Teres Minor Muscle
The teres minor muscle is a small yet vital muscle located in the posterior shoulder region. Together with the infraspinatus muscle, it forms part of the rotator cuff, a group of muscles and tendons crucial for stabilizing and providing mobility to the shoulder joint.
The rotator cuff’s teres minor is an elongated, thin muscle. The word “teres” comes from the Latin word “rounded.” The muscle inserts at the larger tubercle of the humerus as well as the posterior side of the joint capsule.
What is the Teres Minor Muscle?
The teres minor’s main job is to control the deltoid’s motion, which keeps the humeral head from sliding upward while the arm is abducted. It also has the role of laterally rotating the humerus.
The teres minor is a muscle in the shoulder area that is thin and rather slender. It starts on the side of the scapula and goes all the way to the humerus. Regarding muscle hierarchy, the teres minor is superior to the teres major and lower to the infraspinatus muscle. Teres minor muscle fibers and infraspinatus muscle fibers can fuse at times. Most of the teres minor’s surface is covered by the deltoid and trapezius muscles, which are also deeply affected.
Stretching from the lateral edge of the scapula to the larger tubercle (or tuberosity) of the humerus, the teres minor is a small, intrinsic shoulder muscle. It is a part of the “rotator cuff,” a group of tendons and muscles that work together to maintain the glenohumeral joint. The lateral, or external, arm rotation at the shoulder is controlled by the teres minor.
Structure of Teres Minor Muscle
The teres minor originates from the scapula’s posterior surface, just next to the top portion of its lateral border. The muscle’s top fibers terminate in a tendon that attaches to the humerus’s greater tubercle and merges with the shoulder joint’s capsule. Just below the larger tubercle, the muscle’s lower fibers penetrate the humerus directly.
All three muscles have a similar oblique orientation, with the teres minor situated anterior to the teres major and inferior to the infraspinatus. The triceps brachii muscle’s long head is situated inferior to and perpendicular to the teres minor in its anatomical position. Deep to the deltoid muscle is the teres minor.
For the top two-thirds of its length, it originates from the dorsal surface of the axillary border of the scapula. Additionally, it originates from two aponeurotic laminae, one of which separates it from the infraspinatus muscle and the other from the teres major muscle.
Its strands extend laterally and obliquely upward; the bottom strands are put straight into the bone immediately below the impression, while the top strands finish in a tendon that is inserted into the lowermost of the three impressions on the greater tubercle of the humerus.
The function of Teres Minor Muscle
The teres minor, a rotator cuff muscle, aids in maintaining the humeral head (ball) in the shallow glenoid cavity of the scapula (socket), stabilizing the ball-and-socket glenohumeral joint. Additionally, the teres minor turns the arm at the shoulder joint externally or laterally. The teres minor is particularly important in supporting the shoulder during medial rotation to prevent anterior dislocation of the humerus since it is an antagonist muscle to medial rotation due to its status as a lateral rotator.
As components of the rotator cuff, the infraspinatus and teres minor adhere to the head of the humerus and aid in maintaining the humeral head in the glenoid cavity of the scapula. They cooperate with the posterior deltoid for adduction and external (lateral) rotation of the humerus.
In terms of motion, teres minor externally (laterally) turns the arm while it is in the anatomical position. There are several uses for the teres minor when the arm is raised.
Arm adduction
Adducting the arm from its abducted posture, Teres Minor works in unison with Teres Major, latissimus dorsi, and pectoralis Major. This action serves to facilitate throwing and pulling motions with the upper limbs over the head.
Arm external rotation
The teres minor, in conjunction with the infraspinatus, pushes the larger tubercle posteriorly, causing the arm to rotate externally, or laterally. In the preload phase of overhead movements (such as throwing), this action loads the force and supports the shoulder at the same time.
Origin
Teres minor begins in the scapula, where it emerges from two heads divided by the circumflex scapular artery’s groove. The attachment site extends across the upper two-thirds of the scapular lateral border. The fibers unite rapidly to form a solitary muscular belly that travels superolaterally in the direction of the proximal humerus.
Insertion
The teres minor attaches to the humerus’s larger tubercle. In particular, the muscle’s superior fibers release a brief tendon that attaches to the larger tubercle of the humerus’ inferior aspect. In contrast, the inferior fibers insert next to this, straight into the proximal shaft of the humerus, slightly distal to the superior portion tendon, and proximal to the lateral head of the triceps brachii origin.
