Recurrent Shoulder Dislocation
Introduction
Recurrent shoulder dislocation is a disease that develops when the glenohumeral joint, or shoulder joint, dislocates frequently. Being one of the most moving joints in the human body, the shoulder is among the most susceptible to dislocation. Shoulder instability, also known as recurrent shoulder dislocations, is the state in which the dislocations become recurring. Such unstable shoulders typically have shallower shoulder joints with a wider diameter than the socket.
A recurrent shoulder dislocation may result from:
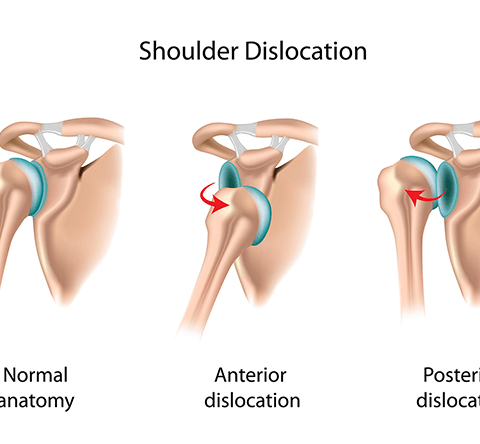
- The front of the socket is prone to anterior dislocation.
- Posterior Dislocation is the socket behind it.
- The inferior dislocation socket is located below.
Because the shoulder joint is inherently unstable, the glenoid labrum, muscles, and tendons work together to hold it in place. A severe trauma may result in a dislocated joint. Osteoarthritis can result from a recurrent shoulder dislocation, which is far more likely to occur again after one incidence. Eventually, the shoulder may dislocate even during routine activities. This will happen more frequently. Two types of treatment are available: Latarjet repair (a bone block) or Bankart repair (arthroscopic surgery to repair the labrum and restore capsule tension).
Relevant Anatomy
- Human shoulders are some of the most dynamic and vulnerable joints. It allows the humerus to articulate against the shoulder blade’s glenoid rim: glenohumeral ligaments and the glenoid labrum, a fibrous ring of tissue, supply stability.
- The glenoid labrum separates from the glenoid and loses some of its stabilizing power when the shoulder dislocates. Moreover, the bone on the humerus head and shoulder blade degrades with each full or partial dislocation of the joint.
- The two bones lose contact and the joint becomes more and more unstable. This is the reason why the dislocation keeps happening. We call it recurring dislocation.
What is Recurrent Shoulder Dislocation?
- Recurrent shoulder dislocation occurs whenever the glenohumeral joint, or shoulder joint, repeatedly dislocates. The shoulder joint is very dynamic in the human body, which makes it especially fragile to displacement.
- In contrast to posterior dislocations, anterior shoulder dislocations take place more frequently. In addition to repetitive strain from specific sports or hobbies, traumatic events like falling onto an outstretched arm can result in shoulder dislocations. The most common indication when a shoulder is dislocated is pain. The intensity of the pain may vary depending on whether the dislocation was immediate or progressive.
- When the humerus’ head is outside of the shoulder joint, it is called a dislocated shoulder. Out of all the joints in the body, the shoulder is the least stable and most flexible. Consequently, it is the joint that is most vulnerable to dislocations or subluxations. After the first dislocation, the shoulder tends to dislocate or subluxate more frequently in a percentage of these patients. Patients are considered to have an unstable shoulder or shoulder instability if they have a propensity for recurrent dislocation or subluxation.
Epidemiology
- Recurrence after the first dislocation of the shoulder is more than 90% likely. This is particularly true for youth under the age of twenty. This is because a dislocated shoulder involves more than just a joint injury. It is damage to soft tissues like tendons and ligaments as well as the surrounding muscle. These muscles and tissues work together to keep the joint firm. The shoulder joint becomes weaker when a dislocated shoulder causes these soft tissues to be ripped or injured. Additionally, it might dislocate once again.
