Ape Hand Vs Claw Hand
Introduction
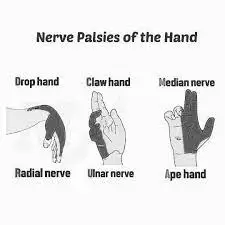
The ape hand and claw hand are two distinct deformities that affect the hand and its functionality. Ape hand deformity, also known as median nerve palsy, occurs due to damage or compression of the median nerve, leading to weakness or paralysis of the thumb’s opposition movement, resembling the hand of an ape.
On the other hand, claw hand deformity typically results from ulnar nerve dysfunction, causing hyperextension of the metacarpophalangeal joints and flexion of the interphalangeal joints, giving the hand a claw-like appearance. Both conditions can significantly impact hand function and require tailored interventions for management.
While their effects on hand function are similar, they differ in their underlying causes and present with different clinical features. This article’s goal is to examine and compare the characteristics, causes, diagnosis, treatments, prognosis, and safety measures related to variations of the Ape and Claw hands.
Ape Hand: Recognizing the Features of Ape
The thumb is positioned closer to the fingers in hand deformity, sometimes referred to as median nerve palsy, which resembles the gripping anatomy of an ape. When disorders like carpal tunnel syndrome occur, the median nerve is compressed or injured, usually near the wrist, resulting in this deformity.
The repositioned thumb has an impact on grip and pinch strength, which can make it harder to perform fine motor skills like buttoning clothes or writing. To evaluate the function of the median nerve, diagnostic techniques include nerve conduction tests and electromyography. Options for treatment vary from conservative methods like physical therapy and splinting to surgical surgery to release pressure on compressed nerves.
Claw Hand: Examining the Unique Elements
The hand appears claw-like due to the deformity known as Claw Hand deformity, which is caused by hyperextension of the metacarpophalangeal joints and flexion of the interphalangeal joints. Like Cubital Tunnel Syndrome or nerve injury at the wrist, this condition is frequently linked to ulnar nerve damage, which typically occurs near the elbow.
Weakened grip strength and difficulty doing tasks requiring exact finger motions can result from Claw Hand. In addition to nerve conduction investigations, the diagnosis process entails a clinical examination that evaluates sensory and motor function in the ulnar nerve distribution. Conservative methods of treatment, such as physical therapy and ergonomic modifications, may be combined with surgical procedures to treat nerve compression or damage.
Causes and Pathophysiology
For accurate diagnosis and treatment of Ape Hand and Claw Hand abnormalities, a greater comprehension of the pathophysiology and underlying causes is essential. The main cause of Ape Hand is compression of the median nerve at the wrist as a result of anatomical abnormalities, injuries, or repeated hand motions.
On the other hand, Claw Hand is caused by damage or compression of the ulnar nerve, which often happens near the wrist or elbow. Hand abnormalities are often caused by injury to the nerve fibers in the affected nerve distribution that are important for motor and sensory function.
Diagnosis and Evaluation
Determining the underlying cause of hand abnormalities and making treatment recommendations depend on an accurate diagnosis. Diagnostic procedures for Ape Hand may involve nerve conduction investigations, electromyography, and physical examination techniques to measure hand strength and thumb location and assess median nerve function.
In Claw Hand, nerve conduction investigations are necessary to determine nerve involvement and serve an important role in evaluating motor and sensory function in the ulnar nerve distribution.
Methods of Treatment
The underlying cause and degree of Ape Hand and Claw Hand abnormalities determine the treatment plan. Conservative treatment techniques including splinting, physical therapy, and ergonomic modifications can, on the one hand, help reduce discomfort and enhance hand function. Surgical intervention, such as carpal tunnel release, may be necessary in cases of severe median nerve compression.
Similarly, Claw Hand treatment may involve conservative measures such as physical therapy and ergonomic adaptations to improve hand function and prevent further nerve compression. Surgical intervention may be indicated to address ulnar nerve compression or injury, such as ulnar nerve transfer position or decompression procedures.
Methods of Treatment
The underlying cause and degree of Ape Hand and Claw Hand abnormalities determine the treatment plan. Conservative treatment techniques including splinting, physical therapy, and ergonomic modifications can, on the one hand, help reduce discomfort and maintain hand function. Surgical intervention, such as carpal tunnel release, may be necessary in cases of severe median nerve compression.
Similarly, Claw Hand treatment may involve conservative measures such as physical therapy and ergonomic adaptations to improve hand function and prevent further nerve compression. Surgical intervention may be indicated to address ulnar nerve compression or injury, such as ulnar nerve transposition or decompression procedures.
The cause of median nerve damage largely determines how the lesion is treated. Splints might be applied in this deformity situation.
- Conservative treatment.
- Surgical treatment.
- Physical therapy treatment
- Conservative treatment
- anti-inflammatory medications to treat pain.
- The purpose of manual treatment techniques is to improve thumb mobility.
- avoiding the activities that cause your thumb to hurt or get stressed.
