Interspinous Ligament Sprain
Introduction:
An interspinous ligament sprain refers to injury or overstretching of the interspinous ligaments, which are located between the spinous processes of the vertebrae in the spine. These ligaments help stabilize the spine, especially during flexion (forward bending).
The term “interspinous ligament sprain” describes damage or overstretching of the bands of fibrous tissue that link the spinous processes of neighboring vertebrae in the spine. These ligaments are essential for maintaining the spinal column’s stability and preventing excessive flexion, or forward bending.
Sprains usually result in localized back pain, stiffness, and tenderness between the affected vertebrae and are caused by trauma, abrupt or repetitive motions, or inappropriate lifting techniques.
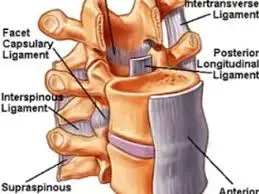
Its fibers attach to the ligamentum flavum anteriorly and the supraspinous ligament posteriorly, respectively. The ligaments are only marginally developed in the neck, broader, thicker, and quadrilateral in shape in the lumbar area, and narrow and elongated in the thoracic region. They are frequently regarded as a component of the nuchal ligament in the neck.
Clinical Relevance Anatomy:
Different levels of the interspinous ligaments’ (ISL) fibers line in different directions. As one moves from the upper to the lower interspinous areas, the fiber orientations progressively shift from horizontal to vertical. Additionally, the ISL fibers vary in thickness at various lumbar spine levels, and their orientation and thickness may indicate a variety of functions.
Although post-mortem examinations have revealed that the core regions of the interspinous ligament are commonly deteriorated, it is uncertain if these lesions cause pain. Because of this, the interspinous ligament becomes a desirable source of low back pain.
Causes of Interspinous Ligament Sprain:
A typical cause of interspinous ligament sprain is sudden or severe forward bending (flexion) of the spine, which causes the ligament to become overstretched or torn. Heavy lifting, sudden twisting actions, and trauma, like a fall or auto accident, can all cause this.
The ligament may gradually weaken and eventually sprain as a result of repetitive tension from bad posture, particularly when sitting or bending for extended periods. Due to repetitive spinal stress and inadequate core stability, athletes and people engaged in physically demanding work are at especially high risk.
Symptoms of Interspinous Ligament Sprain:
Localized pain in the mid or lower back, usually felt between the spinous processes of the vertebrae, is the main sign of an interspinous ligament sprain. Depending on how severe the sprain is, this pain may accompany a dull soreness or an acute pain that usually gets worse with forward bending, twisting, or extended sitting.
Additionally, patients may have decreased range of motion, pain to the touch along the spine, and stiffness in their muscles. In certain instances, the back may feel slightly swollen or unsteady when moving.
Risk Factors of Interspinous Ligament Sprain:
The spinal ligaments are continuously stressed by poor posture, particularly when sitting for extended periods or bending over and over. People who perform manual labor, heavy lifting, or high-impact sports are more vulnerable because they frequently bend and strain their spines.
In addition to lowering spinal stability, weak core muscles and a lack of flexibility can also increase the ligaments’ susceptibility to damage. The risk of sprain is further increased by age-related degeneration, prior spinal injuries, and inappropriate lifting techniques.
Diagnosis of Interspinous Ligament Sprain:
A comprehensive clinical evaluation, which includes a medical history and physical examination to determine the location of pain, tenderness between spinous processes, and mobility limits, is usually the first step in diagnosing an interspinous ligament sprain. In order to replicate symptoms and evaluate spinal stability, specific tests might be conducted. While MRI is the best method for observing soft tissue injuries, such as ligament sprains, imaging tests like X-rays are frequently utilized to rule out fractures or problems with spinal alignment.
Special Test for Interspinous Ligament Sprain:
Spring Test (Posterior-Anterior Vertebral Pressure Test):
A clinical examination designed to evaluate the mobility and integrity of spinal segments, the Spring Test (sometimes called the posterior-anterior vertebral pressure test) is especially helpful in the diagnosis of interspinous ligament sprains. The patient rests in a prone posture throughout the test, and the examiner gently presses down on each vertebra’s spinous processes.
The goal of this pressure is to give the vertebrae a spring-like mobility. Localized pain, soreness, or unusual movement at a particular spinal level, which could indicate a sprain, inflammation, or instability of the interspinous ligaments or surrounding structures, is a sign of a positive test.
Spurling’s Test:
A clinical test called Spurling’s Test is used to evaluate cervical nerve root compression, which is frequently linked to diseases such as cervical radiculopathy. The patient is seated throughout the test, and the examiner applies downward axial pressure to the head after gently extending and laterally flexing the patient’s neck toward the affected side. This test aids in distinguishing between nerve root involvement and localized neck pain.