- However, recurring shoulder dislocations are less common in older adults, particularly in those 50 years of age or later. When it occurs, a ruptured ligament at the rotator cuff at the top of the shoulder usually coexists with it. This is due to the gradual degeneration of our soft connective tissues with aging. Our ligaments and tendons are therefore more prone to tearing.
What are the Types of Recurrent Shoulder Dislocation?
Three primary types can be used to categorize recurrent shoulder dislocation.
- Anterior Dislocation
- Posterior Dislocation
- Inferior Dislocation
Anterior (forward) Dislocation of the Shoulder Joint:
- The humerus is displaced anteriorly in more than 95% of shoulder joint dislocations. In the majority of cases, a sub-coracoid dislocation occurs when the humerus’ head rests beneath the coracoid process. Dislocations of the subglenoid, subclavicular, and, extremely infrequently, intrathoracic or retroperitoneal regions can also happen.
- An outstretched arm is typically struck directly or falls on it, resulting in an anterior dislocation. Usually, the patient retains his or her arm slightly abducted and externally rotated.
- Lesion of Hill-Sachs. An impaction of the humeral head caused by the glenoid rim during dislocation is known as a Hill-Sachs deformity.
- An injury to the axillary nerve results in weakening or palsy of the deltoid muscle. Unilateral deltoid atrophies result in the loss of the shoulder’s typical rounded shape.
Posterior (backward) Shoulder Dislocation:
- Periodically electrical shocks generate convulsions or muscular spasms that lead to posterior dislocations. They could be caused by an imbalance in the rotator cuff muscles’ strength. Patients usually arrive with their arms held internally rotated and adducted, and they usually have a large coracoid process and anterior shoulder flattening.
- Unrecognized posterior dislocations can occur, particularly in patients who are unconscious from trauma or who are elderly. In a group of forty patients, the mean time between damage and diagnosis was one year.
Inferior (downward) Shoulder Dislocation :
- An inferior dislocation of the shoulder following a car collision. Observe the way the humerus is taken off. There is also a greater tuberosity fracture present.
- The least typical kind, inferior dislocation, appears in just over one percent of cases. The name “luxation erect” refers to another situation in which the arm seems to be held behind the head or upward all the time.
- The humeral head is pressed onto the acromion simply because of the arm’s hyperabduction. Due to the increased likelihood of vascular, neurological, tendon, and ligament injuries resulting from this mode of injury, such injuries have a high prevalence of complications.
What might be the cause of Recurrent Shoulder Dislocations?
Recurrent shoulder dislocation may arise from a variety of causes, the entire extent of which is unknown. Although there are numerous additional reasons why shoulder dislocations occur repeatedly, surgery performed on the same shoulder following an injury is the most frequent cause. The causes of recurrent shoulder dislocation might be traumatic or nontraumatic. A shoulder might become unstable for three primary, prevalent reasons:
Past History of Shoulder Dislocation
- Trauma or damage that occurs suddenly tends to cause the first dislocation of the shoulder.
- When the head of the humerus dislocation occurs, the shoulder ligaments and the glenoid, are also sometimes affected.
- The labrum, which is the band of cartilage around the glenoid, may also be bursting. The majority of the time, we define it as a Bankart lesion.
- A significant initial dislocation may result in further dislocations, collapse, or instability.
Repeated Strain
- Nearly all individuals who have chronic instability in their shoulders have not previously experienced a shoulder dislocation. The majority of these patients’ shoulder ligaments are more loosened.
- Sometimes this enhanced looseness is just a natural feature of their anatomy. It can occasionally be caused by frequent overhead motion.
- Activities like swimming, volleyball, and tennis demand a lot of overhead shoulder motion, which can strain the shoulder ligaments. Moreover, a lot of jobs call for overhead repetition.
- Shoulder stability might be difficult to maintain due to looser ligaments. Activities that are unpleasant or repetitive might put a strain on a weak shoulder. An uncomfortable and unsteady shoulder may arise from this.
