Suprascapular Nerve
Introduction
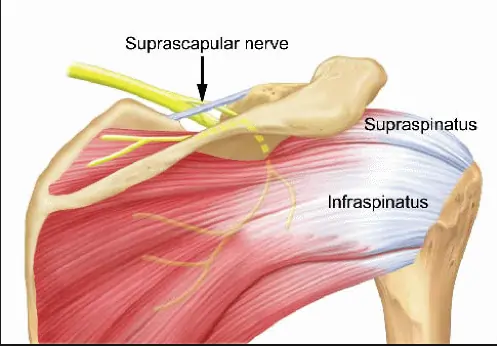
The suprascapular nerve is a branch of the brachial plexus (C5-C6) that supplies motor innervation to the supraspinatus and infraspinatus muscles, which are key for shoulder movement and stability.
It also carries sensory fibers to the glenohumeral joint and surrounding ligaments. The nerve passes through the suprascapular notch, where it is susceptible to compression or injury, leading to shoulder pain and weakness.
Structure
The infraspinatus and supraspinatus muscles are innervated by the suprascapular nerve, which emerges from the brachial plexus upper trunk. It begins in the neck’s posterior triangle and extends laterally and downward parallel to the omohyoid muscle’s belly to the top portion of the scapula. It connects to the supraspinatus fossa beneath the suprascapular ligament. Here, it innervates the muscles of the supraspinatus and infraspinatus.
Function
As a mixed nerve, the suprascapular nerve has both motor and sensory components. As sensory innervation, the acromioclavicular and glenohumeral joints receive sensory branches from the suprascapular nerve. The supraspinatus and infraspinatus muscles are innervated by the motor portion of the suprascapular nerve, respectively.
The ventral rami of the fifth and sixth cervical nerves from the upper trunk of the brachial plexus unite to form the suprascapular nerve, which has its origin in the upper trunk of the brachial plexus. In about 18% of people, the ventral ramus of the fourth cervical nerve is also affected. Along the neck’s posterior triangle, the suprascapular nerve emerges from the upper trunk. It passes parallel to the omohyoid muscle’s belly and descends to the top portion of the scapula.
From there, it passes beneath the suprascapular ligament and ends at the supraspinatus fossa. It passes beneath the supraspinatus muscle in the supraspinous fossa, branching twice for innervation, and then curves around the spinoglenoid notch, over the lateral edge of the scapula’s spine, and into the infraspinous fossa. The infraspinatus muscle is innervated by the nerve branches in the infraspinatus fossa.
Course
The superior trunk of the brachial plexus is the origin of the suprascapular nerve (root values C5, C6). Along with the dorsal scapular nerve, long thoracic nerve, subclavian nerve, and auxiliary phrenic nerve, it is regarded as one of the brachial plexus’s preterminal or supraclavicular branches. It should be noted that the nerves that emerge from the brachial plexus’s cords are referred to as the terminal branches, whilst the cords themselves are known as the infraclavicular branches.
The suprascapular nerve travels laterally from its origin, past the posterior triangle of the neck, and above the brachial plexus. It subsequently enters the supraspinous area of the scapula by passing through the scapular notch, which is inferior to the superior transverse scapular ligament. Here, it branches off to the supraspinatus muscle and proceeds to the infraspinous fossa via the larger scapular (spinoglenoid) notch, which is situated between the glenoid cavity and the scapula’s spine root.
Ultimately, the nerve innervates the infraspinatus muscle by terminating there. The suprascapular nerve’s route is distinct from that of the suprascapular artery and vein, which run above the superior transverse scapular ligament, to prevent confusion.
Muscle Supplied
Both motor and sensory innervation are present in the suprascapular nerve. The muscles of the supraspinatus and infraspinatus receive their motor innervation. The glenohumeral (shoulder) joint is composed of four muscles, two of which are the supraspinatus and infraspinatus.
The posterior scapula’s supraspinous fossa is where the supraspinatus muscle begins. After that, it joins the larger tubercle of the humerus at its superior facet. The supraspinatus, which receives innervation from the suprascapular nerve, works in tandem with the rotator cuff muscles to begin and assist the deltoid in the abduction of the arm.
The posterior scapula’s infraspinous fossa is where the infraspinatus muscle begins. After that, it attaches to the middle facet of the larger tubercle by encircling the lateral proximal humerus. The rotator cuff muscles work in tandem with the infraspinatus to externally rotate the arm.
