Metatarsophalangeal (MTP) Joints
The metatarsophalangeal (MTP) joints are the connections between the metatarsal bones of the foot and the proximal phalanges of the toes. These joints play a crucial role in weight-bearing, balance, and movement, especially during walking, running, and jumping. Dorsal collateral ligaments and extensor tendons strengthen the joint capsule surrounding these synovial joints.
The first MTP joint, at the base of the big toe, is particularly important for push-off during gait. Common issues affecting MTP joints include arthritis, bunions, and turf toe.
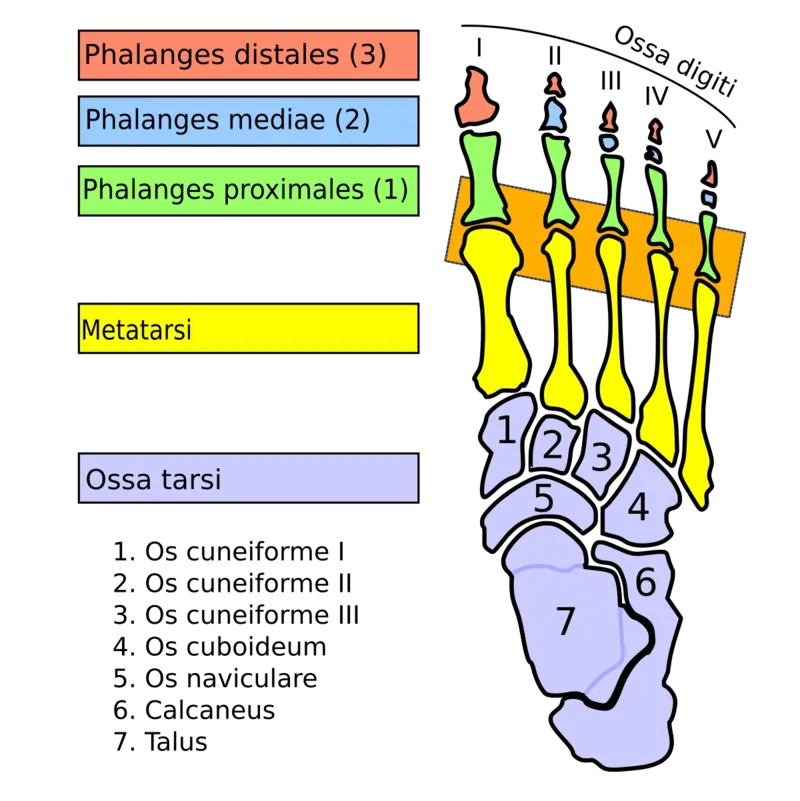
The joints that connect the foot’s metatarsal bones to the toes’ proximal bones, or proximal phalanges, are known as metatarsophalangeal joints, or MTP joints. They are referred to as toe knuckles in everyday speech because they are comparable to the hand’s knuckles. Since the metatarsal bones’ elliptical or rounded surface approaches a shallow cavity (of the proximal phalanges), these joints are known as condyloid joints. The ball of the foot is made up of the area of skin just beneath the joints.
Introduction
The synovial joints that bind the foot’s metatarsal bones to the proximal phalanges of the toes are called metatarsophalangeal joints (MTP). The bases of the proximal phalanges and the heads of the metatarsals articulate at these joints.
During the stance phase of the gait cycle, or walking, the metatarsophalangeal joints—condyloid joints—permit flexion, extension, abduction, adduction, and circumduction. The capsuloligamentous and musculotendinous structures that are connected to the metatarsophalangeal joints stabilize them.
Anatomy
- The articulation of the metatarsophalangeal (MTP) joints is ball-and-socket. There is a noticeable dorsal lip on the proximal phalanx.
- At the crista or plantar aspect of the metatarsal head, the first MTP joint features paired sesamoids with unique articulations.
- The first MTP joint features tiny dorsal and plantar recesses and connects to the sesamoid articulations.
