
Decorticate Posture
What is Decorticate Posture?
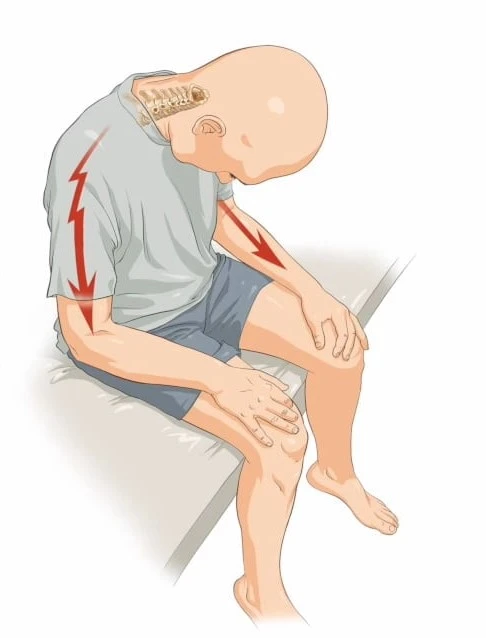
A patient in decorticate posture has an abnormal body posture in which their arms are stretched over their chest, their wrists are flexed, their fingers are squeezed and their legs are extended straight forward. The wrists and fingers are bent and rest on the chest, while the arms are bowed inward toward the torso. This kind of posture indicates serious brain injury.
Individuals with this illness ought to need immediate medical attention. It might affect one or both of the body’s sides.
Decorticate posture definition:
This abnormal posture, which is mostly caused by brain-related conditions, is defined by the body being in a stiff state with the lower extremities extended and the arms, fingers, and wrists flexed.
A patient with decorticate posturing, a form of pathological state in which they are able to regulate their body movement, needs to be seen by a doctor extremely once. It frequently serves as a warning sign for specific kinds of serious brain or spinal cord injuries.
Other terms for decorticate posture include flexor posturing, decorticate stiffness, decorticate reaction, and, informally, “mummy baby.”
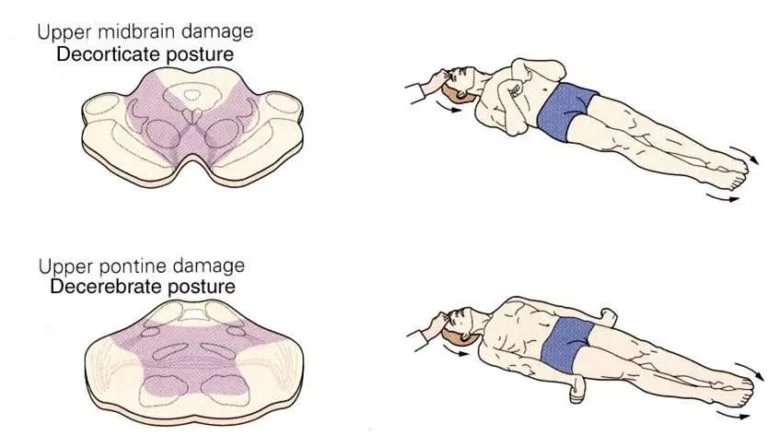
It is an indication of serious injury to the region of the midbrain, which lies between the spinal cord and the brain. Motor movement is controlled by the midbrain. Although decerebrate posture is more severe than decerebrate symptoms, the former is nevertheless a significant condition.
The bending of upper body muscles results in a score of three on the motor section of the Glasgow Coma Scale for a neuro-muscular response to trauma that displays decorticate posture in response to pain.