Branches
A mixed nerve is the suprascapular nerve. Its primary job is to deliver motor power to two of the rotator cuff’s five muscles, which include:
- Supraspinatus muscle
- Infraspinatus muscle
Two joints get sensory innervation from the sensory branch that the neuron produces along its path:
- The glenohumeral joint (shoulder)
- Acromioclavicular joint
Embryology
The suprascapular nerve is derived from the ventral rami of the fifth and sixth cervical nerves, as well as the ventral ramus of the fourth cervical nerve in some populations. The motor nerve roots originate in the spinal cord’s ventral ramus.
The neural tube’s intermediate zone produces the motor neuroblasts of the ventral and lateral horns, from which the ventral (motor) plate grows as a ventrolateral thickening of the neural tube.
Branched axons start at the motor neuroblast, leave the spinal cord, and become the ventral (motor) roots. The basal plate subsequently transforms into the dorsal horn of the spinal cord. After migrating to the nerve, the neural crest undergoes differentiation to become Schwan cells.
Anatomical Variation
Variants of the suprascapular nerve are not well documented. Three variations in the interaction between the suprascapular vessels, nerve, and superior transverse scapular ligament are described in the literature by Polguj et al.
The most prevalent variation is the one in which the nerve and vein travel inferior to the superior transverse scapular ligament, while the suprascapular artery runs superior to it. The second is where the nerve travels inferior to the ligament and the artery and vein flow superior to it. The third and least frequent variation occurs when the nerve, artery, and vein pass beneath the superior transverse scapular ligament.
Examination
The gold standard for diagnosing suprascapular nerve palsy is thought to be nerve conduction tests and electromyography. Suprascapular nerve compression and denervation are indicated by prolonged latency, reduced amplitude, fibrillation potentials, and positive sharp waves in the nerve conduction examination.
X-rays can be used to rule out bone trauma in the area.
The location of the damage can be determined with the use of diagnostic ultrasonography, CT, and MRI. The diagnosis may be supported by immediate pain alleviation after an anesthetic injection to the suprascapular or supraglenoid notch.
Clinical Importance
Suprascapular nerve entrapment
An uncommon disease known as suprascapular nerve entrapment (suprascapular neuropathy) is characterized by discomfort and weakness in the posterior shoulder area, which weakens the shoulder’s abduction and external rotation.
The supraspinatus and infraspinatus muscles become weak as a result of damage to the nerve fibers induced by a traumatic injury to the suprascapular nerve. Compression of the nerve during its passage through the suprascapular notch, whether acute or non-traumatic, is the other common reason.
Surgical Importance
When doing extensive rotator cuff repairs, the suprascapular nerve is in danger. The nerve is near the surgical region utilized for rotator cuff repairs, according to literature. The nerve is vulnerable in the vicinity of the acromion’s lateral border, rotator cuff footprint, and glenoid rim.
When using a double interval sliding approach for arthroscopic cuff repairs, the nerve is also susceptible to damage in the vicinity of these regions. When treating shoulder pain, suprascapular nerve blocks may be used since the nerve is susceptible to compression neuropathy at the spinoglenoid notch and suprascapular regions.
FAQs
What is the function of the suprascapular nerve?
As sensory innervation, the acromioclavicular and glenohumeral joints receive sensory branches from the suprascapular nerve. The supraspinatus and infraspinatus muscles are innervated by the motor portion of the suprascapular nerve, respectively.
What happens if the suprascapular nerve is damaged?
What is suprascapular nerve palsy? Damage to the suprascapular nerve results in suprascapular nerve palsy. The muscles that the suprascapula nerve innervates (controls) may become weak and painful as a result. The shoulder muscles known as the supraspinatus and infraspinatus are innervated by the suprascapula nerve.
How do you treat suprascapular nerve pain?
Suprascapular neuropathy can also be treated using nerve blocks in addition to conservative and surgical methods. By anesthetizing (numbing) the suprascapular nerve with an injection, these blocks significantly reduce symptoms and the shoulder discomfort associated with this disorder.
What is the recovery time for suprascapular nerve palsy?
Full recovery, including a return to normal activities, can take around 3 to 6 months, depending on the severity of the initial condition, the degree of muscle and nerve damage; and a patient’s overall health. For arthroscopic suprascapular nerve release, patients are placed under general anesthesia
How to stretch the suprascapular nerve?
Using the hand behind your back, hold a towel draped over your opposite shoulder. 3. Pull your hand slowly up your back with the towel until you feel a slight stretch.
References
- Suprascapular nerve. (2023, October 30). Kenhub. https://www.kenhub.com/en/library/anatomy/suprascapular-nerve
- TeachMeAnatomy. (2023a, September 19). Suprascapular Nerve – Course – Functions – TeachMeAnatomy. https://teachmeanatomy.info/encyclopaedia/s/suprascapular-nerve/
- Suprascapular nerve. (2022, October3).StatPearls.https://www.ncbi.nlm.nih.gov/books/NBK557880/