
Lisfranc Injury (Midfoot)
What is a Lisfranc Injury?
A Lisfranc injury involves damage to the midfoot, specifically the ligaments or bones connecting the forefoot and hindfoot. It can result from trauma, such as falls, sports injuries, or car accidents, leading to pain, swelling, and difficulty bearing weight. Early diagnosis and treatment are crucial to prevent complications like chronic pain or arthritis.
If the ligaments supporting the midfoot have been cut or the midfoot bones are damaged, lisfranc (midfoot) injuries occur. Jacques Lisfranc de St. Martin, a French physician who served in the Napoleonic army in the 1800s, coined the phrase “midfoot fracture dislocations” after observing midfoot injuries in cavalry soldiers.
From a straightforward injury affecting a single midfoot joint to a complicated lesion involving several midfoot joints and fractured bones, the severity of a Lisfranc injury can vary greatly.
It is easy to mistake a basic Lisfranc injury with a sprain, particularly if it results from a simple twist and fall.
A Lisfranc joint injury, however, is not a straightforward sprain that can be “walked off” or anticipated to recover swiftly. Even a little Lisfranc injury may be quite serious, taking months to heal and perhaps requiring surgery.
Anatomy of Lisfranc (Midfoot)
The midfoot is the middle part of the foot, where the arch on top of the foot is formed by a group of tiny bones. Five long bones (metatarsals) stretch from this cluster to the toes.
Strong ligaments called the Lisfranc joint complex run across and down the foot, holding the bones in place. Nevertheless, the first and second metatarsals are not joined by any connective tissue. These bones can be broken or dislocated by a twisting fall.
The midfoot transfers the forces produced by the calf muscles to the front of the foot during walking, and the Lisfranc joint complex, which has very little motion, is essential for stabilizing the arch for push off during walking (gait). If a Lisfranc injury is not treated, the arch may continue to be unstable, which could cause the foot to collapse or flatten.
Epidemiology of Lisfranc (Midfoot) Injury
Lisfranc joint injuries fall into one of two categories: low energy or high energy. Trauma can result in direct or indirect injuries. Because of their rarity and anatomical complexity, joint injuries are frequently overlooked.
High-energy injuries such as from motor vehicle accidents or crush injuries are not related with any specific damage pattern. High energy injuries are linked to poorer outcomes. A Lisfranc injury can also result from direct trauma, such as a fall from a height, but low-energy injuries typically happen indirectly, when an axial or rotational load is applied to a plantarflexed foot, causing hyperplantarflexion of the foot and tearing the weak dorsal ligaments.
Numerous foot fractures and dislocations may arise from these high-energy traumas. The prevalence is high among football players. Due to their increased participation in high-speed sports, men are two to four times more likely to get a Lisfranc joint injury . The third decade of life is when the damage is most prevalent.
Anatomical variations that increase the incidence of Lisfranc injury include a short second metatarsal and a shallow mortise for the second torso-metatarsal joint.
Causes of Lisfranc injury
A simple twist and tumble can result in a low-energy Lisfranc injury. One player landing on the back of another’s foot as the foot is extended downward in the push-off position is another typical occurrence among football and soccer players.
Direct trauma, such a car accident or a fall from a height, causes more serious injuries. Multiple foot fractures and joint dislocations, as well as damage to the spine and other limbs, can happen in these high-energy lisfranc injuries.
Symptoms of Lisfranc (Midfoot) Injury
Whether or whether you have a fracture, lisfranc injuries frequently cause the following symptoms on or around the top of your foot:
- Pain.
- Swelling, particularly in the area of the instep, or inside edge.
- You may also have bruises on the bottom of your foot.
- You are unable to place any weight on your foot: If you experience any discomfort, you may still have a Lisfranc injury even if you are able to place some weight on your foot.
- Expansion of the midfoot region
- Big lump in the upper midfoot region
Differential diagnosis of Lisfranc injury
- Calfunction of the posterior tibialis tendon.
- Cuboid fracture.
- Metatarsal fracture.
- Midfoot sprain.
- Navicular compression injuries.
Diagnosis
Medical History and Physical Examination
Your doctor will check your foot and ankle after discussing your symptoms and concerns with you. None of the physical examinations the doctor will conduct will exacerbate the injury, despite the possibility of some discomfort.
Your doctor will specifically check for the following:
- Your foot is bruised around the bottom. This points to either a midfoot fracture or a total rupture of the midfoot ligaments.