Multi-directional Instability
- Shoulder instability can occur in a small percentage of individuals even in the absence of past injuries or repetitive strains.
- Patients with this condition may experience a dislocated shoulder that feels loose and can dislocate out of the front, back, or bottom of the shoulder. We call this multidirectional instability.
- These individuals may be “double-jointed,” with naturally loose ligaments throughout the body.
What indicators are present with Recurrent Shoulder Dislocations?
- Sometimes, there is significant pain that extends past the shoulder along the arm.
- The shoulder sounds like it’s falling out of the joint when doing abduction and external rotation.
- An external rotation and rotation of the shoulder and arm characterize an anterior dislocation, whereas an adduction and internal rotation constitute a posterior dislocation.
- Tingling and numbness in the arm.
- Visually misplaced shoulder. A dislocated shoulder might give the appearance of being unusually square.
- There is not a noticeable bone on the shoulder’s side.
How is a Recurrent Shoulder Dislocation treated?
- The symptoms are usually used to make the diagnosis, which is then verified by X-rays.
- The diagnosis of recurrent shoulder dislocation is often depending on the patient’s medical history and physical examination.
- The diagnosis is verified using radiographs. Radiographs displaying glenohumeral joint inconsistency often show the majority of dislocations. While they may be difficult to spot on typical AP radiographs, posterior dislocations are easier to spot on alternative views.
- Radiographs are typically taken again after reduction to ensure that the reduction was successful and to look for bone damage.
- To evaluate soft tissue damage following recurrent shoulder dislocations, an MRI scan may be performed.
- The apprehension test (anterior instability) and sulcus sign (inferior instability) are helpful tools for assessing susceptibility to subsequent dislocation in cases of recurrent dislocations.
How is a Recurrent Shoulder Dislocation treated?
Recurrent shoulder dislocations can be treated in two main ways:
- Non-Surgical Treatment
- Surgical Treatment
Non-Surgical Treatment
- Typically, a splint or sling has been employed to preserve the shoulder in a particular posture. Arrange a soft cushion between the arm and the torso to give support as well as comfort. To relieve the pain and anxiety associated with a dislocation, powerful painkillers are required.
- Initially, the doctors would attempt to address this disease with non-surgical measures; if they failed to improve the shoulder’s pain and instability, they would next consider surgery.
Surgical Treatment
When non-surgical treatment fails to relieve discomfort and shoulder instability, doctors turn to surgical intervention. In certain situations, surgery may be recommended to repair the torn and injured ligaments that stabilize the shoulder joint. The surgeons may choose to use one of the two techniques listed below.
Arthroscopy or key-hole surgery
This kind of procedure is typically performed same-day or as an outpatient. The doctors create tiny incisions close to the shoulder during this minimally invasive procedure. The process of mending the soft tissues with tiny devices is then carried out while a tiny camera views the shoulder. Relapse after arthroscopic surgery is 5%, which is extremely unusual with a bone block. The patient will require open surgery if it occurs.
Open Surgery
For certain patients, the surgeons may advise open surgery because of several reasons. During this procedure, a big incision will be made across the shoulder, and the surgeon will do surgery and direct tissue restoration. In modern treatment, open surgery is only necessary when a bone graft is required to repair the lost shoulder bone; bone reconstruction procedures can now be completed arthroscopically.
Post Surgery–Care
After surgery, it could be important to provide temporary assistance to the patient’s shoulder with a sling. The physical therapist and doctor might suggest exercises to strengthen the ligaments after the sling is taken off. Rehabilitation will aid in enhancing the shoulder’s range of motion and avoiding scarring during the healing process. The physician will also suggest shoulder muscle-strengthening activities.
Complication
- Nerve Damage: Although uncommon, this is a dangerous complication. Because the surgeon is repairing so near to the brachial plexus the bundle of nerves supplying the arm runs the risk of injuring a nerve, which could result in momentary loss of sensations, movement, or sensation of having pins and needles.
