
Pronator Teres Muscle
The pronator teres muscle is a key anatomical structure located in the forearm region of the upper limb. It plays a vital role in forearm pronation, which is the movement of turning the palm downwards or towards the posterior aspect of the forearm. This muscle is part of the superficial layer of the anterior compartment of the forearm.
What Is The Pronator Teres Muscle?
The pronator teres muscle twists the forearm so that the palm faces downward. The word pronator comes from the Latin word, which means “lying face downward.” The fusiform pronator teres muscle is located in the superficial layer of the anterior compartment of the forearm. Its main purpose is to help with forearm flexion and pronate the forearm. Thus, this muscle plays a crucial role in sports.
The pronator teres is innervated by the median nerve, which originates in the humerus and the ulna and passes via its two heads. Thus, in cases of overuse or even hypertrophy of the pronator teres, there is a danger of compression of the median nerve at this location.
Pronator teres syndrome is the clinical term for compression of the median nerve at this location. Pain and numbness are the most common symptoms of this condition in individuals, while movement disorders may also occur in some cases.
Structure of Pronator Teres Muscle
The pronator teres muscle has two heads—the humeral and the ulnar head.
The larger and more superficial humeral head originates from the common flexor tendon (which originates from the medial epicondyle of the humerus) and the medial supracondylar ridge, which is located directly above it.
The ulnar head, also known as the ulnar tuberosity, is a thin fasciculus that connects the preceding at an acute angle. It originates from the medial side of the ulna’s coronoid process.
As it enters the forearm between the two muscle heads, the ulnar head separates the median nerve from the ulnar artery.
The muscle ends in a flat tendon that is placed into a rough imprint in the middle of the lateral surface of the body of the radius, just distal to the supinator insertion. The forearm is crossed by the muscle laterally.
The cubital fossa, a triangular hollow anterior to the elbow, has its medial edge formed by the muscle’s lateral border.
The function of Pronator Teres Muscle
The pronation of the forearm, an exclusive upper limb movement, is the primary function of the pronator teres. At the proximal radioulnar joint, the muscle pushes the radius medially, rotating its head around the proximal portion of the ulna. By rotating the hand’s palm, this action also pronates the hand, turning it to face the earth. Pronator teres help with forearm flexion because it crosses the elbow joint.
The hand is turned posteriorly by the pronator teres, which pronates the forearm. The pronator teres muscle rotates the hand such that the palm faces inferiorly when the elbow is bent to a straight angle. In this action, the pronator quadratus aids it.
The pronator teres’ principal function is to pronate the forearm, as its name implies. The pronator teres works in tandem with the pronator quadratus to pull the radius medially, which rotates the radial head around the proximal ulna. The hand moves from supination, or upward palm position, to pronation, or downward palm position. Additionally, the pronator teres muscle has a minor function in elbow flexion.
Origin of Pronator Teres Muscle
Origin of Humeral Head: Directly above the deep antebrachial fascia, common flexor tendon, and medial epicondyle of the humerus.
Origin of Ulnar Head: The ulna’s coronoid process on the medial side
Insertion
The two heads combine to form a single muscular belly that inserts onto the lateral surface of the radius via a flat tendon. The pronator tuberosity is the name for this region, which is a rough spot in the center of the radius shaft. This region is situated below the supinator muscle insertion.
Actions
The primary function of the pronator teres is the pronation of the forearm. Additionally, it can support other muscles in the flexion of the forearm at the elbow.
These motions are helpful in sports like tennis, where forearm rotation is required for some strokes, such as backhands and forehands. Pronator teres help rotate the forearm during throwing and bat swings in baseball.
It also helps with the rotation of the forearm during a golf stroke. Pronator teres help rotate the forearm to twist a doorknob or lid, which is important for daily tasks like opening the cups and turning buttons.
Nerve supply
The median nerve supplies the pronator teres (C6, C7). The medial and lateral cords give rise to the median nerve, which is the brachial plexus’s terminal branch. In addition, the median nerve supplies sensation to the radial side of the hand and motor innervation to the forearm flexors and thenar line.
Blood Supply
Three arteries supply the pronator teres muscle’s vascularization:
branches of the ulnar artery: common interosseus artery, anterior ulnar recurrent artery
A branch of the radial artery known as the radial common artery
branches of the brachial artery; inferior ulnar collateral arteries
Embryology
The myotome, which gives rise to all limb muscles, is derived from the paraxial mesoderm cell layer. Nearby, the limbs’ bones, connective tissue, and vascular originate from the lateral plate mesoderm. Usually, limb buds begin to form at four weeks of gestation, and by eight weeks, the bones and muscles are fully developed. The size of the muscles increases after 8 weeks.