- Midfoot tenderness to pressure (palpation).
- An examination of the midfoot under stress reveals pain. To find out if you have midfoot discomfort, the doctor could grab your heel and twist the front of your foot. Your undamaged foot shouldn’t hurt from this.
- The “piano key” test causes pain. To find out if this hurts, the doctor could grab your toes and move them up and down. If there is an injury, this will cause discomfort since it places stress on the midfoot.
- heel rise in one limb. It’s possible that the doctor will urge you to stand on one foot and rise on your “tip toes.” This is helpful if the injury is minor and puts a lot of strain on the midfoot. Your unaffected foot shouldn’t hurt during this examination.
Imaging Tests
The following further tests might be prescribed by the physician to help confirm your diagnosis:
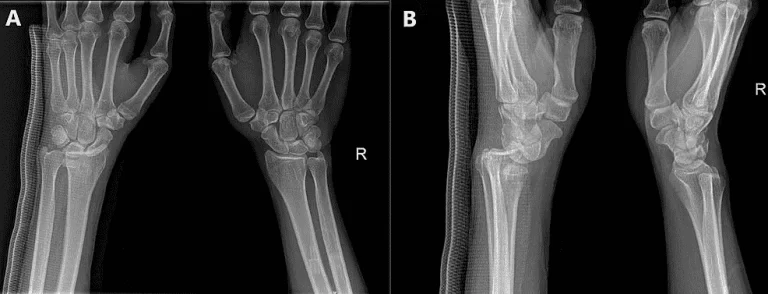
X-rays:
In an X-ray picture, broken bones and their locations can be observed. The Lisfranc joint’s alignment can also be seen on an X-ray. Any deviation from the joint’s typical position might indicate ligament damage.
The doctor can request that the patient stand for an X-ray if the injury was caused by a straightforward twist and fall, which is known as a low-energy injury. Given that the bones are not anticipated to be damaged, the doctor is searching for a ligament injury in this instance.
A standing (weightbearing) X-ray won’t exacerbate existing injuries, and if it is performed, an injury that might be managed non-surgically won’t worsen to the point where surgery is required.
In order to evaluate the alignment of the bones in the damaged foot with the unaffected side, the doctor might also take X-rays of your uninjured foot.
Magnetic resonance imaging (MRI) scan:
Your doctor may prescribe an MRI scan since it can be challenging to diagnose minor Lisfranc injury. The soft tissues around the bone, such as the ligaments damaged in a Lisfranc injury, are better seen by MRI images. Although it is not necessary to do this test in order to detect a Lisfranc injury, it might be useful in situations when the diagnosis is unclear.
CT scan:
CT scans may produce 3-D renderings and cross-sectional pictures of the damaged foot and are more detailed than X-rays. A CT scan may be ordered by your orthopaedic surgeon to aid in surgical planning since it will assist determine the precise degree of the injury and the number of joints affected. To diagnose or treat a Lisfranc injury, however, this test is not necessary.
Treatment of Lisfranc (Midfoot) Injury
The degree of a Lisfranc injury determines how it should be treated.
Nonsurgical Treatment of Lisfranc injury
Nonsurgical therapy may be sufficient for healing if the joint is free of fractures or dislocations and the ligaments are not totally ripped.
Wearing a non-weightbearing cast or boot for six to eight weeks is part of a nonsurgical treatment regimen. During this time, you have to be extremely careful not to place any weight on your wounded foot. The next step is weightbearing in an orthotic or a detachable cast boot.
To make sure your injury is healing properly, your doctor will want to take further X-rays and follow up with you on a frequent basis. Surgery will be required to realign the bones in the damaged joint if there is any indication during follow-up that they have shifted.
Surgical Treatment of Lisfranc injury
For injuries involving displaced fractures (broken bones) or aberrant joint placement (instability), surgery is advised. Realigning the joints, putting the broken bone pieces back in their proper positions, and giving the midfoot stability are the objectives of surgical therapy.
Lisfranc injuries can be treated using these methods:
Open reduction internal fixation (ORIF).
The surgeon makes an incision on the top of the foot, positions the bones correctly (reduction), and fastens them with plates or screws; some or all of this hardware may need to be removed later, which may be three to five months after surgery, depending on the surgeon’s judgment, because the plates or screws will be placed across joints that typically have some motion.