- Use heat therapy or ice massage.
- Using dynamic splints is recommended to allow thumb mobility.
Surgical Treatment
Depending on how severe the deformity is, surgery can be necessary. The hand’s affected portion functions better after the procedure. Surgical care might include:
- Nerve decompression
- Nerve repair
- Nerve graft
- Surgery to transplant a tendon is recommended if nerve repair is not carried out. Tendon transfers remove excess tendons from other hand or forearm regions to restore a function that was compromised by the nerve lesion.
Physical Therapy Treatment
The objective of physical therapy care is:
- regain the strength of your muscles.
- Boost the performance of your muscles.
- Increase the impacted area’s sensitivity.
- Reduce the discomfort.
- It aids in restoring muscular strength while braces and splints (C-splints) aid in the healing process.
Finger Stretch
- Stretch your hands with this exercise to help relieve discomfort and improve hand range of motion.
- Place the hand on a tabletop or other level surface, palm down.
- Without straining the joints, slowly extend your fingers so they are as flat on the surface as possible.
- Release after thirty to fifty seconds of holding.
- Repeat with each hand for a minimum of four more times.
Grip Strengthener
- Certain tasks, such as keeping objects in place without dropping them and turning knobs on doors, can be made simpler with this practice.
- Squeeze as hard as you can on a softball in your hand.
- After a brief period of holding, release.
- Using both hands, repeat five to ten times.
- Two or three times a week, perform this exercise; however, allow the hand to rest for 48 hours in between.
- This exercise should not be performed if you have any thumb joint injuries.
Pinch Strengthener
- This motion strengthens the thumb and finger muscles.
- It can make tasks like using the petrol pump, opening food packages, and turning keys easier for the individual.
- Place a soft foam ball or putty between the thumb and the tips of your fingers. For 20 to 40 seconds, hold.
- Repeat with both hands ten to fifteen more times.
- Do this exercise two or three times a week, allowing your hands to rest for 48 hours in between.
- Try not to perform this workout if you have any thumb joint injuries.
Thumb Extension
- If your thumb muscles are stronger, it will be simpler for you to pick up and carry heavy things, such as bottles and cans.
- Lay the hand down flat on a surface. Encircle the hand at the base of the finger joints with a rubber band.
- As far as possible, slide the thumb gently away from the fingers.
- Release after 20 to 40 seconds of holding.
- Ten to fifteen repetitions for each hand.
- You may perform this exercise two or three times each week, but give your hands a 48-hour break in between sets.
Thumb Flex
- The thumbs’ range of motion is aided by this action.
- Start by holding out your hand palm up in front of you.
- As much as possible, extend the thumb apart from the other digits.
- Next, bend the thumb such that it contacts the tiny finger’s base by bending it across the palm.
- For 20 to 40 seconds, hold.
- Make sure you repeat each thumb at least four times.
Thumb Touch
- This exercise helps the thumbs have more range of motion, which is beneficial for tasks like picking up the toothbrush, fork, spoon, and writing pens.
- Straighten your wrist as you hold out your hand in front of you.
- Form an “O” with the thumb and each of the four fingertips by slowly touching them one at a time.
- Maintain each rep for 30 to 40 seconds.
- Continue doing it on each hand for a minimum of four to five times.
Thumb Stretches
- Regarding the thumb joints, perform these two stretches:
- With the palm facing you, extend your hand.
- Bend the thumb tip slightly in the direction of the index finger’s base.
- For 20 to 30 seconds, hold. Let go and do it four or five more times.
- With the palm facing you, extend your hand.
- Utilizing only the lower thumb joint, slowly extend the thumb across the palm.
- About 20 to 40 seconds, maintain.
- Let go and repeat an additional four times.
Play With Clay
- A better technique to increase finger range of motion and strengthen hands simultaneously is to play with clay or putty.
- It won’t even feel like physical activity.
- Compress the clay into a ball, roll it into long “snakes” using your hands, or make the spikes on a dinosaur with your fingertips, following the children’s example.
Hot and Cold therapy
It aids in improving sensitivity while reducing pain and inflammation.
Electrical modality
- To excite the muscles of the opponent, therapists first use Ig current electrical stimulation to the thenar muscles.
- The transition to the SF current, which aids in muscle strengthening, then happens gradually.
Prognosis and Considerations
The prognosis for individuals with Ape Hand or Claw Hand deformities depends on various factors, including the extent of nerve damage, the success of treatment interventions, and adherence to preventive measures.
With prompt diagnosis and appropriate treatment, many individuals can experience improvement in hand function and quality of life. However, severe or untreated cases may lead to long-term disability and functional limitations. Healthcare providers should consider the individual’s specific needs and circumstances when developing a treatment plan and providing ongoing care.
Preventive Measures
While some hand deformities are unavoidable, implementing preventive measures can help reduce the risk of developing Ape Hand or Claw Hand. In occupations or activities that involve repetitive hand movements or prolonged pressure on the median or ulnar nerves, ergonomic considerations and lifestyle modifications are essential.