Related Muscles
All of the square-shaped pronator quadratus muscle, which originates on the anteromedial ulna and extends perpendicular to the direction of the forearm to insert on the anterolateral radius, performs a coordinated action with the pronator teres to produce a coordinated pronation action.
The pronation movement is brought about by the contraction pulling the radius toward and over the ulna. The median nerve stimulates this muscle as well. This muscle is found on the distal forearm, whereas the pronator teres lie on the proximal forearm.
Due to its minor aid in forearm flexion, the pronator teres muscle works in concert with several other muscles.
The supinator muscle, which comes from portions of the ulna, radial collateral ligament, annular ligament, and humerus, Supinates the forearm and inserts on the proximal radial shaft.
Associated condition of pronator teres muscle
Pronator teres syndrome is a disorder where the median nerve is compressed as it passes through the pronator teres muscle due to overuse or strain.
Inflammation, muscle spasms, and strains or tears in the pronator teres muscle are possible additional problems linked to it.
The forearm, hand, and fingers may experience pain, weakness, numbness, or tingling as a result of pronator teres syndrome. The symptoms may occasionally radiate to the neck or shoulder.
Other problems that are linked to the pronator teres muscle include injuries like fractures, dislocations, or sprains of the ligaments that affect the elbow, forearm, or wrist.
If you suffer an injury to your wrist or forearm, or if you are exhibiting any symptoms associated with the pronator teres muscle, you should consult a physician.
Diagnosis of pronator teres muscle
A complete physical examination is necessary to diagnose a pronator teres muscle ailment. Imaging tests and nerve conduction studies may also be performed. The following are typical steps for identifying a problem with the pronator teres muscle:
Physical examination:
In addition to examining the afflicted area, a medical professional may inquire about the patient’s symptoms, including any tingling, discomfort, weakness, or numbness in the fingers, hand, or forearm.
In addition, they might evaluate the patient’s strength, feeling, and range of motion in the afflicted arm.
Imaging tests
A pronator teres muscle ailment may be diagnosed with an MRI, ultrasound, or X-ray.
These examinations can detect any damage or irregularities in the surrounding structures, such as fractured bones or dislocated joints, or in the muscle itself.
Nerve conduction studies:
If pronator teres syndrome is suspected, a nerve conduction study may be requested to evaluate the median nerve’s function.
To monitor the electrical activity of the nerves, tiny electrodes are applied to the skin during this test.
Differential diagnosis
Conditions affecting the pronator teres muscle can be differentially diagnosed by taking into account the following conditions:
Carpal tunnel syndrome:
This is a disorder brought on by compression of the wrist’s median nerve.
It may result in hand and finger pain, weakness, numbness, or tingling, which are symptoms that are similar to those of pronator teres syndrome.
Ulnar nerve compression
Numbness and tingling in the ring and pinky fingers can be signs of compression of the ulnar nerve at the elbow and are sometimes confused with pronator teres syndrome.
Radial tunnel syndrome:
The radial nerve in the forearm is compressed, which results in this disease.
It may result in forearm soreness and tenderness, which may resemble pronator teres syndrome symptoms.
Cervical radiculopathy:
Compression of a nerve root in the cervical spine is the source of this ailment, which can result in hand and arm pain, weakness, and numbness.
Forearm muscle strains or tears
A pronator teres syndrome-like set of symptoms can also result from strains or rips in other forearm muscles, such as the flexor muscles.
Wrist or forearm fractures
Pain and weakness in the hand and forearm can also result from wrist or forearm fractures.
If you are having any forearm or pronator teres muscle-related problems, you must see a healthcare professional. The best course of treatment must be determined by a correct diagnosis.
Anatomical Variations of Pronator Teres Muscle
The ulnar head of the pronator teres may not always be present, based on studies that have been published. In a study of 60 upper limbs, Nebot-Cegarra et al. discovered that 78.3% of participants had an ulnar head.
Surgical Importance
Compressive neuropathy of the median nerve, which runs between the two heads of the pronator teres, is known as pronator teres syndrome. Weakness, sensations, and pain are some of its clinical signs. While conservative methods tend to improve most patients, in cases of severe manifestations of this illness or for those who do not respond to conservative treatment, surgical decompression may be a viable alternative.
The purpose of surgery is to compress the median nerve between the two pronator teres heads. First, the pronator teres superficial facia is freed. Depending on the degree of compression of the median nerve, either a partial or total excision of the tendon origin may come next.
The Disabilities of the Arm, Shoulder, and Hand (DASH) survey score as well as the Visual Analog Scale (VAS) pain score improve patients they are in operation. However, in one study, up to 25% of patients experienced carpal tunnel syndrome despite receiving appropriate decompression at the pronator teres.