The Transverse Ligament Test:
The cervical spine’s stability, specifically the transverse ligament that supports the odontoid process (dens) against the atlas (C1 vertebra), is evaluated with the transverse ligament test. The patient lies supine during the test, and the examiner gently presses the occiput anteriorly while lifting the head and neck slightly off the table.
This pressure may result in aberrant movement between the first and second cervical vertebrae (C1 and C2) if the transverse ligament is unstable or injured. This can induce symptoms like nausea, dizziness, or an unsteady feeling. A positive test raises the possibility of atlantoaxial instability, a dangerous condition that needs more assessment and care.
Rib Springing Test:
The purpose of the Rib Springing Test is to evaluate rib mobility and identify any limitation or dysfunction in the rib cage and thoracic spine. The examiner applies a light, oscillatory pressure to the ribs during the test, usually starting at the lower ribs and working their way upwards while the patient is seated or supine.
In an attempt to spring or move the ribs, the examiner exerts pressure on the rib cage. Localized rib pain, stiffness, or limited movement is a sign of a positive test and could be a sign of thoracic spinal misalignment, intercostal muscle tension, or rib dysfunction. Rib subluxations and costovertebral joint dysfunction can be diagnosed using this test.
Lumbar Ligament Stress Test:
The posterior longitudinal ligament, supraspinous ligament, and interspinous ligaments in particular are evaluated for stability and integrity using the Lumbar Ligament Stress Test. To check for ligamentous laxity or pain, the examiner places controlled tension or strain on particular regions of the lumbar spine while the patient is seated or in a prone position.
The test may include passive spine movement, such as flexion or extension, to assess how the ligaments react to tension. Pain, discomfort, or excessive movement at a certain spinal level, which suggests ligamentous damage, sprain, or instability, are signs of a positive test. This test is frequently used in combination with other diagnostic techniques to assist in determining possible causes of low back pain.
Sacral Spring Test:
A clinical test called the Sacral Spring Test is used to evaluate sacral mobility and sacroiliac joint dysfunction. Pain or limited movement in the sacroiliac joint, as in sacroiliitis or sacroiliac joint instability, are signs of a positive test and may indicate sacroiliac joint dysfunction or inflammation. The test aids in the diagnosis of lower back pain that may affect the sacrum.
Treatment of Interspinous Ligament Sprain:
The goals of treating an interspinous ligament injury are to lessen pain, encourage healing, and stabilize the spine. Rest, applying ice to reduce inflammation, and taking painkillers or anti-inflammatory drugs as prescribed by a healthcare professional are all part of the initial therapy.
Physical therapy, which uses methods including soft tissue release, manual therapy, and mild spinal mobilization to reduce pain and increase mobility, is essential to the healing process. Supportive braces or more imaging may be necessary in severe or chronic instances in order to rule out other spinal injuries and direct future care.
Physical Therapy Treatment:
In order to promote healing and avoid further injury, the goal of physical therapy treatment for an interspinous ligament sprain is to decrease pain, increase mobility, and strengthen the surrounding muscles. In order to reduce pain and inflammation, the first line of treatment frequently consists of rest, cold therapy, and mild soft tissue mobilization. Spinal mobilizations are one type of manual treatment that can be used to increase joint mobility and reduce ligament strain.
Therapeutic activities that focus on the lower back and core muscles are added as the acute pain goes away in order to maintain the spine and strengthen the stabilizing muscles. Ergonomic training and postural correction are also crucial for preventing further ligament strain during regular tasks. Exercises that increase flexibility, particularly in the hip and back muscles, aid in reducing stiffness and restoring range of motion.
Advanced methods such as electrotherapy (TENS), heat therapy, or tape may be used in more chronic situations to help relax muscles and manage pain. A customized rehabilitation program is frequently developed to match each patient’s needs and activity level, and gradual progression is crucial during treatment to prevent re-injury.
Complications of Interspinous Ligament Sprain:
An interspinous ligament sprain can cause several problems if it is not treated appropriately. Chronic pain or persistent stiffness is one possible side effect that might restrict range of motion and interfere with day-to-day activities.
The affected area may become more vulnerable to other injuries if the ligament does not mend properly, which could lead to spine instability. Degenerative alterations in the spine, such as facet joint degeneration or early development of osteoarthritis, might result from repeated sprains or inadequate rehabilitation.
Muscle imbalances caused by the spine’s changed biomechanics can occasionally result in secondary disorders such nerve compression or muscle strains. To avoid these problems and encourage a full recovery, prompt and proper treatment, including physical therapy, is crucial.