These may include using ergonomic tools and equipment, taking regular breaks, and practicing proper hand and wrist positioning during activities. Additionally, maintaining overall hand and wrist health through exercises, stretching, and avoiding excessive force or strain can help prevent nerve compression and related hand deformities.
Ape Hand Vs Claw Hand Comparison
| Feature | Ape Hand | Claw Hand |
| Thumb Positioning | Ape-like grip, closer to the fingers | Pay attention to the hyperextension of other fingers; the thumb is unaffected. |
| Associated Nerve Damage | Injury to the median nerve (such as carpal tunnel syndrome) | Injury to the ulnar nerve (ulnar nerve palsy) |
| Characteristics | Thumb in line with fingers, consistent look | Flexion of the interphalangeal joints and hyperextension of the metacarpophalangeal joints, resulting in the formation of a claw-like form |
| Causes | Carpal tunnel syndrome, median nerve compression | Ulnar nerve compression, trauma, or injury |
| Functional Implications | Having trouble with precise activities and fine motor skills | Reduced grip force and difficulties performing precise tasks |
| Common Conditions | Problems with the median nerve and carpal tunnel syndrome | Cubital Tunnel Syndrome and Ulnar nerve palsy |
| Treatment Approaches | Splinting, physical therapy, and surgical procedures | Treating underlying nerve injury, undergoing surgery, and physical therapy |
| Diagnostic Methods | Research on nerve conduction, electromyography (EMG) | Research on nerve conduction and clinical assessment |
| Sensory Symptoms | In the distribution of the median nerve, numbness and tingling | The hand resembles an ape with a unique thumb placement |
| Motor Symptoms | Deficit in thumb and finger strength | Hand strength weakness and poor finger coordination |
| Clinical Presentation | The hand resembles to an ape with a unique thumb placement | The hand resembles an ape with a unique thumb placement |
| Prognosis | Varies, based on the success of the therapy and the underlying reason | Varies, depending on the degree of nerve injury and the effectiveness of the intervention |
| Rehabilitation Focus | Exercises for hand-thumb coordination and ergonomic modifications | Exercises for finger range of motion and grip strength |
| Preventive Measures | Positioning hands ergonomically to prevent repeated strain on the median nerve | Ergonomic changes to prevent prolonged pressure on the ulnar nerve |
Complications
- Because of how the extensor hood mechanism is balanced differently after intrinsic tendon transfers than after adductor plasty, more difficulties occur.
- If there is not enough strength or excursion in the selected muscle, the transfer might not be appropriate. A further problem with extension arises while placing the transfer into the lateral bands of the extensor covering.
- Insufficient tendon transfers can be addressed by a strengthening program to build up the muscle, but they frequently need to be surgically corrected.
- If the selected muscle has too much strength or is too brief of an excursion, the transfer might not be appropriate either.
- Excessively tight stitching of the transfer into the lateral band may result in a swan-neck deformity in the finger.
- Passive range of motion treatment can be used to address tendon transfers that are either excessively tight or too strong to facilitate flexibility.
Conclusion
Ape Hand and Claw Hand deformities may share similarities in their impact on hand function, but their underlying causes, clinical presentations, and treatment approaches differ significantly. By understanding the distinct characteristics of each condition and understanding treatment interventions accordingly, healthcare professionals can provide optimal care and improve outcomes for individuals affected by these hand deformities.
Early diagnosis, proper treatment, and preventive measures are key to minimizing disability and maximizing hand function in individuals with Ape Hand and Claw Hand deformities.
FAQs
What is ape hand deformity?
The disorder known as ape hand deformity causes the thumb to become permanently twisted and adducted, impairing its ability to move accordingly. Damage to the distal median nerve, which supplies the thumb’s controlling muscles, is the reason for this deformity.
What is the ape hand deformity also known as?
Typically adducted as well as rotated, the thumb is called an “ape-like hand.” The “pointing finger” deformity results from paralysis of the flexor digitorum superficialis, which damages the median nerve in the mid-forearm.
What is the other name for a claw hand deformity?
Your fingers will bend in towards your wrist when you have a claw hand. It may also be known as ulnar nerve palsy. Additionally, it may make it difficult or impossible for you to straighten every finger. The word “claw hand” refers to this stuck-in position when your hand is clenched into a claw form.
What is the clinical anatomy of claw hands?
The 4th and 5th fingers’ proximal and distal interphalangeal joints exhibit flexion, whereas the metacarpophalangeal joints exhibit hyperextension in a claw hand. Patients with this disorder can create a fist, but when they spread their fingers, it’s known as a claw hand.
References
- What Is Ape Hand and What Causes It? Healthline. https://www.healthline.com/health/ape-hand#vs-claw-hand
- Ape Hand. (n.d.). Physiopedia. https://www.physio-pedia.com/Ape_Hand
- Ape Hand Deformity – Cause, Symptoms, Treatment, Exercise. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/ape-hand-deformity/
- Claw Hand. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK507781/