- Complications consist of Bankart lesions, Hill-Sachs lesions, rotator cuff tears, and axillary nerve injury.
What is physical therapy for the Recurrent Shoulder Dislocation?
- Shoulder dislocations Physical therapy is an important part of recovery following a shoulder dislocation or subluxation. It helps to:
- Strengthening activities that could be included in a rehabilitation program for a dislocated shoulder.
- As soon as the discomfort permits, an anterior dislocated shoulder strengthening program can be started. As this is the shoulder posture most likely to dislocate again, the athlete must avoid early motions that abduct and laterally rotate the shoulder.
- Static exercises that don’t require any movement should be done first and increased progressively.
Common physical therapy exercises for shoulder dislocation include the following:
- Pendulum exercises entail gently circularly swinging your arm to improve range of motion.
- Range of motion exercises helps increase shoulder flexibility and mobility by progressively rotating the joint in all directions.
- Strengthening exercises focus on shoulder muscles, such as the rotator cuff.
- Proprioception exercises increase your body’s ability to locate your shoulder joint in space.
The following exercises are suggested by physical therapists:
- Isometric shoulder external rotation: With your affected arm out in front of you, bend it to a 90-degree angle and press the back of your hand up against the wall.
- Shoulders External rotation: Using both hands, grasp an exercise band, pull it apart until you feel a stretch, and then slowly go back to the beginning position.
- Shoulder blades Squeeze: Squeeze your shoulder blades as if you were holding something on your back, and hold the position for ten seconds while standing or sitting up straight.
- Isometric shoulder flexion wall: Place your arm against a wall while standing facing it, then hold the contraction.
Listen to your physical therapist’s directions to the entirety to promote a speedy recovery. Regular physical treatment is required for a successful recovery. Attempt to attend all of your appointments. Working closely with a physical therapist can help you restore your shoulder function and prevent the risk of future dislocations.
What are the prevention for the Recurrent Shoulder Dislocation?
Recurrent shoulder dislocations are prevented with a mix of lifestyle changes, exercises, and medical interventions. Here are a few effective approaches:
- Reduce your involvement in contact sports and overhead throwing, as well as other activities that put undue strain on the shoulder joint.
- Maintain a healthy weight: Excess weight can cause additional strain on the shoulder joint.
- To avoid putting excessive strain on your shoulders, lift large objects with good form.
- Strengthen the rotator cuff muscles, which serve to support the shoulder joint. External rotations, internal rotations, and side-lying external rotations are all exercises that can help strengthen them.
- In some circumstances, using a brace or sling can help keep the shoulder from dislocating.
FAQs
What leads to recurrent dislocation of the shoulder?
The risk factors for shoulder dislocation are weak shoulder muscles, loose ligaments, and shallow joint sockets. Previous dislocation: Shoulder dislocations increase the likelihood of subsequent dislocations by stretching and tearing the muscles and ligaments holding the shoulder in place.
How can a recurrent shoulder dislocation be treated?
Patients who experience recurrent shoulder dislocations may be eligible for surgery to repair damaged or strained ligaments, which will improve the ligaments’ ability to stabilize the shoulder joint. It is possible to surgically correct bankart lesions. Anchors are used to sew the ligament back over the bone.
References
- Recurrent shoulder dislocation, recurrent pain. (n.d.). https://www.samitivejhospitals.com/article/detail/recurrent-shoulder-dislocation-recurrent-pain
- Recurrent Shoulder Dislocation – Docteur Bruno Lévy. (2023, March 13). Docteur Bruno Lévy. https://docteurbrunolevy.com/en/chirurgie/recurrent-shoulder-dislocation/
- Physiotherapist, N. P.-. (2023, July 22). Recurrent shoulder dislocation: Cause, Symptom, Treatment. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/recurrent-shoulder-dislocation/
- Recurrent Shoulder Dislocation Bangalore | Shoulder Dislocation Treatment. (n.d.). https://www.orthobangalore.com/recurrent-dislocations