This position consists of two parts:
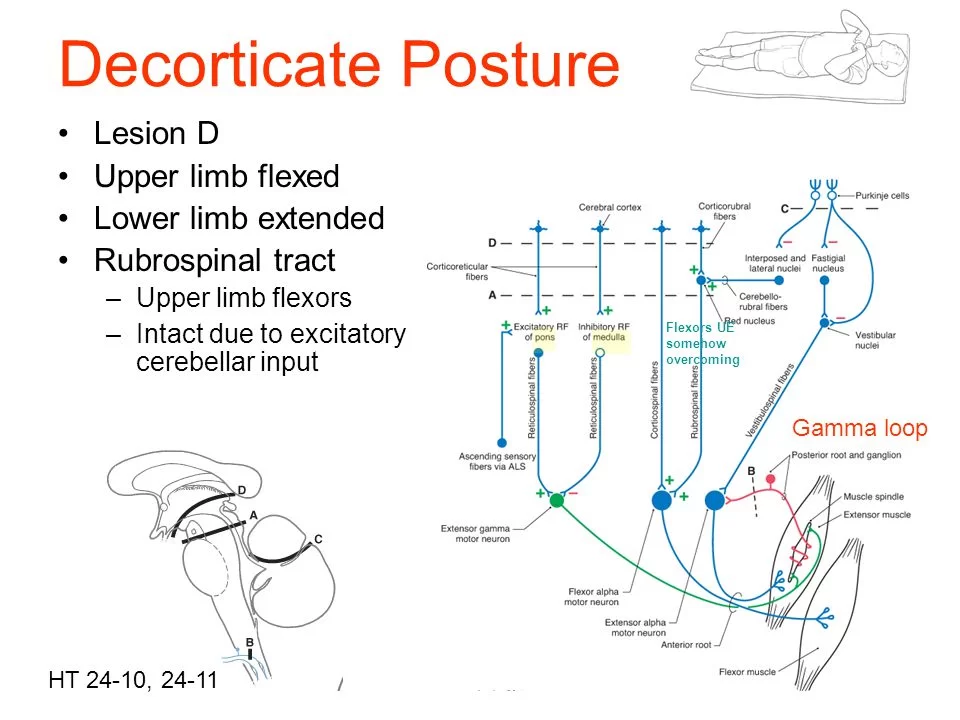
It is the inhibition of the red nucleus and simultaneous facilitation of the rubrospinal tract. The motor neurons in the cervical spinal cord that supply the flexor muscles of the upper limb are stimulated by the rubrospinal tract. While the medial and lateral vestibulospinal and pontine reticulospinal tracts are in charge of the extension posturing in the upper limb, the rubrospinal tract and medullary reticulospinal tract are creating the flexion kind of posturing.
The second aspect of this posture involves the complication of the lateral corticospinal tract, which activates the motor neurons in the lower spinal cord that supply the flexor muscles of the lower limb. Simultaneously, the stimulation of the lower limb’s extension movement is greatly enhanced by the pontine reticulospinal and the medial and lateral vestibulospinal tracts, which in turn activate the medullary reticulospinal tract.
The flexion posture in the upper limb and the extensor posture in the lower limb are mostly caused by lesions above the red nucleus in these two pathways.
This atypical position indicates the possibility of significant harm to the cerebral hemispheres, internal capsule, and thalamus. Another possibility is midbrain injury. The red nucleus is also affected, suggesting a lesion lower in the brainstem, and this position is often suggestive of more serious damage at the rubrospinal tract.
Your body may adopt a decorticate stance on auto-pilot if there is a brain injury or other interruptions. It is a sign of several medical disorders as well as brain traumas.
Certain muscular groups in your body become rigid instinctively during decorticate posture. It may impact one or both of the body’s sides. When it impacts both parties, though, it’s not necessarily the same. The effects might be inconsistent on both sides of the body.
Reflexive decorticate posture occurs. It does not feature the uncontrollably moving motions of a seizure. Usually, it’s a reaction to unpleasant feelings instead (which is part of assessing reflexes in a neurological exam).
The following are possible symptoms of decorticate posturing:
- Stiff, extended legs.
- Toes bent slightly inward and directed away from the torso.
- Bend your elbows upward and point your arms toward your midsection.
- wrists curled.
- clasped hands pressed against the chest and together.
Epidemiology
Publications regarding the prevalence of abnormal posing are nonexistent. The prevalence of diseases that frequently result in decorticate and decerebrate posture is known, nonetheless. Traumatic brain injury (TBI) is the most prevalent cause of decorticate and decerebrate posture. According to a 2019 systematic study, there are 69 million TBIs globally each year, of which 7.95% are considered serious. Those with a GCS of 8 or lower are considered to have had a severe TBI.
Pathophysiology
Anatomically speaking, the intercollicular line at the level of the red nucleus is often the divide linked to decorticate and decerebrate posture. This idea, however, has been challenged since, although the brainstem is usually affected, injuries in the supratentorial area can also result in both decorticate and decerebrate posture.
