.
FAQs
What’s another name for the trochlear nerve?
The trochlear nerve is the fourth Cranial Nerve (CNIV) and has the longest intracranial course while also being the thinnest. On the other side of its origin, it has a general somatic efferent (somatic motor) nerve that innervates one muscle (superior oblique).
What disease affects the trochlear nerve?
Diseases or injuries to the fourth cranial nerve can paralyse the superior oblique muscle. The term for this condition is fourth nerve palsy. It’s also called superior oblique palsy or trochlear nerve palsy. Fourth nerve palsy can occur at birth or develop later in life.
What constitutes a trochlear nerve disorder?
Patients with trochlear nerve palsy complain of double vision vertically (vertical diplopia) or images that are tilted or rotated. The diplopia is binocular and can deteriorate or improve with different gazes.
Where is the trochlear nerve located?
The trochlear nerve arises through the posterior aspect of the midbrain and has its point of origin in the brain’s trochlear nucleus.
What is the treatment for the trochlear nerve?
Oculomotor exercises and prism glasses can help restore concordant vision. If the palsy does not resolve, surgery, particularly for congenital strabismus, may be required.
Which cranial nerve is the smallest?
The trochlear nerve is the smallest cranial nerve. It comes from the surface of the midbrain.
References:
- Kim, S. Y., Motlagh, M., & Naqvi, I. A. (2023, July 15). Neuroanatomy, Cranial Nerve 4 (Trochlear). StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK537244/
- Professional, C. C. M. (n.d.). Trochlear Nerve. Cleveland Clinic. https://my.clevelandclinic.org/health/body/21816-trochlear-nerve
- The Trochlear Nerve (CN IV) – Course – Motor – TeachMeAnatomy. (2019, March 13). TeachMeAnatomy. https://teachmeanatomy.info/head/cranial-nerves/trochlear-nerve/
- Trochlear Nerve. (n.d.). Physiopedia. https://www.physio-pedia.com/Trochlear_Nerve
- Cranial Nerve 4 Palsy – EyeWiki. (n.d.). https://eyewiki.aao.org/Cranial_Nerve_4_Palsy
- Articles. (n.d.). https://www.cedars-sinai.org/health-library/diseases-and-conditions/f/fourth-nerve-palsy.html
- Anderson, B. (2022, December 13). Trochlear Nerve: What To Know. WebMD. https://www.webmd.com/brain/trochlear-nerve-what-to-know



One Comment