Nerve Supply
The brachial plexus’ posterior cord gives rise to the axillary nerve, which is made up of nerve roots C5 and C6. The axillary nerve travels to the inferior edge of the subscapularis muscle after passing anterior to the subscapularis muscle and posterior to the axillary artery.
Here, it leaves the axilla posteriorly across the posterior circumflex humeral artery (PCHA), passing via the quadrangular area formed by the long head of the triceps brachii medially, the surgical neck of the humerus laterally, and the teres minor superiorly and inferiorly.
The axillary nerve splits into two terminal branches when it enters the posterior scapula; the teres minor is innervated by the posterior terminal branch.
Blood Supply
The posterior circumflex humeral artery and the circumflex scapular artery, one of the subscapular artery’s branches, supply the teres minor. The axillary artery’s third and farthest distal segment gives birth to the subscapular artery and the posterior circumflex humeral artery.
Lymphatics
The major branch of the axillary artery is the subscapular artery. It descends caudally and splits into the thoracodorsal and circumflex scapular arteries. The circumflex scapular artery passes between the teres minor and subscapularis along the lateral edge of the scapula.
It passes cranially through the triangle formed by the long head of the triceps brachii laterally, the teres minor superiorly, and the teres major inferiorly. It then enters the infraspinatus fossa, where it meets the scapular anastomosis. The teres minor is supplied by the circumflex scapular artery along its course.
A more distal branch of the third segment of the axillary artery is the posterior humeral circumflex artery. The teres minor superiorly, teres major inferiorly, the surgical neck of the humerus laterally, and the long head of the triceps brachii medially serve as its boundaries as it moves posteriorly via the quadrangular area beside the axillary nerve. After that, the artery supplies the shoulder joint by traveling anteriorly around the humerus’ surgical neck. The teres minor is supplied by the posterior humeral circumflex artery along its course.
Actions
- External rotation of the shoulder joint is the primary result of Teres Minor and Infraspinatus.
- It supports the shoulder’s adduction and extension.
- Abducts the scapula’s inferior angle once the humerus is stabilized.
Embryology
The myotome of the paraxial mesoderm (somites) gives rise to the teres minor, a muscle in the upper limb. Around four weeks into development, the upper limb bud emerges and is located across somites C4, C5, C6, C7, C8, T1, and T2.
The myotomes migrate into the limb bud around week five, forming two anterior and posterior condensations. They frequently occur when the tendon rubs against the bone that is at or near the tendon. By eight weeks, the muscular groups are well-established.
Related Muscles
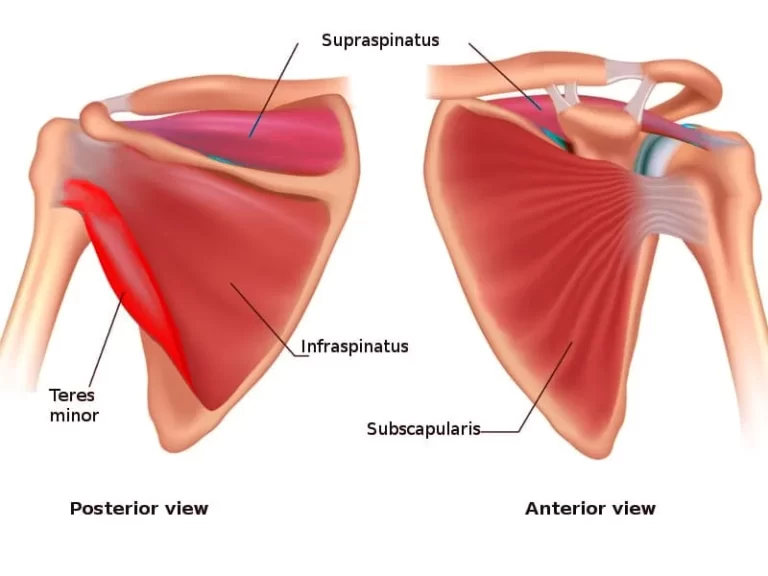
The teres minor, supraspinatus, infraspinatus, and subscapularis are the four muscles that make up the rotator cuff.