Despite being stereotyped, both posture styles can exist in different degrees and even asymmetrically, with one side decorticate and the other side decerebrate. A less severe degree of damage is typically suggested by an uneven presentation of a certain posture.
Decorticate Posturing
Compared to decerebrate posture, the process underlying decorticate posturing is less well understood. The area of the midbrain’s red nucleus is crucial for movement, according to phylogenetic analysis. In primates, the rubrospinal tract affects primordial grip reflexes, especially in young animals, and it also happens to be the reason why monkeys crawl.
The spinal motor neurons receive signals from the red nucleus via the rubrospinal tract. Since fine motor abilities are essential to primates, the motor cortex—via the corticospinal tracts—has a greater role in movement than lower, phylogenetically related regions. Decorticate posture has been linked to extensive lesions in the rostral midbrain, diencephalon, or forebrain.
The thalamus, internal capsule, corona radiata, motor cortex, and premotor cortex are included in this. Because the rubrospinal tract in primates only extends to the thoracic spine, it affects the upper limbs but not the lower. The upper limbs flex and make a clutching reflex, which is caused by the red nucleus through the rubrospinal tract. During normal physiology, the higher brain areas, such as the cerebral cortex, block this reaction.
A lesion to the corticospinal tract disinhibits the red nucleus and permits the upper limb flexion reflex to function normally. As was previously mentioned, the vestibulospinal pathways are likewise left uninhibited, resulting in lower limb extension. Decorticate posture is the bending of the upper limbs and the extension of the lower limbs.
Because the red nucleus is physically located at the intercollicular level, lesions above it often result in decortication, while lesions below it induce decerebration. Abnormal posture can proceed from decorticate to decerebrate when compression moves from the forebrain and the brain to the brainstem.
Causes of Decorticate Posture:
Decorticate posture frequently denotes issues or injury to certain brain regions. Among the domains it may touch upon are:
The superior midbrain. This region is the uppermost portion of the brainstem, a vital brain structure that connects your spinal cord to the rest of your brain.
The cortex of the brain. This is the outermost layer of the cerebrum, which is wrinkled. The Latin word for “tree bark” is where the word cortex originates. The majority of your brain’s processing and thought processes take place in the cerebral cortex.
The midbrain. Your brain’s central, egg-shaped structure is responsible for relaying impulses between various brain regions. It is one of the key intersections for signals going to and coming from the brain cortex.
The following situations, though they’re not exclusive, can result in decorticate posturing:
- Traumatic brain injuries (TBIs) and concussions.
- Heart Attacks.
- Brain hemorrhages, or cerebral bleeding.
- Cancer and brain tumors, particularly those affecting the brainstem.
- Infections such as encephalitis, meningitis, or extremely severe malaria cases.
- Increase in intracranial pressure or skull pressure.
- Hydrocephalus.
- Cerebral hypoxia.
- Severe drug overdose or alcohol intoxication.
- lead poisoned.
- Reye Syndrome.
- low blood sugar.
- Hepatic encephalopathy.
Risk factors of Decorticate Posturing
Severe brain injury is indicated by decorticate posture. If immediate medical attention is not received, this injury may result in death. If it becomes worse, it could result in erratic posture. When there is a more significant brain injury, a decreased posture happens.
Differential Diagnosis
Normal flexion might resemble decorticate posture, which is sometimes referred to as withdrawal to pain. On the other hand, abnormal flexion is characterized by sluggish, stereotyped motions, whereas normal flexion moves quickly and variably.
Normal flexion is characterized by the wrist being either neutral or extended, the shoulder abducting away from the body, and—most importantly—no lower limb extension. Abnormal flexion causes the wrist to flex with forearm pronation, the shoulder to adduct, and the internal rotation to occur. The lower limbs’ extension is a crucial component.
Extra-pyramidal abnormal posture, or opisthotonus, is observed in cases of cerebral palsy, tetanus, drowning, traumatic brain injury, and poisoning. It’s an odd posture with a sharply arched neck and spine. The disorder known as paratonia, or gegenhalten, is usually caused by encephalopathy or neurological diseases and can also resemble abnormal posing.