Prevention of Interspinous Ligament Sprain:
It is crucial to maintain good posture and refrain from excessive spinal flexion or twisting motions to prevent an interspinous ligament strain. Regular workouts can improve spinal stability and lower the chance of ligament strain by strengthening the core muscles that support the spine. To avoid putting undue strain on the ligaments, proper lifting techniques such as bending the knees rather than the back are essential.
Maintaining a healthy range of motion and minimizing stiffness are two benefits of regular hip and lower back stretching and flexibility exercises. Overloading the spine can also be avoided by taking regular rests when standing or sitting for extended periods, especially when doing so in positions that are not ergonomically sound. The risk of suffering an interspinous ligament sprain can be considerably decreased by implementing these techniques into regular routines.
Prognosis:
When treated and rehabilitated appropriately, the prognosis for an interspinous ligament injury is usually excellent. When early intervention, including rest, physical therapy, and pain management, is started and the injury is minor, most people recover completely in a matter of weeks to months.
The ligament can recover with the right treatment, restoring normal spinal function. A lengthier recovery period and the possibility of chronic soreness or instability exist, though, in more severe cases or if the sprain occurs frequently. To avoid more problems, it is essential to regularly perform rehabilitation activities that strengthen the surrounding muscles and enhance posture. The sprain may result in persistent pain or spinal instability if treatment is not received or if rehabilitation is insufficient, which may impair mobility and quality of life.
Conclusion:
With the right care and rehabilitation, an interspinous ligament sprain, which is frequently a painful and restricting condition, can be effectively managed. Rest, physical therapy, and strengthening exercises are examples of early intervention that can speed up healing and restore spine function.
Even while most people heal completely with the right care, recurrence can be avoided with good lifting techniques, frequent exercise, and attention to posture. However, if the sprain is not treated, it may result in long-term issues like muscle imbalances, spinal instability, and persistent pain. To avoid these issues and guarantee the best possible recovery, prompt diagnosis and treatment are essential.
FAQs
After an interspinous spacer, how long does it take to recover?
You might be able to travel and do light activities as soon as you feel well after the minimally invasive operation to implant an interspinous spacer. You may even be able to return to your regular activities in as little as two weeks, depending on your particular situation.
What is the most recent interspinous spacer treatment for spinal stenosis?
By inserting a spacer between the vertebrae, a novel surgical procedure called lumbar interspinous distraction decompression (IDD) is drawing interest for its method of reducing nerve compression.
What is the interspinous spacer’s success rate?
With Superion and X-STOP, the percentage of participants who achieved ZCQ clinical success was 78% and 93% for patient satisfaction, 64% and 63% for physical function, and 75% and 53% for symptom severity.
Which joint is supported by the interspinous ligament?
Attaching from the base to the apex of each spinous process, this thin ligament blends dorsally with the supraspinous ligament and ventrally with the ligamenta flava.
For whom are interspinous spacers appropriate?
Interspinous spacer therapies may be appropriate for patients with leg pain and spinal stenosis.
What dangers can interspinous spacers pose?
Screw misalignment, unintentional durotomy (leakage of cerebrospinal fluid [CSF]), infection, deep vein thrombosis, and postoperative anemia are a few of the problems. Interspinous process devices and minimally invasive lumbar decompression were developed as a result of these worries.
How long does it take to recover after an interspinous spacer?
While complete recovery may take several months, depending on personal healing variables, most patients can anticipate returning to modest activities in a few weeks.
How is edema of the interspinous ligament treated?
The standard first-line therapies for cervical interspinous bursitis include steroid injections and oral or intravenous anti-inflammatory drugs. Pain alleviation may result from surgical resection of the bursa in situations that are unresponsive to conventional treatment.
Is it possible to heal spinal ligaments?
Injections: Injections of corticosteroids can relieve pain and lower inflammation. Minimally Invasive Procedures: Endoscopic spine surgery is one technique that can repair the ligament in severe situations with less tissue damage and quicker recovery times.
How much time does it take for spinal ligaments to heal?
Ligament injuries typically result from a traumatic occurrence, and their healing time might range from six weeks to a year, depending on how severe the injury is.
References
- Creighton, A., Sanguino, R. A., Cheng, J., & Wyss, J. F. (2021). Successful treatment of supraspinous and interspinous ligament injury with Ultrasound-Guided Platelet-Rich plasma injection: Case Series. HSS Journal® the Musculoskeletal Journal of Hospital for Special Surgery, 17(2), 227–230. https://doi.org/10.1177/1556331621992312
- Patel, D. (2023e, July 29). Spinal ligament – anatomy, structure, function. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/spinal-ligament/
- Florence, T. J., Say, I., Patel, K. S., Unterberger, A., Laiwalla, A., Vivas, A. C., & Lu, D. C. (2022). Neurosurgical Management of Interspinous Device Complications: a case series. Frontiers in Surgery, 9. https://doi.org/10.3389/fsurg.2022.841134