The posterior scapula is the source of the supraspinatus, infraspinatus, and teres minor, which all insert into the larger tubercle of the humerus. The anterior scapula’s subscapular fossa is the source of the subscapularis, which attaches to the humerus’s lesser tubercle.
Together, the rotator cuff muscles stabilize the glenohumeral joint, a ball-and-socket joint that is much shallower and more unstable than the hip. Every muscle aids in specific arm movements as well. The deltoid, an intrinsic shoulder muscle that is not a rotator cuff muscle, is in charge of abduction from 15 to 90 degrees; the supraspinatus is in charge of the first 15 degrees.
Supporting in lateral or external rotation of the arm at the shoulder is the infraspinatus and teres minor. Medial or internal, rotation of the arm is performed by the subscapularis, extrinsic muscles such as the latissimus dorsi and pectoralis major, and the teres major, another intrinsic muscle.
Surgical Considerations
Even with a tear to the teres minor, a rotator cuff tear cannot heal on its own; nonetheless, it is frequently possible to restore good function to the injured shoulder without surgery. Therefore, if nonsurgical treatment is ineffective and the patient continues to feel pain or weakness, or if the arm’s optimal function is needed for sports or overhead work, surgery is indicated.
The kind of rip determines the kind of surgical repair. Only debridement, or the removal of injured tissue, may be necessary for an incomplete tear, or “partial thickness” tear. Although it may only affect a portion of the tendon, a “full-thickness” rip goes all the way through the tendon and can be fixed with side-to-side sutures.
A full tear—a condition where the tendon is torn completely away from its bony insertion—occurs most frequently in rotator cuff injuries, necessitating immediate tendon restoration return to the bone. Surgical repair can be performed in two ways: open, through which a big incision allows direct access to the injury, or arthroscopic, through which two small incisions allow the passage of an arthroscope and tools for damage repair.
Clinical Significance
Injury
This can involve throwing a hard pitch, holding onto a fast-moving rope when engaging in water sports, falling into an outstretched hand abruptly, or pushing with the paddle when paddling. A persistent rip gradually becomes larger.
They frequently occur when the tendon rubs against the bone that is at or near the tendon. In most cases, the teres minor is normal after a rotator cuff tear.
Imaging
Although isolated teres minor atrophies have also been observed, rotator cuff tears often cause minor muscle atrophy. Excessive and/or sustained compression of the components passing through this anatomical tunnel results in circular space syndrome.
The entrance is used by the posterior humeral circumflex artery and the axillary nerve. Shoulder pain and paresthesia down the arm are the most typical complaints from individuals affected by abduction, extension, external rotation, and overhead exercise. There is a direct correlation between compression of the relevant posterior humeral circumflex artery or axillary nerve branch and selective atrophy of the teres minor muscle.
These illnesses need to be considered to provide the most comprehensive differential diagnosis that is possible.
Quadrangular Space Syndrome
The axillary nerve and the posterior humeral circumflex artery are two examples of structures that are too or persistently compressed when quadrangular space syndrome occurs. Overuse of the arm, especially during overhead activities, or atraumatic injury such as a dislocated shoulder can result in the condition. The posterior humeral supplies the teres minor, which is innervated by the axillary nerve. Thus, paresthesia, nebulous shoulder discomfort, and selective atrophy of the teres minor may be associated with quadrangular space syndrome.
Tendinitis
Tendinitis is an inflammation or irritation of the tendons of the rotator cuff muscles, involving the teres minor tendon. While rotator cuff tendinitis is typically the result of repetitive arm use, frequently from overhead activities, tendinitis is typically exertional injury brought on by repeated use. When the patient raises their arm above their head, they will experience clicking or pain.
Conservative measures of treatment include rest, ice, and anti-inflammatory drugs. Exercises for strengthening and stretching the tendons aid in lowering the force applied to them. Injections of cortisone may be used to treat refractory pain.
The term “shoulder impingement syndrome” refers to the overhanging acromion bone of the scapula compressing and impinging on the rotator cuff tendons, notably the teres minor. Impingement results from a narrowing of the space between the rotator cuff and the acromion, which is frequently brought on by repetitive arm movements overhead that irritate the rotator cuff tendons.
Patients may have shoulder pain in addition to shoulder weakness, especially while attempting to raise an arm overhead. Conservative measures of treatment include rest, ice, and anti-inflammatory drugs.