Golfer’s elbow, or medial epicondylitis, is a disorder marked by pain along the medial portion of the elbow. Often starting slowly, the pain gets worse with forearm pronation or wrist flexion. In this situation, the pronator teres are frequently considered to be the cause of pathology.
Clinical Significance
Compression of the median nerve between the ulnar head and humeral head of the pronator teres causes pronator teres syndrome, an uncommon disease that is characterized by pain and numbness in the forearm. Neuropathic symptoms and weakening of the muscles innervated by the anterior interosseous (AIN) branch of the median nerve are common in patients with this illness.
The flexor pollicis longus, pronator quadratus, and flexor digitorum profundus of the second digit are the muscles that are frequently implicated. Excessive forearm pronation exacerbates the pain associated with this syndrome, which is more likely to be focused near the wrist.
Patients may experience frequent item drops and an increase in their perception of discomfort. Additionally, they could find it difficult to accomplish formerly easy actions involving these muscles, such as opening a prescription container that has a lock.
Only one to five percent of all median nerve neuropathies have this rare and low-incidence condition. As a result, this illness may be difficult to identify and is frequently mistaken for carpal tunnel syndrome in clinical settings. Additional diagnostic testing can help clarify its unique features and direct therapy.
Although they are not usually required for diagnosis, nerve conduction velocity (NCV) tests and electromyography (EMG) can be useful. The proximal forearm’s NCV will display a slower median nerve conduction velocity. While not required for diagnosis, magnetic resonance imaging (MRI) can be helpful and usually reveals abnormally elevated signal intensity in the pronator a T2-weighted picture, and atrophy of the forearm muscles innervated by the median nerve.
Stretching-focused physical therapy, NSAIDs, and rest are common treatments for this illness. If this method is unsuccessful, a corticosteroid injection into the pronator teres should be taken into consideration. Surgical decompression is the final therapy option.
Although they are uncommon, pronator teres strains have been documented in a few performers. Usually, an injury is caused by a bat or club hitting the ground while being looked around. An elbow in pronation is subject to an eccentric force as a result. Because it is so uncommon, medial epicondylitis and ulnar medial collateral ligament injuries can be mistaken for this ailment. Patients may exhibit tenderness to palpate over the pronator teres and ecchymoses. An MRI can frequently help with this injury’s diagnosis.
The cornerstone of treatment is conservative care, which includes rest, NSAIDs, and physical therapy. This approach frequently produces outstanding outcomes. Tennis and golf players who pronate their forearms during play may be at risk for developing pronator teres pathology.
Pronator tear injury may coexist with insufficiency of the ulnar collateral ligament, flexor-pronator tendinosis, medial epicondylitis, and lateral epicondylitis. Resistance bands can be used to strengthen the pronator teres, which is beneficial for treating strains and preventing injuries. By pushing a resistance band laterally while maintaining a modest flexion in the elbow, one can engage the pronator teres, which in turn causes the forearm to pronate.
The median nerve innervates the pronator teres and pronator quadratus, the two muscles responsible for the pronation of the forearm. As a result, injury to this nerve may cause weakness or even paralysis. Clinicians can determine the precise location of this injury with the aid of EMG and NCV. This condition may have direct trauma to the axilla or elbow nerve, or it may result from a supracondylar humerus fracture.
Assessment Of Pronator Teres Muscle
Palpation
The pronator tendon originates from the common flexor tendon at the medial epicondyle of the humerus.
It forms the cubital fossa’s medial border as it obliquely crosses from medial to Pronate or supinate the forearm and feels the antecubital fossa, usually in an almost medial direction, to palpate it.
Treatment of pronator teres muscle
The degree of damage and the severity of the injury will determine how best to treat a pronator teres muscle injury. The following common treatments can be recommended:
Rest
It’s critical to give the injured armrest so that the muscle can repair.
It is advised to stay away from activities that make the injury worse, such as hard lifting or repetitive motions
Ice
Reducing pain and inflammation in the wounded area may be achieved by applying an ice pack.
When necessary, use ice for 20 to 30 minutes every several hours
Compression
Compression sleeves or bandages can support the affected muscle and help with edema reduction.
Elevation
Reducing edema can also be aided by keeping the injured arm elevated above the heart.
Medications
It can be suggested to use over-the-counter painkillers, including ibuprofen or acetaminophen, to assist control of discomfort and inflammation.
Surgery
In severe circumstances, surgery can be required to relieve compression on the median nerve in cases of pronator teres syndrome or to repair a torn or injured pronator teres muscle.
