Iliohypogastric nerve
Introduction
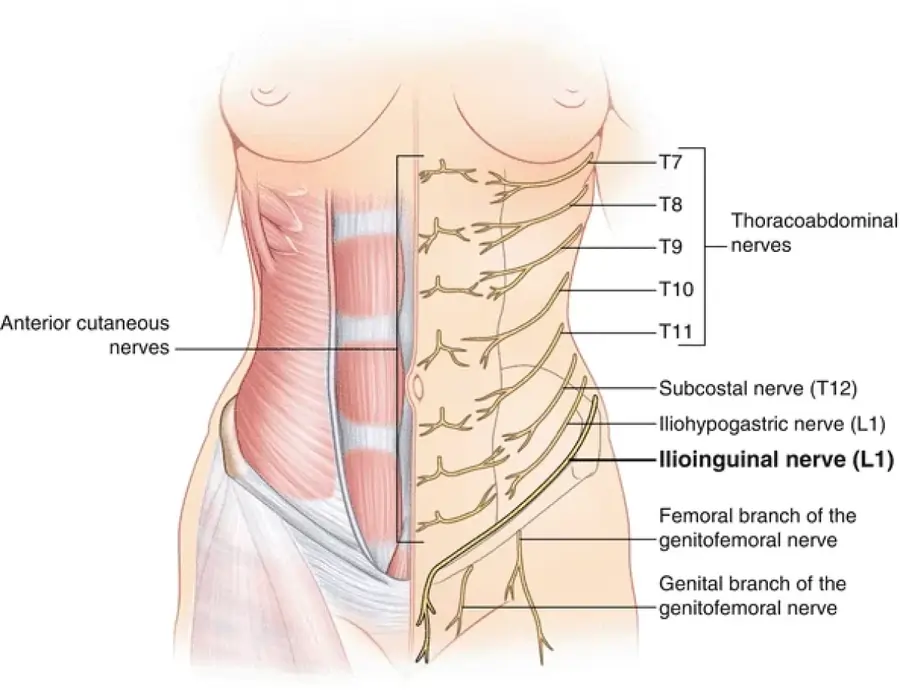
The iliohypogastric nerve is a branch of the lumbar plexus, originating mainly from the L1 spinal nerve. It provides motor innervation to the lower abdominal muscles (such as the internal oblique and transversus abdominis) and sensory innervation to the skin over the lower abdomen and upper hip (gluteal) region. It plays a role in abdominal wall strength and sensation.
Together with the ilioinguinal nerve, it emerges as a single trunk from the anterior/ventral ramus of the L1 spinal nerve root. After emerging from the upper border of the psoas major muscle, the nerve begins its journey on the posterior abdominal wall. After that, it runs between the anterior abdominal muscles and crosses obliquely to the anterior abdominal wall.
The iliohypogastric nerve, being a mixed nerve, provides sensory innervation to the skin of the posterolateral gluteal and suprapubic areas in addition to motor and sensory innervation to the abdominal muscles.
Structure
Origin
The superior branch of the anterior ramus of spinal nerve L1 is where the iliohypogastric nerve begins. Additionally, T12 sends fibers to it through the subcostal nerve.
Course
Together with the ilioinguinal nerve, the iliohypogastric nerve emerges from the anterior ramus of the L1 spinal nerve root of the lumbar plexus.
The iliohypogastric nerve goes inferolaterally, posterior to the lower pole of the kidneys and in front of the quadratus lumborum muscle, after emerging from the upper lateral border of the psoas major muscle.
The iliohypogastric nerve passes anteriorly between the internal abdominal oblique muscles and the transversus abdominis muscle, and posteriorly, immediately above the iliac crest, it pierces the transversus abdominis muscle as it travels towards the anterior abdominal wall.
Function
Sensory function
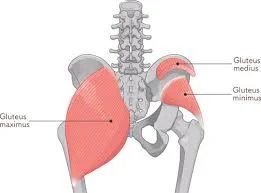
The transversus abdominis muscle, internal abdominal oblique, and external abdominal oblique all receive sensory fibers from the nerve. Additionally, the posterolateral part of the gluteal area and the skin of the suprapubic region are supplied by the iliohypogastric.
Motor function
Additionally, the transversus abdominis and the internal abdominal oblique muscles get motor fibers from the iliohypogastric nerve. Additionally, it innervates the conjoint tendon, which is a tendon made up of the internal oblique and transversus abdominis muscles’ shared aponeurosis.
Branches
The iliohypogastric nerve splits into the lateral cutaneous and anterior cutaneous branches when it passes between the transversus abdominis and internal abdominal oblique.
Lateral cutaneous branch
To feed the posterolateral portions of the gluteal skin, the lateral cutaneous branch penetrates the external and internal abdominal oblique muscles above the iliac crest.
Anterior cutaneous branch
The transversus abdominis and internal abdominal oblique muscles are innervated by the anterior cutaneous branch, which extends anteriorly between them. About 2 cm medial to the anterior superior iliac spine, it punctures the internal oblique muscle. This branch then supplies the skin above the pubic region by passing via the aponeurosis of the external abdominal oblique muscle, which is located around 3 cm above the superficial inguinal ring.
Communications
The subcostal and ilioinguinal nerves are in communication with the iliohypogastric nerve.
Variation
Up to 20% of persons may not have the iliohypogastric nerve. Rather, its fibres are transported by other nerves, such the ilioinguinal nerve.
Clinical Importance
Other nerves may be impacted, and iliohypogastric nerve damage is seldom isolated. An oblique open approach to the appendix during surgery can sometimes result in injury. Transverse incisions in the lower abdomen, such as those made after a hysterectomy, can also cause damage to the iliohypogastric nerve. Since many nerves innervate the suprapubic area, a discernible sensory loss is uncommon.
Nerve injuries can be caused by:
either as a result of acute surgical damage or after the surgery, when the nerve becomes trapped in scar tissue.
Sport-related injuries like muscular tears or trauma can potentially harm the nerve.
Rarely, pregnancy-related nerve damage might also happen because of the third trimester’s fast abdominal growth. The term “idiopathic iliohypogastric syndrome” describes this condition.
The suprapubic and inguinal areas may experience a searing pain if the iliohypogastric nerve is injured or trapped. A local anesthetic injection, painkillers such as anti-inflammatory drugs, or physical therapy like cryotherapy are the available treatment options.
The posterior wall of the inguinal canal may become weaker if the iliohypogastric nerve divides above the level of the anterior superior iliac spine. This may increase the risk of developing a direct hernia.
FAQs
What is the main function of the iliohypogastric nerve?
The iliohypogastric, ilioinguinal, and genitofemoral nerves have a primary sensory function, innervating the lower abdomen, inguinal region, the upper and medial anterior thigh, and part of the genitalia.
What happens if the iliohypogastric nerve is damaged?
The iliohypogastric nerve is a nerve that passes through the muscles of the lower abdomen, supplying sensation to the skin of the gluteal region and lower abdomen. Painful feelings or sensory deficiencies in these locations may arise from damage to this nerve.
How do you treat iliohypogastric nerve pain?
Damage to this nerve may result in pain or sensory deficits in these areas.
What are the complications of an iliohypogastric nerve block?
Vasovagal response (passing out), new or increased pain, infection, bleeding, lasting skin changes, allergic or unanticipated medication reaction with small or serious consequences, and unintentional nerve damage are some examples of potential dangers.
References
- Iliohypogastric nerve – 2024 – https://en.wikipedia.org/wiki/Iliohypogastric_nerve
- Iliohypogastric nerve – 2023 https://www.kenhub.com/en/library/anatomy/iliohypogastric-nerve