Tear
The teres minor is one of the rotator cuff muscles that are susceptible to tearing. Tears may be acute or persistent. Attempting to carry anything heavy or falling on an outstretched arm are the usual causes of an acute tear.
A chronic tear develops gradually and is usually the result of muscular deterioration caused by tendinitis or shoulder impingement syndrome. Although a rotator cuff injury cannot heal on its own, it is frequently possible to restore good shoulder function without surgery.
Assessment of Teres Minor Muscle
Hornblower’s sign
Lying prone, sitting, or standing
For females, a halter top or a gown covering the non-examined side with the examined portion exposed is advised.
Treatment of the sufferer.
When the patient’s shoulder is relaxed, place your fingers on the superior aspect of the scapula’s axillary border, which is inferior to the infraspinatus tendon and lateral to the infraspinatus muscle belly.
With the elbow flexed to 90 degrees and the elbow tucked to the side of the patient’s body, place the patient’s arm in neutral.
Exercise of Teres Minor Muscle
Teres Minor Muscle Stretching Exercise
Shoulder Adductor Stretch
- Maintain a standing posture next to a wall.
- Lay the arm closest to the wall’s left palm flat against it.
- As high as you can without being hurt, start to stroll your left hand’s fingers straight up the wall.
- Reposition your left hand so that it is flat against the wall, then press your weight against it.
- A stretch runs down the left side of your body and through your left arm.
- After 30 seconds of holding it, switch to the right side.
Sleeper Stretch

on a level, stable surface with your right side up.
Your arm is bent, and your right shoulder is beneath you.
Put your left hand over your right.
Press the right arm down with your left arm.
The rear of your right shoulder feels strained.
For a total of thirty seconds, hold it and then release it.
Proceed to the left. four times on each side.
External Rotation Stretch
An elastic band is required for the patient to perform this stretching.
Using an elastic band, create a loop that is 2 to 2.5 feet long.
Next, fasten the ends together and attach the loop to both the stable item and the firm.
Now, encircle an elbow with a loop. After that, keep your elbow bent and close to your side.
After that, turn the arm out.
In one repetition, hold the position for 30 seconds if the patient feels stretched, then repeat.
Return to the starting position and complete two sets of three repetitions on each side.
Cross body Stretch
Place your right arm straight across your chest as you stand.
Your left shoulder is behind your right hand.
Raise your forearm and keep your left elbow close to your chest to support your right elbow with your left arm.
Press your right elbow in toward your chest with your left forearm.
Hold it for up to 30 seconds when you start to feel stretched.
Doorway stretch
With their back to the closed door, the patient assumes a lofty posture.
To grip a door handle, now shift the arm to the back and bend the left elbow.
Next, bend forward and take a step forward.
The patient reports feeling a stretch across the outside of the left scapula, behind the shoulder.
Repeat on the other side after holding it for 30 seconds in one repetition.
Perform three sets of three reps each.
Triceps Stretch
Maintain a straight upper torso and a tall posture.
Then raise your right arm into the air.
Subsequently, bend at the right elbow to align the palm with the spine.
With the left hand, apply pressure by placing it on the right elbow.
To experience the deep stretch, gently draw a bent right elbow back and towards the head with the left hand.
In one repeat, hold this posture for thirty seconds, then release it.
Perform three sets of three repetitions.
Work out three times a day.
Continue and then move to the left arm.
Passive External Rotation Stretch
The patient requires a stick to complete the stretch.
Hold a stick by one end with one hand and the other end with another.
Now, throughout the stretching, maintain the left elbow close to the body.
Next, move a stick horizontally to the right side.
There can be a tug on the patient’s left rear shoulder.
In one repetition, hold the stretch for 30 seconds, then release it for another 30 seconds.
Perform three sets of three repetitions.
Conduct three sessions every day.
On the right side, repeat.
Teres Minor Muscle Strengthening exercise
Reverse Dumbbell Fly
Place your feet hip-width apart and start standing while holding a dumbbell in each hand.
Bend your knees slightly and push your hips back behind you while bending your torso forward with a flat back. Keep your hips in this posture for the duration of the workout.
With your palms facing each other and your elbows slightly bent, let the weights drop toward the floor.
Lift the weights out to your sides until they are in line with your shoulders, being sure to keep your shoulders down and away from your ears and slightly bend your elbows.
Carefully lower the dumbbells.