If your symptoms seem like they could be caused by a pronator teres muscle injury, you should consult a doctor. They can offer an accurate diagnosis and suggest the best course of action for your particular requirements.
Exercise of Pronator Teres Muscle
Pronator Teres Stretching Exercise
Pronator Stretch
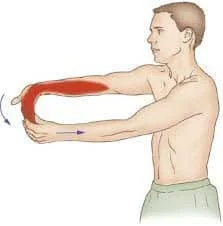
- With one elbow bent toward your body, rest the other hand on your hand’s back.
- Rotate your forearm so that the palm faces the ceiling with the assistance of the other hand, until your forearm stretches.
- Give the stretch a 20–30-second hold.
- Remain in that posture and unwind.
Wrist flexor stretch
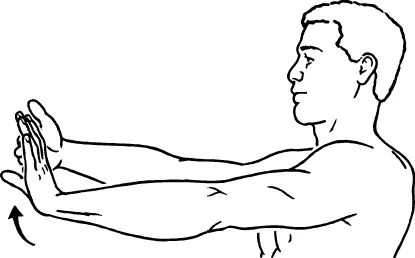
- With the palm facing up, extend the afflicted arm in front of you.
- Gently draw the fingers back towards the wrist with the other hand until the person’s forearm stretches.
- Hold for 10–20 seconds, then do so five or seven times.
Pronator Teres Strengthening Exercise
Pronation/supination with dumbbell

- The elbow should be bent while holding a light dumbbell with your palm facing downward.
- Gently extend your forearm until your palm faces above, then bring it in so that it faces downward again.
Hammer curls
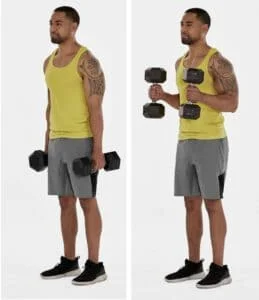
- With the palms of each hand facing your body, transfer a small amount of weight in them.
- With your palms facing inward, carefully raise your arms to your shoulders.
- Slowly lower your arms back down, then repeat 10–15 times.
Reverse curls

- A small amount of weight should be supported by both hands, with the palms facing the floor.
- Curl your arms slowly up to your shoulders, maintaining a downward-facing palm position.
- Slowly lower your arms back down, then repeat 10–15 times.
Wrist curls with resistance band
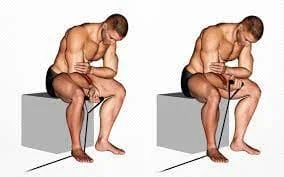
- Place your hand hanging off the edge of a table or bench, palm up, and place your forearm on it.
- A resistance band should be held with one end in your hand and the other end placed on a stationary object.
- Against the band’s resistance, carefully curl your wrist up toward your forearm and then slowly lower it back down.
Pronator teres stretch with resistance band

- Place your hand hanging off the side of a table or bench, palm down, and place your forearm on it.
- A resistance band has two ends: one is held in your hand, while the other is placed on a fixed object.
- Against the band’s resistance, spin your hand with your wrist toward your body and then slowly back outward.
Half-wrist rotation holds
This is a lower arm and wrist strengthening exercise.
You can use a chair, table, or bench to support your forearm.
Grip one end of a little weight while the hand is hanging off the bench’s edge.
Rotate the wrist to hold the weight at a 135-degree angle after holding it at a 45-degree angle for five seconds.
After holding for five seconds, switch sides, and repeat as needed.
Isometric wrist pronation
wrist pronation that is isometric Using a kettlebell, this exercise stresses the wrist and forearm muscles rotationally.
Pin a rolled-up towel or yoga block between your elbow and body to aid forearm muscle isolation.
Holding the weight by the handle, flex the elbow to a 90-degree angle.
Supinate the wrist to position the kettlebell bottoms-up and tilt it slightly outward of the forearm.
Hold this position for five to seven seconds.
Steer clear of full-range supination since this will strain your passive tissues more than the pronators in your wrists and forearms to support the weight.
Wrist flip
Flipping a wrist The wrist is strengthened by this workout.
Using a bench, table, or chair to support your forearm, hold a dumbbell.
Start with your wrist facing down and stretch it to lift the weight against gravity.
Then, to elevate the weight against gravity once more, flex and rotate the wrist such that the palm is facing upward.
Banded wrist pronation
An exercise to strengthen the wrist pronators is banded wrist pronation.
Put a band in your palm and loop it around your hand once, starting from the pinky side and working your way up to the thumb.
Grip the band with your thumb and ensure that the loop closes by encircling the back of your hand.