Sometimes the hardware breaks before it can be taken out. When screws or plates span bones with some mobility, this is common. Similar to how a paperclip will break after being bent repeatedly, metal can become fatigued and fail in certain circumstances. Even though part of the hardware may break, the procedure is frequently successful.
Midfoot fusion.
Fusion of the affected midfoot bones may be suggested as the surgical therapy for certain people and Lisfranc injury types. In essence, the purpose of fusion surgery is to realign the damaged bones and allow them to heal together, eliminating the need for a joint between them.
Fusion may be a suitable treatment to relieve discomfort and restore function to the midfoot because the joints of the midfoot have relatively little mobility to begin with.
In order for the bones to heal together, the surgeon removes the cartilage from the bones and compresses them together using metal plates, screws, or staples. Since the joints are fused and will not move until they heal, it is usually not necessary to remove the hardware.
Physical therapy of lisfranc injury
Early Immobilization:
In order to facilitate the first healing process following a Lisfranc injury, the foot must be completely immobile. This may require wearing a cast, a boot, or using crutches to keep weight off the affected
Pain management:
In the early phases of recovery, pain management is essential. To aid with pain and inflammation, physiotherapists may employ techniques like massage, electrical stimulation, or cold.
Range of Motion (ROM) Exercises:
To avoid joint stiffness, physiotherapists will begin mild range of motion exercises once the initial pain and swelling have decreased. Toe wiggles, ankle pumps, and mild foot and ankle stretches are a few examples of these exercises.
Strengthening Exercises:
Toe curls, heel lifts, and resistance band exercises are among activities that may be used to strengthen the muscles surrounding the Lisfranc joint, which is crucial for stability and support.
Training for Proprioception and Balance:
Lisfranc injuries can impact both proprioception, or the sense of one’s body’s posture in space, and balance. Proprioception and balance may be enhanced by performing balancing exercises on both stable and unstable surfaces.
Gait Training:
It’s essential to regain the ability to walk correctly. To avoid additional issues, physiotherapists work with patients to make sure they walk with the proper gait pattern.
Functional Training:
To help you safely return to your desired level of activity, functional exercises that are adapted to your needs—such as movements unique to your sport—will be introduced as your rehabilitation progresses.
Patient Instruction:
It’s critical to comprehend your ailment and the significance of following your physiotherapy regimen. Your physiotherapist will teach you self-management skills, activity moderation, and appropriate footwear.
Gradual Return to Activity:
Under a physiotherapist’s supervision, a person should resume sports or other physically demanding activities gradually. Physiotherapists evaluate preparedness and guarantee safe advancement.
FAQs
For what reason is it known as a Lisfranc injury?
If the ligaments supporting the midfoot are ripped or the midfoot bones are damaged, lisfranc (midfoot) injuries occur. Named for French physician Jacques Lisfranc de St. Martin, who saw midfoot injuries in cavalry troopers during the Napoleonic era in the 1800s, midfoot fracture dislocations
Lisfranc: is it a ligament or a bone?
Connecting the midfoot and forefoot are the bones and ligaments that make up the Lisfranc joint complex. Lisfranc injuries include bone fractures and dislocations, as well as ligament rips and strains (far right).
Is it possible to walk after suffering a Lisfranc injury?
A serious injury can cause the foot to become deformed, making it extremely uncomfortable to put any weight on it. A little injury could make the foot seem normal, and you might be able to walk on it with relatively slight discomfort.
Will Lisfranc recover by itself?
Lisfranc injuries are unlikely to go away on their own and, if ignored, can cause arthritis, instability, chronic pain, arch collapse, and even paralysis.
Is Lisfranc considered a disability?
Although lisfranc injuries are uncommon—roughly 1 in 55,000 Americans get one each year—they are far too frequently misdiagnosed or written off as a straightforward sprain. Osteoarthritis, altered gait, persistent foot discomfort, and long-term impairment might result from incorrect or nonexistent treatment.
References
- Stamatiou, N. (2023, December 8). Lisfranc Injuries and Physiotherapy Management – Brisbane Physiotherapy & Podiatry. Brisbane Physiotherapy & Podiatry. https://www.brisbanephysiotherapy.com/news/lisfranc-injuries-physiotherapy
- Lisfranc (Midfoot) injury – OrthoInfo – AAOS. (n.d.). https://orthoinfo.aaos.org/en/diseases–conditions/lisfranc-midfoot-injury/
- Lisfranc Fracture. (2025, January 24). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/22237-lisfranc-fracture


One Comment