Single-Arm Dumbbell Row
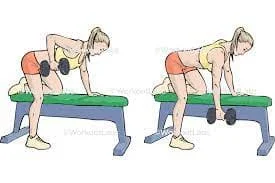
Place your left foot back and stand with your feet spaced apart.
With your right hand softly resting on your right thigh for support, hold a dumbbell in your left hand.
Lean your body forward, keeping your back flat, and hinge your hips back.
Raise your right arm to your abdomen while maintaining your elbow at your side.
After that, turn around and carefully reduce the weight.
After completing the left arm, swap sides.
Cable External Rotation

At elbow height, fasten a handle to the cable station pulley.
With your left hand, grasp the handle, and position the cable machine so that it is on your right side.
Bend your elbow to a 90-degree angle and tuck it into your left hip so that your forearm and palm face inward.
To remove the handle from your body, spin your shoulder outward without straightening your arm.
Tuck your left elbow into your left hip and bend it to a 90-degree angle so that your forearm and palm face inward to revert to your beginning position.
Complete all repetitions of both internal and external rotation using one arm, then move on to the other.
Inverted Row
About your arm’s length above the ground, place the bar.
Lay down under the bar and spread your legs out in front of you.
Raise your arms and grasp the bar with both hands in an overhand hold wider than the distance between your shoulders.
Ensure that your heels are flat on the ground and that your limbs are extended straight.
To raise yourself up, pull your shoulder blades back until your chest contacts the bar.
Reduce gradually to the beginning point.
BAND PULL PARTS
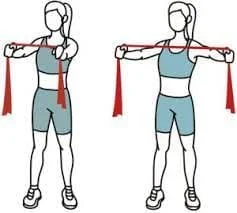
Stand up straight with your feet shoulder-width apart.
Hold the band toward its ends with an overhand grasp.
Squeeze your shoulder blades together to release the band.
Return to the starting position gradually.
LAT PULL-DOWNS

Sit down on a bench with your back to the cable machine.
Reach up and grab the bar with both hands in an overhand hold that is a little wider than shoulder-width apart.
Pull down on the bar by bringing your shoulder blades back and down when it reaches your chest.
Return to the starting position gradually.
Seated shoulder external rotation
The external rotators of the shoulder are the main target of this workout.
Place one foot on the bench and support your elbow with that foot as you sit on a bench to elevate your knee.
Start with your elbow bent to a 90-degree angle and your lower arm parallel to the ground.
Until your lower arm is nearly in line with the floor, or as close as you can manage, turn your shoulders slowly downward.
Turn carefully back up, and repeat if needed.
Side-lying external rotations
This workout targets the shoulder’s external rotators, which are in charge of fortifying the rotator cuff.
Hold a hand weight with your upper arm while you are on your side.
Raise the weight to the maximum outward rotation while keeping the elbow tucked in your body (within normal bounds).
Repeat the procedure of lowering the weight gradually until it is in front of your abdomen.
Isometric external rotation
This is an exercise that uses work-based isometric compression against a wall.
Align your elbow 90 degrees to the wall as you stand next to it.
Maintain a straight elbow that is slightly below your shoulder.
Thumb up and slowly press outward against the wall for three seconds, building up your strength.
Remain at your maximal contraction for five to seven seconds, then progressively back off until you are at rest (for another three-second count).
Conclusions
Despite its relatively small size, the teres minor plays a crucial role in shoulder function and overall upper extremity movement. Injuries or dysfunctions involving this muscle can lead to shoulder instability, weakness, and decreased range of motion, emphasizing its importance in maintaining optimal shoulder health and function.
For the majority of rotator cuff injuries, the teres minor was normal. In both solitary and multiple rotator cuff tears, the appearance of the teres minor in CT and MRI images could be described using a morphologic classification scheme.
FAQ
What is the main movement of teres minor?
The teres major is a thick, flattened muscle that extends from the inferior posterior scapula to the medial lip of the humeral intertubercular groove. It works in concert with the latissimus dorsi to adduct, internally rotate, and extend the humerus.
What is an MRI of the teres minor?
When evaluating teres minor tears and denervation injuries, MRI is a useful tool for identifying related abnormalities of the capsule and labrum in cases of teres minor tears, as well as for recognizing possible masses, fatty atrophy, and muscular edema in cases of denervation.
How common are teres minor tears?