Hold the other end of the band in the hand that is not the target.
Starting with your palm facing upward, rotate the band until your palm is facing down.
Rotate in the other direction to complete a repetition.
Grip strength exercises
You can increase your total forearm strength and grip by squeezing a soft ball or utilizing a grip-strengthening tool.
Before beginning any fitness program, it’s crucial to speak with a physiotherapist or other healthcare professional to be sure it’s safe and suitable for your needs. To guarantee the best possible recuperation, they can modify the program as necessary and offer advice on the correct form and technique.
Summary
From the forearm’s inside (medial aspect) lies a muscle called the pronator teres. It comes from the ulnar head, which comes from the coronoid process of the ulna, and the humeral head, which comes from the medial epicondyle of the humerus. The muscle then attaches itself to the radius’s lateral aspect.
Pronation of the forearm, or the rotation of the hand’s palm from facing upward (supination) to facing downward (pronation), is functionally attributed to the pronator teres muscle. This motion is necessary for several tasks, including using a screwdriver, opening doors, and hitting a forehand stroke in tennis.
Conditions like pronator teres syndrome, which is characterized by discomfort and numbness in the forearm, weakness in gripping, and possibly tingling feelings radiating into the hand, can be brought on by use or injury to the pronator teres muscle. Physical therapy, stretching exercises, rest, and, in extreme situations, surgery are common forms of treatment.
FAQ
What is the pronator teres muscle used for?
supports the elbow joint flex by pronating the forearm. It functions in concert with the pronator quadratus. The muscle fibers are shortened and less able to provide force when the elbow is completely extended
What is pronator teres?
The superficial layer of the forearm’s anterior compartment contains the fusiform pronator teres muscle. Its main purpose is to help with forearm flexion and pronate the forearm. Thus, this muscle is crucially involved in athletic endeavors.
Why is it called pronator teres?
Pronation of the forearm is the motion of the muscle that gives rise to the word pronator, which is derived from the Latin prunus, which means “inclined forward or lying look down. The shape of the muscle is described by the Latin word teres, which means “round or cylindrical shaped” or “long and round.”
How can I train my pronator muscle at home?
Pronation and supination of dumbbells. Method: With one hand, hold a dumbbell vertically while putting your elbow on your knee.
Wrist Roller.
Resistance Band Pronation.
Towel Wring.
Hammer Curls.
Forearm Pronation with a Stick
What is the pronator teres stretch test?
The patient’s elbow is bent 90 degrees during the pronator teres syndrome test. The practitioner urges the patient to pronate his hand against the practitioner’s resistance while stabilizing the elbow with one hand. The medical professional holds this resistance while extending the patient’s elbow.
What is pronator teres muscle damage?
Injury to the pronator teres muscle is uncommon. In athletics, an injury may be misdiagnosed as a MUCL injury. Common observations include tenderness and weak/painful forearm pronation. An MRI aids in the grading of the muscular strain damage and validates the diagnosis.
How do you strengthen pronator teres?
Using a single-handed grip and a straight arm throughout, draw The Pronator across your body, twisting your shoulders but keeping your pelvis neutral. Go back to the starting position to finish the exercise. You can perform this exercise on the opposite side of your body.
What is the pronator muscle responsible for?
The forearm, directly below the wrist, contains the pronator quadratus muscle. It emerges from the ulna and inserts onto the radius with two heads. We can twist our forearm into the palm-down position (pronation) by using the pronator quadratus and pronator teres.
How do you treat pronator teres pain?
Inflammations and pain can be reduced by nonsteroidal anti-inflammatory drugs (NSAIDs).
Steroid injections to reduce swelling and pain.
Placing a bandage to provide elbow support.
Resting and icing the affected area(s)
Physical therapy.
What nerve is damaged in pronator teres?
Henrik Seyffarth initially described pronator teres syndrome (PTS) in 1951. PTS is brought on by the pronator teres (PT) muscle in the forearm compressing the median nerve (MN). The rounded, pronating PT muscle gets its name from both its shape and action.
How long do pronator teres take to recover?
For the great majority of people with pronator syndrome, conservative treatment is effective. It may only take three to six months of refraining from the problematic activity, splinting, and the use of nonsteroidal anti-inflammatory medicines (NSAIDs) to reduce inflammation for symptoms to improve under the careful supervision of a hand specialist.
In the pronator teres muscle, which nerve has been damaged
Pronator syndrome, commonly referred to as pronator teres syndrome (PST), is caused by compression of the median nerve in the upper forearm. One of the three nerves that allow us to sense objects at our furthest point is the middle nerve, whose growth begins in the upper arms and branches into the fingers.

2 Comments