Finally, spasticity can occur in people who have had corticospinal tract traumas, such as hemorrhages, tumors, or ischemic strokes. Similar to decorticate posture, flexor muscles often predominate in the upper limb and extensor muscles in the lower limb. The retention of awareness in spastic individuals is the most notable distinction between abnormal posture and spasticity.
Diagnosis
History and Physical
In the early stages after brain trauma, merely characterizing the reaction as either flexion or extension may be adequate, according to Teasdale et al.’s initial work on the Glasgow coma scale. This is because discerning between normal and pathological flexion needs an experienced observer.
Abnormal flexion of the arms with extension of the legs is known as decorticate posture. It entails adduction and internal rotation at the shoulder together with gradual flexion of the elbow, wrist, and fingers. The lower limbs exhibit plantar flexion of the foot, extension of the knee, and internal rotation at the hip. Usually, toes are hyperextended and abducted.
Evaluation
Both decorticate and decerebrate posture are clinical diagnoses, and they should not be seen as independent diagnoses but rather as pathological indicators of neurological damage. Numerous studies may be necessary because of the range of etiologies that might result in these results. As was previously mentioned, surgical intervention for compressive lesions may be beneficial if done quickly.
For this reason, early intracranial imaging, such as CT or MRI, is necessary. Serum and CSF samples are two laboratory techniques that can be used to evaluate other reasons, such as infection and metabolic disruption.
This is a dangerous medical condition that calls for immediate medical attention. A person in this unusual posture may be unconscious, most likely in a coma. Rarely, the physician will admit a patient to the hospital’s critical care unit (ICU), where they begin breathing support and other medical treatments. Occasionally, emergency surgery is also necessary, depending on the patient’s diagnosis and condition. Nevertheless, doctors make this determination after seeing the patient.
In addition to the physical examination of the brain and neurological system, the doctor ordered a few tests to ensure an accurate diagnosis. These tests are as follows:
- MRI or CT scan
- EEG
- Cerebral angiograms
- Puncture of the lumbar region.
Treatment of Decorticate Posture
This unusual posture needs immediate medical attention. The key determinants of treatment are the etiology, the symptoms, and the diagnosis. In situations of extreme severity, patients are sent to an intensive care unit (ICCU), where they receive medical care under 24-hour supervision. The need for emergency surgery may also arise, contingent upon the physician’s recommendation.
The underlying cause is addressed by treatment, such as by treating infections and, where practical, reversing metabolic abnormalities. Removing extra-axial hematomas from TBI patients can increase survival. Since some diseases, including hypoxic brain damage, may not be curable, supporting measures are adopted.
The symptom of decorticate posture cannot be immediately treated. Treating the underlying issue, though, could be feasible.
A person with a decorticate posture may benefit from further treatment in addition to treating the underlying problem. Individuals experiencing this symptom may require supportive care because they are unconscious or in a coma. Mechanical ventilation to assist with breathing is a type of supportive therapy.
The range of therapy choices is due to the large number of potential causes. The best person to advise you on treatment choices and the ones you prefer is a healthcare practitioner.
Physical Therapy Treatment:
The course of physical therapy is determined by the patient’s health and symptoms. Maintaining range of motion in all body joints, reducing stiffness if it exists, frequent positioning when necessary, and regular chest physical therapy are the most typical forms of treatment. If the patient is in a coma, these measures are especially crucial.
Rehabilitation is based on mobility and symptoms if the patient has symptoms associated with paralysis. Frequent exercise aids in the patient’s recovery of motor control and balance. Walking with a stick or other assistance device during gait training.
Is it possible to prevent decorticate posturing?
Decorticate posture has several avoidable reasons. It’s not always feasible to prevent this symptom because some occur randomly or for causes that are not fully understood by professionals. You do, however, have some control over some of the factors that may contribute to decorticate posture.
Actions you can do consist of:
- Take care of your long-term health issues. When it comes to treating chronic diseases such as diabetes, high blood pressure, and epilepsy, heed the advice of your healthcare practitioner.
- When necessary, put on protective gear. Decorticate posture is most frequently caused by head traumas, specifically concussions and traumatic brain injuries. Wearing seat belts and helmets will help prevent injuries to your brain.