Teres minor tears are rare, accounting for as little as 0.9% of all rotator cuff injuries, according to reports. However, it has been noted that fatty infiltration of the teres minor muscle occurs more frequently (at a rate of about 3%) when other cuff tendons are torn.
What is the antagonist of the teres minor?
posterior deltoid, infraspinatus, rhomboid major, rhomboid minor, supraspinatus, upper trapezius, anterior deltoid, latissimus dorsi, lower trapezius, pectoralis major, pectoralis minor, and posterior deltoid. The levator scapulae, serratus anterior, middle trapezius, and middle deltoid are antagonistic.
What is the teres minor attached to?
One intrinsic muscle in the shoulder region is the teres minor. It is a member of the rotator cuff muscle group. Attachments: arises from the scapula’s posterior surface, right next to its lateral border. It affixes to the humerus’s larger tubercle.
What causes fatty atrophy of the teres minor muscle?
The cause of fatty infiltration of the teres minor is still unknown in many cases, while possible causes include disuse from related injuries, traction injuries on the axillary nerve following trauma, chronic rotator cuff tears, and quadrilateral gap syndrome.
What are the facts about teres minor?
External rotation of the shoulder joint is the primary result of Teres Minor and Infraspinatus. It supports the shoulder’s adduction and extension. Abducts the scapula’s inferior angle once the humerus is stabilized.
What causes teres major and minor pain?
Overuse or tension on a muscle is a common cause. Some specific causes for this particular muscle are as follows: strong steering wheel control. both reaching ahead and above, especially while carrying bulky items, like when cutting wood. sleeping for extended periods with the arm medially rotated
What does teres minor pain feel like?
Pain in the posterior shoulder and tingling and numbness in the fourth and fifth digits are caused by trigger points located in the teres minor. Since the infraspinatus muscle and the teres minor muscle collaborate closely, trigger points between those two muscles are common, and they don’t usually occur alone.
How is a teres minor tear diagnosed?
Trigger points in the teres minor induce pain in the posterior shoulder as well as tingling and numbness in the fourth and fifth digits. Trigger points between the teres minor and infraspinatus muscles are common and normally do not develop alone because those two muscles work closely together.
How do you strengthen the teres minor muscle?
Dumbbell Pullover: Lie across the bench with only your upper back and neck being supported by the bench.
Cable Straight Arm Pull Down
Inverted Row
Underhand Yates Row
Underhand Grip Lat Pull down
Lat Pull Downs
Pull Ups
Chin Ups
What are the facts about teres minor?
The larger tubercle is a bony landmark on which the teres minor joins to the humeral head after beginning on the lower, lateral margin of the scapula. The teres minor produces an equal amount of external rotation force when the shoulder is abducted, unlike the infraspinatus (raised overhead).
Why does my teres minor muscle hurt?
Overuse (repetitive overhead reaching, pushing, or even lifting with outstretched arms) or prolonged muscle weakening can also result in injuries. Overuse of a muscle can lead to the common condition known as tendinitis, or inflammation of a tendon.
What causes teres minor trigger points?
Rarely do trigger points in the teres minor occur on their own; instead, they are triggered by straining the infraspinatus muscle. In the belly of the teres minor, these trigger points cause complaints of localized pain beneath the deltoid muscle.
What is the function of the teres major and minor?
The teres major muscle does not adhere to the glenohumeral joint capsule like the teres minor does. It is therefore not thought of as a component of the rotator cuff muscles. This muscle’s primary job is to generate arm movements at the shoulder joint.
Is the teres minor an internal or external rotator?
These two muscles are the external rotators of the shoulder and are located beneath the scapular spine. Teres Minor is more active when the arm is externally rotated in a 90-degree abduction, whereas Infraspinatus predominantly acts with the arm in neutral.
What is the action and nerve supply of the teres minor?
The teres minor’s main job is to control the deltoid’s motion, which keeps the humeral head from sliding upward while the arm is abducted. It also has the role of laterally rotating the humerus. The axillary nerve innervates the teres minor.
What is the exercise for teres minor rehab?
With your feet flat on the ground, take a straight seat in the chair. Bending the elbows, bring the band in close to the chest and squeeze the shoulder blades together. Letting go of the shoulder blades, slowly go back to the beginning position. Perform the exercise eight to twelve times.

One Comment