- The smaller dorsal and larger plantar capsular recesses of the second through fifth, or lesser, MTP joints go from the metatarsal necks to the bases of the proximal phalanges.
- Along the midline of the joints, the extensor tendons run.
- Medial and lateral to the bones and joints are the dorsal digital nerves and arteries.
Articular surfaces
The rounded heads of the metatarsal bones and the shallow concavities on the bases of the proximal phalanges articulate to form the metatarsophalangeal joints. Mostly covering the distal and plantar sides, the articular surface of the metatarsal bone heads is vertically convex. At these joints, plantar flexion is made possible by the prominent plantar articular surface. Additionally, the first metatarsal bone’s head is transversely convex, which permits a greater degree of abduction and adduction than the other toes.
Two distinct facets, separated by an anteroposteriorly oriented ridge, make up the unique plantar articular surface of the first metatarsal head. A smaller lateral facet occupies the remaining one-third of the palmar articular surface, while a larger medial facet covers roughly two-thirds of it. The sesamoid bones of the big toe’s plantar ligament/plate articulate with these.
In a similar vein, the metatarsophalangeal joints of the second and fifth toes may or may not have a sesamoid bone.
Joint capsule and ligaments
A synovial membrane lines the flexible joint capsule that envelops each metatarsophalangeal joint and joins near the articular borders. Collateral ligaments on both sides and a plantar ligament on the plantar aspect support this fibrous capsule. These ligaments are crucial to the capsule. Fibers from the extensor tendons strengthen the capsule’s thin dorsal surface.
The metatarsophalangeal joint is connected to three different kinds of ligaments: deep transverse metatarsal, plantar, and collateral ligaments.
Collateral ligaments
Each metatarsophalangeal joint has collateral ligaments on both the medial and lateral sides. From the tiny dorsal tubercles on either side of the metatarsal heads to the corresponding side of the phalangeal bases (phalangeal collateral ligament) and the plantar ligament distally (accessory collateral ligament), these robust ligaments extend obliquely, or inferodistally.
Plantar ligaments
The dense fibrocartilaginous plates known as plantar ligaments (or plantar plates) are securely fastened to the phalangeal bases’ plantar surfaces. The plantar ligaments’ dorsal surfaces, which are a component of the metatarsal heads’ articular surface, are somewhat concave. These ligaments’ edges mix in with the deep transverse metatarsal ligaments and the collateral.
A groove in the plantar portions of the plantar ligaments allows the flexor tendons to pass through to the toes. The sesamoid bones and their ligamentous bands, which create a canal for the tendon of the flexor hallucis longus muscle, largely replace the plantar ligament of the first digit.
Deep transverse metatarsal ligaments
Four short, broad bands called the deep transverse metatarsal ligaments to connect the plantar ligaments of neighboring metatarsophalangeal joints to form a single unit. They stop the forefoot from splaying or expanding. The tendons of the lumbrical muscles, digital vessels, and nerves on the plantar surface, as well as the dorsal interossei tendons, enclose these ligaments.
Innervation
The metatarsophalangeal joints are primarily supplied by the plantar digital nerves. The first, second, third, and medial halves of the fourth metatarsophalangeal joint are all supplied with plantar aspects by the medial plantar nerve. Digital branches of the lateral plantar nerve innervate the fifth joint and the lateral portion of the fourth joint.
The medial side of the first metatarsophalangeal joint is one of the digital branches of the superficial fibular (peroneal) nerve that primarily supplies the metatarsophalangeal joints on the dorsal aspect. The deep fibular nerve’s digital branches innervate just the medial side of the second metatarsophalangeal joint and the lateral side of the first metatarsophalangeal joint.
Nerve Supply
- Sensory and motor functions are provided by the medial and lateral plantar nerves, which are branches of the tibial nerve.
- Dorsiflexor muscles are supplied by the deep peroneal nerve.