- Consume a diet that is balanced. Nutrient deficits and electrolyte imbalances are frequently preventable, or at least less likely to occur. Controlling your diet can also prevent the decorticate posture that is linked to a number of brain disorders, particularly strokes.
- Continue to be physically active and maintain a weight that is appropriate for your body. Conditions that impact your brain can be avoided or delayed depending on your weight and amount of activity. Your healthcare professional can offer guidance on achieving and sustaining a healthy weight for you.
- Refrain from using illegal and non-medical drugs, and consume alcohol-containing drinks in moderation. Decorticate posture may have underlying causes, including substance use problems. keep away from non-medical drugs and substance usage, and always take prescription drugs exactly as prescribed. For males and individuals assigned male at birth (AMAB), moderate alcohol consumption is defined as no more than two drinks per day; for women and individuals assigned female at birth (AFAB), the limit is one drink per day.
- Seek medical attention for infections. Numerous illnesses that impact the brain originate in adjacent areas such as the nose, ears, or eyes. Treating infections in these locations should not be put off. Treating infections early on will help you prevent the spread of disease, which can cause issues like decorticate posture.
Prognosis
With just 37% of decorticated patients and 10% of decerebrate patients surviving after head injuries, abnormal posture is a concerning indicator. The death rate for children who require hospital admission owing to head injuries is generally between 10% and 13%; however, in severe instances with decerebrate posturing, the mortality rate rises to 71%.
Comparable death rates of 68% to 83% in TBI with decerebrate posture have been reported in other studies. Extradural hematoma, admission within 6 hours of damage, and younger patient age were factors that promote survival in TBI with decerebrate posture. Older age and acute subdural hematoma were associated with worse outcomes.
One day after the trauma, abnormal posture or a GCS motor score of less than 4 indicated that there was almost little possibility of independence returning. Individuals who displayed either decorticate or decerebrate stances after receiving a gunshot wound to the head had almost little chance of making a significant recovery. In grades 4 and 5, decerebrate posture is included in the Hunt and Hess subarachnoid hemorrhage severity grading system. They gave death rates of 42% and 77%, respectively.
The etiology, diagnosis, degree of symptoms, age, and other relevant variables all affect the prognosis.
This unusual posture may be a sign of serious nervous system or brain impairment, which can occasionally lead to irreversible brain damage and cause the following symptoms:
- Seizures
- Paralysis
- Inability to speak
- Coma
Complications
Complications include mortality and impaired neurological function, as described under prognosis. In the short term, coma patients may also experience difficulty breathing and managing their cardiorespiratory system.
Usually, decorticate posture indicates severe brain damage or anomalies in brain activity. Without treatment or delay in treatment, many of the disorders that cause it are fatal.
Therapeutic delays may potentially result in long-term damage. The previously regulated talents by the affected portions may be severely degraded or lost altogether when serious injury occurs.
Conclusion
Posturing requires decortication, which renders the person unconscious and in a coma. This symptom is an important indicator of conditions that damage or impede brain function.
Treatment or reversibility is possible for many of the disorders that lead to decorticate posture, particularly those like hypoglycemia. One of the most important elements in deciding the chances of life and recovery is the underlying reason.
However, this symptom does not indicate that there is no possibility of survival or recovery. Modern medical advances have made it possible to cure many neurological issues that might induce decorticate posture. Many of the folks who are currently suffering decorticate posturing have optimism because things are getting better all the time.
Experiencing decorticate posturing in a loved one may be disturbing. This causes unconsciousness and coma in its victims. This symptom is a crucial sign of illnesses that harm the brain or interfere with its normal functions. This symptom does not, however, imply that there is no chance of survival or recovery. Many neurological disorders that might result in decorticate posture can now be treated because of developments in medicine. Many persons with this symptom today and in the future have optimism because the odds are becoming better all the time.
FAQs
What advantages can decortication provide?
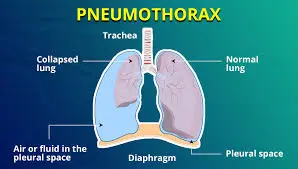
Compared to more conservative therapy, including chest tube drainage plus antibiotics or even intrapleural fibrinolytic, decortication generally speeds up the healing process from a pleural space infection.
What does the term decortication mean?