Blood supply
As branches of the dorsal pedal artery, the dorsal metatarsal arteries supply blood to the metatarsophalangeal joints on the dorsal surface.
The plantar metatarsal arteries, which emerge from the deep plantar arch, provide the arterial blood supply to the plantar portions of the metatarsophalangeal joints.
These two arteries—the deep plantar artery from the dorsal pedal artery and the lateral plantar artery from the posterior tibial artery—combine to form the deep plantar arch.
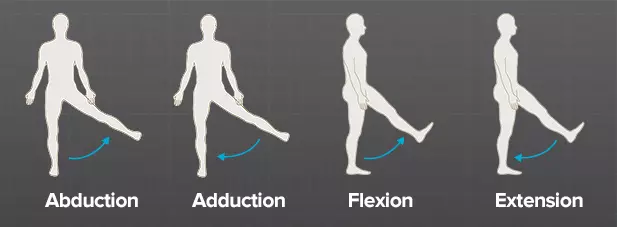
Movements
Flexion, extension, and limited abduction, adduction, and circumduction are all made possible by the metatarsophalangeal joints. There are two degrees of freedom in each joint.
The metatarsophalangeal joints flex (plantarflex), which pulls the toes together and bends them toward the plantar portion of the foot. Flexor tendons that run to the digits are responsible for this motion. About 45° of range of motion is permitted by the first metatarsophalangeal joint during active flexion, while about 40° is permitted by the lateral four metatarsophalangeal joints.
Extensor tendons that travel to the digits are responsible for the extension (dorsiflexion) of the metatarsophalangeal joints. The toes are slightly spread out and pointed laterally when the metatarsophalangeal joints are actively extended, elevating them toward the dorsal surface of the foot. About 70° of extension is possible in the first metatarsophalangeal joint, but only about 40° is possible in the lateral four metatarsophalangeal joints.
At full extension, the metatarsophalangeal joints are in a close-packed posture; at 10° extension, they are in an open-packed position. These joints’ capsular pattern, or loss of passive range of motion during inflammation, varies, although, in the case of the big toe’s metatarsophalangeal joint, it is typically thought to be more limited in extension than flexion.
There is very little abduction or adduction at the metatarsophalangeal joints, and it happens to the second digit, which acts as the midline.
Certain auxiliary movements may be evoked during passive movement of the metatarsophalangeal joints. These include rotation of the bases of the proximal phalanges over the metatarsal heads and minor sliding (up and down).
Muscles acting on the metatarsophalangeal joint
Muscles in the leg and foot are responsible for all motions of the metatarsophalangeal joints.
- The flexor hallucis longus, flexor hallucis brevis, and oblique head of the adductor hallucis muscle are the main muscles responsible for flexing the first digit (great toe) at the MTP joint. The lubricants, dorsal and plantar interossei, and flexor digitorum brevis are the primary muscles involved in flexing the lateral four digits. The flexor digitorum longus and the quadratus plantae support them, whereas the flexor digiti minimi brevis aids in the fifth digit.
- The extensor hallucis longus muscle is responsible for extending the first digit’s MTP joint. The extensor digitorum longus and extensor digitorum brevis muscles are responsible for the extension of digits two through five.
- The adductor hallucis muscle is responsible for the adduction of the MTP of the first digit, while the homologous plantar interossei perform the same function for the digits three through five.
- The abductor hallucis muscle performs abduction of the first digit, whereas the abductor digit minimi muscle produces abduction of the fifth digit. The dorsal interossei muscles are responsible for the abduction of the MTP of digits two through four.
Clinical significances
The metatarsophalangeal (MTP) joint is vital for walking, balance, and weight-bearing. This joint’s dysfunction or damage can result in severe pain, problems moving about, and deformities. Key clinical conditions of the MTP joint are listed below:
1. Hallux Valgus (Bunion)
Hallux Valgus (Bunion):
- A lateral displacement of the big toe with expansion of the 1st MTP joint.