A type of surgical treatment called decortication is used to remove fibrous tissue that has grown unnaturally on the surface of the diaphragm, chest wall, or lung. The lungs and the chest wall often have a gap between them known as the pleural space, which is coated with a very thin fluid layer for lubrication.
Could you please return from your decerebrate posturing?
When decerebrate posture is present together with hepatic encephalopathy, we should think of it as a possibly reversible finding that might leave the patient without any lasting harm, even though this finding usually prompts contemplation of irreversible problems.
Does decorticate mean stiffness?
Your body may naturally adopt a decerebrate posturing posture if there is a brain injury or disturbance. Another name for it is “decerebrate rigidity.” It may indicate a variety of illnesses, including brain traumas.
Is the posing of decorticates abnormal?
Typically, abnormal posturing reactions to unpleasant stimuli result in decorticate and decerebrate posturing. They entail conventional trunk and extremity motions. It has to be identified and treated very early to prevent the significant morbidity and death that are linked to these disorders.
Which stance is worst, decorticate or decerebrate?
Both postures can be caused by brain injuries in several anatomical locations, however they generally include some degree of brainstem damage. Nonetheless, it is acknowledged that in order to decorticate, an injury must usually be more rostral than in a decerebrate posture.
Decorticate or decerebrate—which comes first?
A very serious disorder known as brain herniation occurs when portions of the brain push through the hard structures inside the skull. Decorticate posture is a symptom of herniation syndrome, a brain herniation. If the illness is not addressed, decerebrate posturing progresses.
Following decorticate posturing, what happens?
Decorticate Posturing’s Risks
It’s possible that the problems underlying your decorticate posture may persist. Chronic symptoms might result from brain injury. You may continue to experience headaches, seizures, paralysis, and other issues even after receiving therapy.
In decorticate, what area of the brain is damaged?
Considering. Damage to the nerve route in the midbrain—the area between the brain and spinal cord—is indicated by decorticate posture. In addition to several other crucial tasks, the midbrain regulates motor activity.
What is a decorticate posture in terms of lesion level?
Decorticate posture, which involves pronating the forearm, and flexion at the elbow with the lower extremities extended and the foot inverted, is the outcome of a UMN lesion above the level of the red nucleus. Conversely, a lesion below the level of the red nucleus but above the level.
Is Decorticate posturing at what score?
Consequently, decorticate posture indicates that the lesion’s extent has not spread below the rubrospinal tract, indicating that the tract’s integrity is intact. A motor score of three is assigned for this type of reaction while evaluating the patient’s Glasgow Coma Scale.
Can you survive the posturing of decorticate?
Decorticate posture is typically linked to a very poor likelihood of survival and is not frequently reversible. It is important that you talk to your loved one’s medical professionals about their prognosis if they have this physical symptom.
What causes the positioning of Decorticates?
Decorticate posture can be caused by
Decorticated posture is caused by a brain-associated ailment, such as brain cancer, stroke, drug use, poisoning, infection, liver failure, and other related brain issues.
What differentiates decorticate from decerebrate?
Decorticate posture is the outcome of injury to the cerebral cortex, especially if that lesion involves damage to the internal capsules. Compared to decerebrate posing, decorticate posturing is more frequent and frequently results in greater survival rates.
What is indicated by decorticate posturing?
Decorticate posture is characterized by a rigid individual holding their legs straight, clenching their fists, and bending their arms. The arms are bent inward toward the body, and the fingers and wrists are resting on the chest. This kind of posturing suggests serious brain damage.
References
- Professional, C. C. M. (n.d.). Decorticate Posturing. Cleveland Clinic. https://my.clevelandclinic.org/health/symptoms/24969-decorticate-posturing
- Knight, J., & Decker, L. C. (2023, July 31). Decerebrate and Decorticate Posturing. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK559135/
- Dhameliya, N. (2022, January 11). Decorticate Posture : Cause, Symptoms, Diagnosis, Treatment, Exercise –. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/decorticate-posture-cause-symptoms-diagnosis-treatment-exercise/
- Physiotherapist, N. P. (2023, December 13). Decorticate Posture : Introduction, Cause, Diagnosis, Treatment. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/decorticate-posture/comment-page-1/



One Comment