- Typical of those who wear high heels or small shoes.
- May lead to pain, edema, and difficulty walking.
2. Hallux Rigidus
- First MTP joint arthritis, resulting in discomfort and stiffness.
- Common in athletes who suffer from repetitive stress injuries or in older persons.
- Makes walking more difficult during the push-off phase.
3. Turf Toe
- A hyperextension injury of the 1st MTP joint, affecting the plantar plate and ligaments.
- Common among athletes, particularly those who play football, soccer, or gymnastics.
- Reduces mobility and causes pain and edema.
4. Metatarsalgia
- The MTP region experiences pain and inflammation as a result of the metatarsal heads being under too much strain.
- Causes include high-impact sports, inappropriate footwear, and excessive use.
5. Sesamoiditis
- Sesamoid bone inflammation beneath the first MTP joint.
- Common among dancers, runners, and those with high arches.
6. Rheumatoid Arthritis (RA)
- Impacts the MTP joints, particularly those numbered two through five.
- Causes instability, discomfort, and joint abnormalities.
7. Gout
- The first MTP joint is frequently affected by uric acid crystal deposition (“Podagra”).
- Causes swelling, redness, and abrupt, intense pain.
8. Claw Toe & Hammer Toe
- Abnormalities affecting the interphalangeal and MTP joints.
- Causes include long-term pressure, ill-fitting shoes, and neuromuscular disorders.
9. Freiberg’s Disease
- The second or third metatarsal head may have avascular necrosis or bone death.
- Common in female adolescents.
- Pain, stiffness, and restricted movement are the symptoms.
10. Capsulitis of the MTP Joint
- The second MTP joint is typically affected by joint capsule inflammation.
- Frequently brought on by too much forefoot pressure.
FAQs
The metatarsophalangeal joints: what are they?
Approximately 2 cm from the toe webs are the ellipsoid synovial joints known as the metatarsophalangeal (MTP) joints. The plantar ligament (plate) on the plantar surface and the collateral ligaments on either side reinforce their capsule.
What is meant by medical joint (MTP)?
Turf toe, also known as metatarsophalangeal (MTP) joint sprain, is a sprain of the great toe plantar ligament complex. Both active and passive motion of the enlarged joint cause pain.
In the foot, what does MTP mean?
In your big toe, the first metatarsophalangeal (MTP) joint is located. The first MTP joint fusion is a surgical treatment used to treat big toe arthritis, also called hallux rigidus, which can cause discomfort and swelling and make it difficult to run, walk, and wear shoes.
The first MTP joint is where?
The base of the big toe is where the First Metatarsophalangeal joint is situated. When walking, this joint facilitates toe-off. This is frequently the location of arthritic changes in the joint or a bunion.
What is the purpose of MTP?
The abortion pill, sometimes referred to as medical termination of pregnancy (MTP), is a type of abortion that involves taking one or two medications.
MTP joint pain: what is it?
In many cases, metatarsalgia is caused by pain in the metatarsophalangeal joint. The most frequent cause of metatarsophalangeal joint discomfort is misalignment of the joint surfaces due to changes in foot biomechanics, which can lead to capsular impingement, flexor plate rips, joint subluxations, and osteoarthrosis, or the breakdown of joint cartilage.
How is pain in the first MTP joint treated?
The arthritis cannot be cured, but it may be less painful if orthotics are tried to relieve pressure beneath the joint or if shoes are modified to limit movement through the joint. Anti-inflammatory drugs and paracetamol, two other common analgesic regimens, might also be beneficial.
References
- Metatarsophalangeal (MTP) joints. (2023, October 30). Kenhub. https://www.kenhub.com/en/library/anatomy/metatarsophalangeal-mtp-joints
- Wikipedia contributors. (2024b, September 10). Metatarsophalangeal joints. Wikipedia. https://en.wikipedia.org/wiki/Metatarsophalangeal_joints